
Calcium &
Phosphorous
and related disorders

Objectives
1. distribution
S
& forms
2
. Homeostasis of blood Ca and
inorganic phosphate PO4- -
3
. hypercalcaemia
&hypocalcaemia

Ca
is one of the predominant cation
element in human body;
1 Kg in 70
Kg
human
body.
99
%
in
skeletal=bone
˂1
%
intracellular
= 0.1 % in the extracellular(in blood).
Ca
in blood: ͌
50% ionized Ca(Ca +2) or
[Ca+2]
,
͌ 40 % protein bound mainly
albumin,
͌
10 % to other anion;
oxalate, citrate…. etc.
The biologically and metabolically active
form is the
Free or ionized Ca[Ca +2].
Total Ca= Ca bound+ Free Ca
So measurement of serum Ca is affected
by serum protein and also by PH.
Conditions
that
increased
serum
protein(oral contraceptive, estrogen …)
will also increased total Ca,
while
decreased serum protein(chronic liver
disease, nephrotic syndrome
….) will
decreased the total Ca
,
But
In these conditions
Free Ca
is
normal
(not change), and no need for
treatment.

Homeostasis of Ca &
PO4- -
Mean
S
the regulation of blood Ca and
PO4- -. This need for normal organs:
1.Bone
2.
Kidney
3.
GIT.
Also for normal factors: 1. Parathyroid
hormone PTH
2. active vitamin D 1,25
Dihydroxycholecalciferol(1,25 DOH D3).
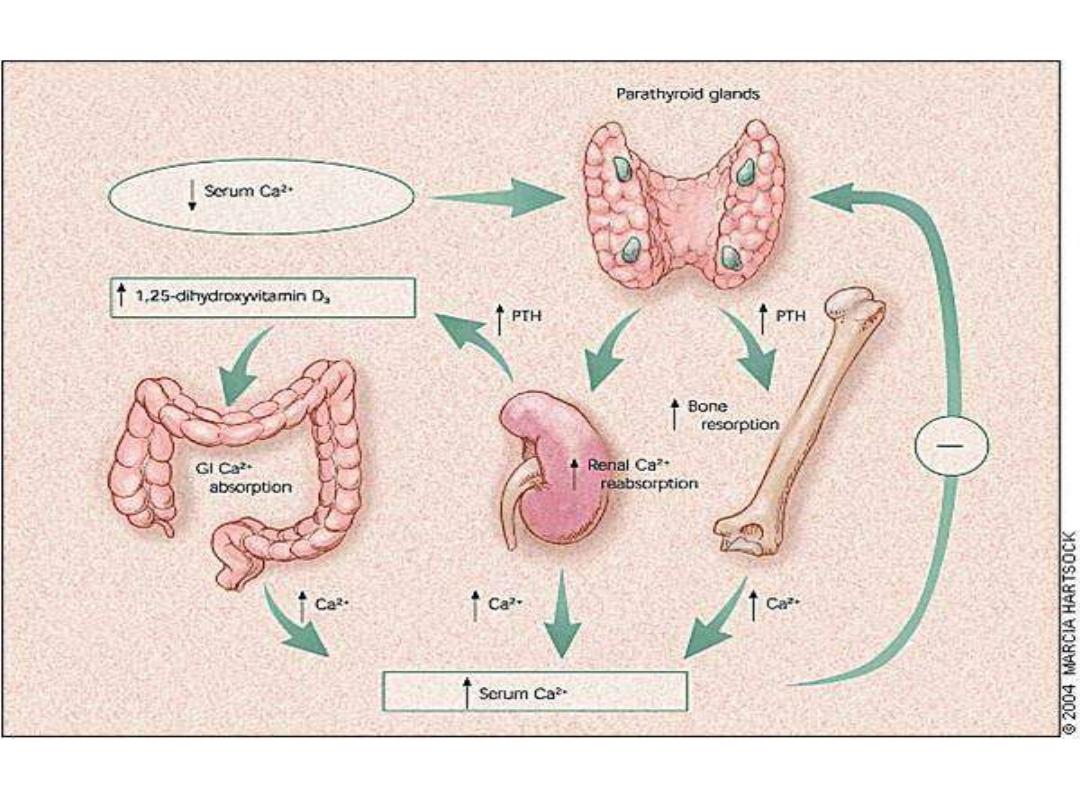

Low circulating serum calcium
concentrations
stimulate the parathyroid glands to secrete
PTH, which mobilizes calcium from bones by
osteoclastic stimulation. PTH also stimulates
the kidneys to reabsorb calcium and to convert
25-hydroxyvitamin D3 (produced in the liver) to
the
active
form,
1,25-dihydroxyvitamin D3, which stimulates GI
calcium
absorption.
High
serum
calcium
concentrations
have a negative feedback effect
on
PTH
secretion.

PTH
action
*
Renal
effects (steady state maintenance)
-Inhibition
of
phosphate
transport
-Increased
reabsorption
of
calcium
-Stimulation of 25(OH)D-1alpha-hydroxylase
*
Bone
effects (immediate control of blood
Ca)
-Causes calcium bone release within minutes
-Chronic elevation increases bone remodeling
and
increased
osteoclast-mediated
bone
resorption
-However, PTH administered intermittently has
been shown to increase bone formation and
this is a potential new therapy for osteoporosis

PTH → synthesis of 1,25 DOH vit. D3( by
stimulation
of
renal
1α
hydroxylase).
PTH→
↑
serum
Free
Ca
levels:
1.PTH→ ↑GIT absorption of Ca and PO4 - -(in
conjunction with active D3)
2. ↑bone
resorption of Ca and PO4 - -(in conjunction with
active D3).
3. ↑renal reabsorption of Ca and
excretion
of
PO4
ion.
The net action
of PTH in the presence of
normal
kidney
function(normal
urea
&
creatinine)
:
Increased
serum
free
Ca
&
decreased
serum
PO4
ion.

Active vit. D3 increased both of serum Ca &
PO4- -(from bone & GIT), this also in the
presence
of
normal
kidney
function.
Note: vit D2 ergosterol is plant source, D3 is
animal
origin.
Cholecalciferol(vit.D3), and 25 OH D3 both are
biologically inactive . The only active one is
1,25 DOH D3, which need
for normal
metabolism by liver and kidney. Anticonvulsant
drugs convert 25 OHD3→24,25DOHD3, the
inactive form. Kidney failure leads to lack of 1α
hydroxylase and →absence of 1,25 DOHD3.