Chest Lectures
Pr. Dr.Waleed Mustafa
Consultant Thoracic & Vascular SurgeonObjectives
The students should know the followings:-1-Surgical anatomy of the chest wall , lung ,pleura and mediastinum .
2-Diseases affecting pleura (From surgical point of view ) .
3-Indications , contraindications and complications of bronchoscopy .
4-Chest trauma -----indications for surgery
5-Indications , contraindications , technique and complications of chest tube thoracostomy .
6-Hydatid disease in Iraq .
7-Surgery in bronchiectasis , lung abscess and TB.
8-Carcinoma of the bronchus aetiology , presentation , investigations and modalities of treatment
9-Chest wall deformities .
10-Thoracoscopy indications and complications .
Anatomy
The respiratory system consists of the :
Nose , Nasal passage , Nasopharynx , larynx ,Trachea ,Bronchi & lungs . The chest wall is covered by Pectoralis muscle anteriorly while posteriorly both (Latissmus dorsi and serratus muscle) are encountered .
There are (12) pairs of ribs ,
Seven of which are termed (True Ribs) as the cartilages articulate with the sternum.
The lower five ribs are termed (False Ribs) which are not connected directly to the sternum.
The eleventh and the twelfth ribs are termed (Floating Ribs )
Because they are not attached anteriorly .
The sternum is divided into the Manubrium .Body and xiphoid . The clavicle articulates with the sternum and Ist.costal cartilage .Muscles associated with the intercostals space are , The external intercostals ,internal intercostals and transversus thoracic(inner most intercostal) muscles .There are (11) intercostals spaces containing a vein ,an artery and a nerve which course along the lower edge of each rib .

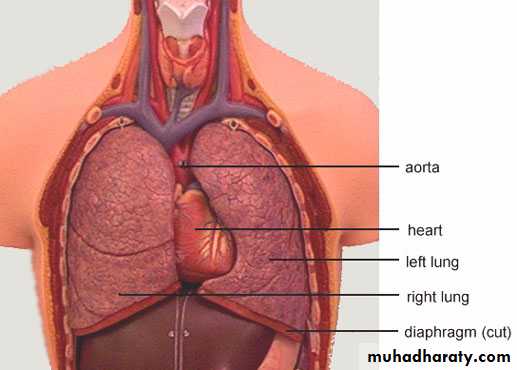
• Pleura is a fibro elastic membrane lines by squamous epithelial cells .It consists of two portions:-1-Parietal pleura which lines the thoracic cavity and it is divided into four parts a- Costal pleura which lies against the ribs &intercostal muscles b-Diaphragmatic pleura which covers the upper surface of the diaphragm.C-Mediastinal pleura which lies against the mediastinum .D-Cervical pleura which covers the dome of the thoracic space 2-Visceral pleura which intimately invests the lung .
• Costo –phrenic angle is the angle between the costal &diaphragmatic pleura.
• Cardio –phrenic angle is the angle between the heart &diaphragmatic pleura
• Inferior pulmonary ligament is the anterior & posterior reflection of the pleura between the root of the lung & the diaphragmatic surface
The function of the pleura is to maintain the environment of the pleural space in which the lung is function.
The bronchial arteries originate from the aorta or the intercostals arteries . Pulmonary veins drain into the left atrium .No bronchial veins. The Lymph nodes found along the lobar branches are termed(hilar LN).There are also Tracheal and tracheo-bronchial LN.Phrenic nerve located anteriorly while the vagus nerve located posteriorly in the thoracic cavity .

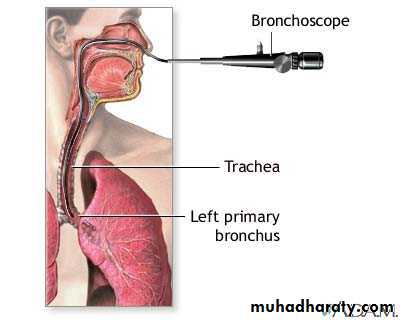
The Trachea is a fibro muscular tube (10-12 cm) in length and (13-22 mm) in width. Supported laterally and ventrally by (16-22) U-shaped hyaline cartilages . The trachea originates at the level of the cricoid cartilage down to its bifurcation at the level of the sternal angle where it divided into right and left main bronchi .The spur at the bifurcation is termed the (Carina) . The right main bronchus is (12-16 mm) in diameter ,the left is ( 10-16 mm) in diameter .The right main bronchus deviates less from the axis of trachea than the left ,this explains why foreign body is more common in the right main bronchus .The main bronchi are divided into the segmental bronchi which end into the terminal bronchiole which divided into the respiratory bronchiole which terminate into the alveoli .
Clinical manifestations of respiratory dieases
1-Cough2-Dyspnea or breathlessness , it is an unpleasant subjective awareness of the sensation of breathing .
3-Chest pain in diseases with pleural or chest wall involvement .
4-Haemoptysis .
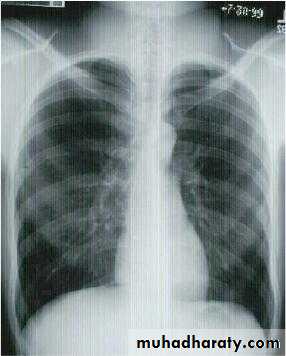
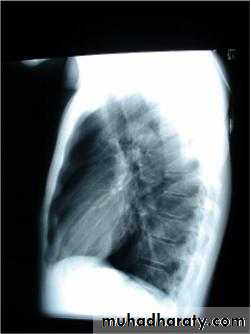
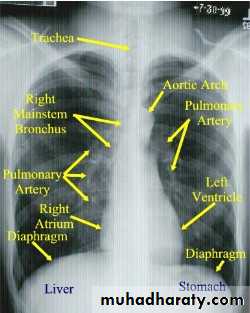
Investigations :-
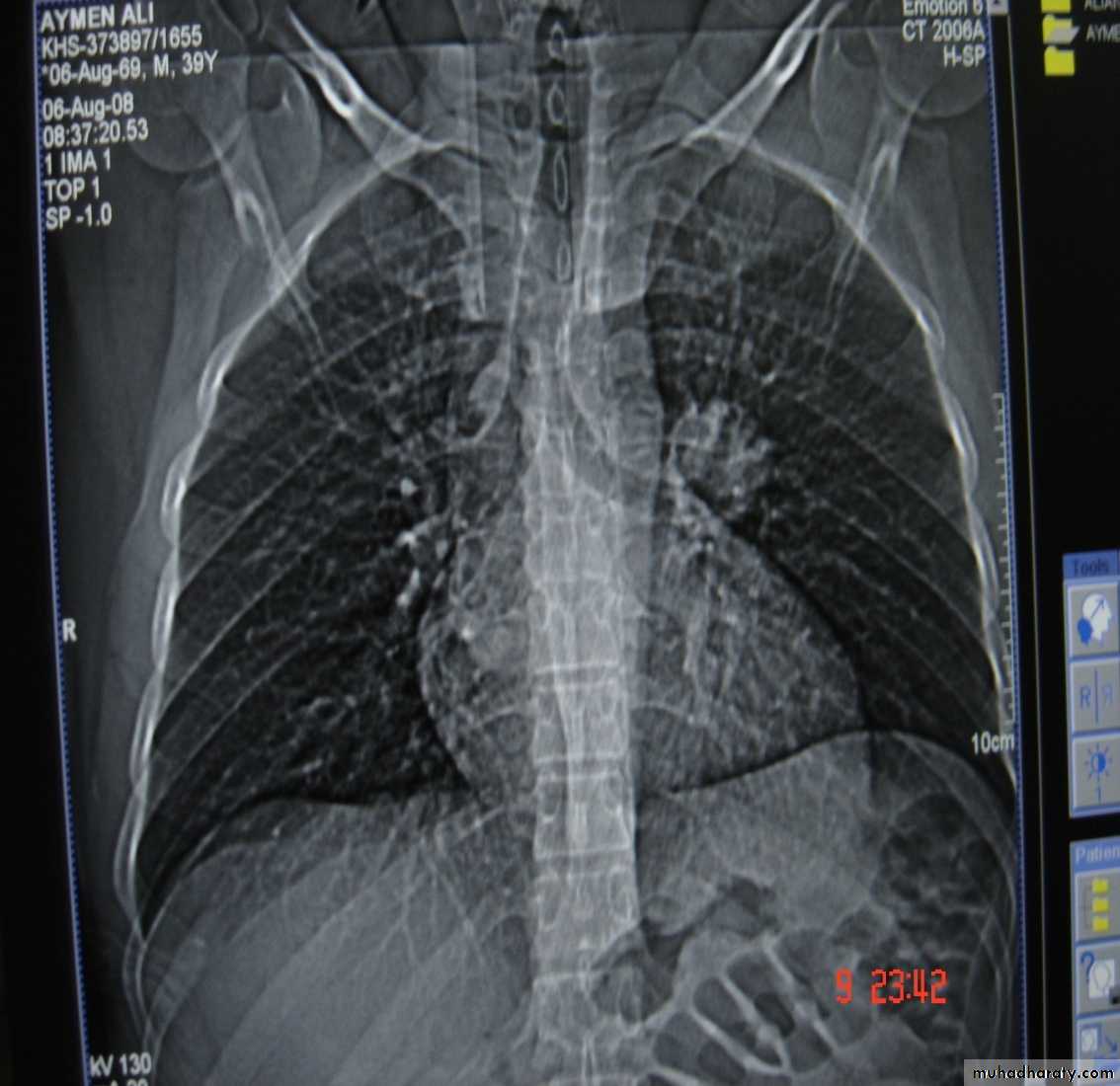
1-Chest X-Ray2-CT chest
3-MRI mediastinum
4-US chest to detect any effusion .
5-Pleural aspiration .
6-Bronchoscopy flexible or rigid .
Pulmonary Function Tests
1-Tidal Volume (TV)
Is the amount of air inspired or expired per single breath .
2-Functional residual Capacity (FRC)
The amount of gas contained in the lung at the end of quiet expiration .
3-Inspiratory reserve volume;-
Is reached when the patient makes a maximum inspiration and increased the lung volume ,compared with that contained at the peak tidal volume.
4-Vital capacity :-
The volume expired from maximal inspiration to maximal expiration.
5-residual volume :-
Is the amount of air remaining in the lung after maximal expiration.
8—FEV1
Is the volume of air expired in one second .
Diseases of the pleura
• 1-Spontaneous pneumothorax
Is the accumulation of air inside the pleural cavity , occurring without any known etiology .More in males ,more on the right side .It can be bilateral
• Causes 1- Ruptured pulmonary bleb.2-Ruptured of a cystic defect in the pleura.3-Teared visceral pleura 4-No cause can be demonstrated in (15-20%).Complications:-1-pleural effusion2-empyema 3-tension pneumothorax which leads to mediastinal shift &circulatory collapse.4-Respiratory failure in elderly patient with COAD (COPD) .
• Treatment :-
• 1-Bed rest ,O2 administration &observation in limited pneumothorax.
• 2-Aspiration
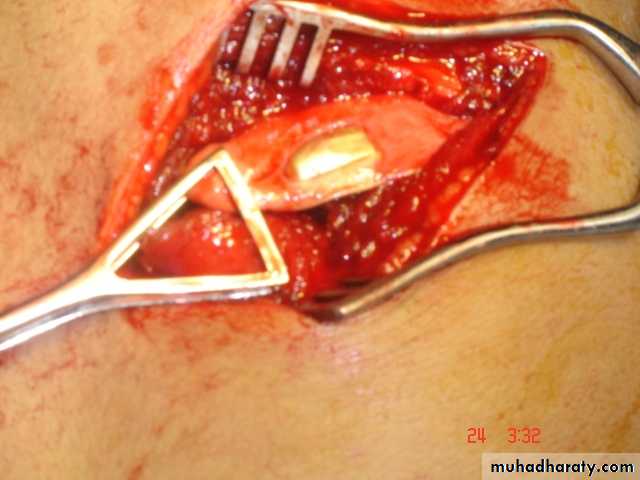
• 3-Chest tube (thoracostomy tube or ICD intercostal drain in a safety triangle which is bounded by pectoralis muscle anteriorly &lattismus muscle posteriorly and the superior border of the nipple.in the fifth intercostal space just anterior to the mid axillary line to avoid the long thoracic nerve .
• 4-bronchoscopy is indicated if the lung fail to expand
• 5-Chemical pleurodesis.by injecting sclerosing agent as Tetra cycline
• 6-Surgery pleurectomy by thoracotomy or thoracoscopically if the lung fail to re expand
• 2-Spontaneous haemothorax
• Is the presence of blood inside the pleural cavity• Causes:-
• 1-pulmonary causes ----------TB , AV malformation
• 2-pleural causes -----------torn vascular adhesion
• 3-pulmonary malignancy ….primary or metastatic
• 4-blood dyscrasia ……………..hemophilia
• 5-abdomina; pathology haemo peritoneum
• 6-thoracic causes ………ruptured great vessels
• Clinical featuresdyspnea , chest pain ,syncopesigns of hypovolaemic shock blood inside the pleural cavity may leads to deposition of fibrin on the pleural surface leading to fibrosis (trapped lung syndrome) .
• Treatment
• 1-Resuscitation
• 2-Tube thoracostomy
• 3-May needs thoracotomy if excessive bleeding
• initial bleeding more than 1.5 liter
• Or continuous bleeding more than 200 ml/hour for more than 4 hours
• 3-Chylo –thorax
• Is the presence of lymph in the pleural space• Causes
• A-Congenital atresia of the thoracic duct , birth trauma
• B-Traumatic
• C-Neoplastic malignancy
• D-Infection TB
• Diagnosis milky pleural effusion that does not clot and contains fat , fat soluble vitamins & antibodies
• Treatment
• 1-Conservative consists of insertion of tube thoracostomy to drain the effusion , correction of the fluid and electrolytes with nutritional supplement.
• 2-Surgery consists of ligation of the thoracic duct if the effusion continues for more than two weeks .
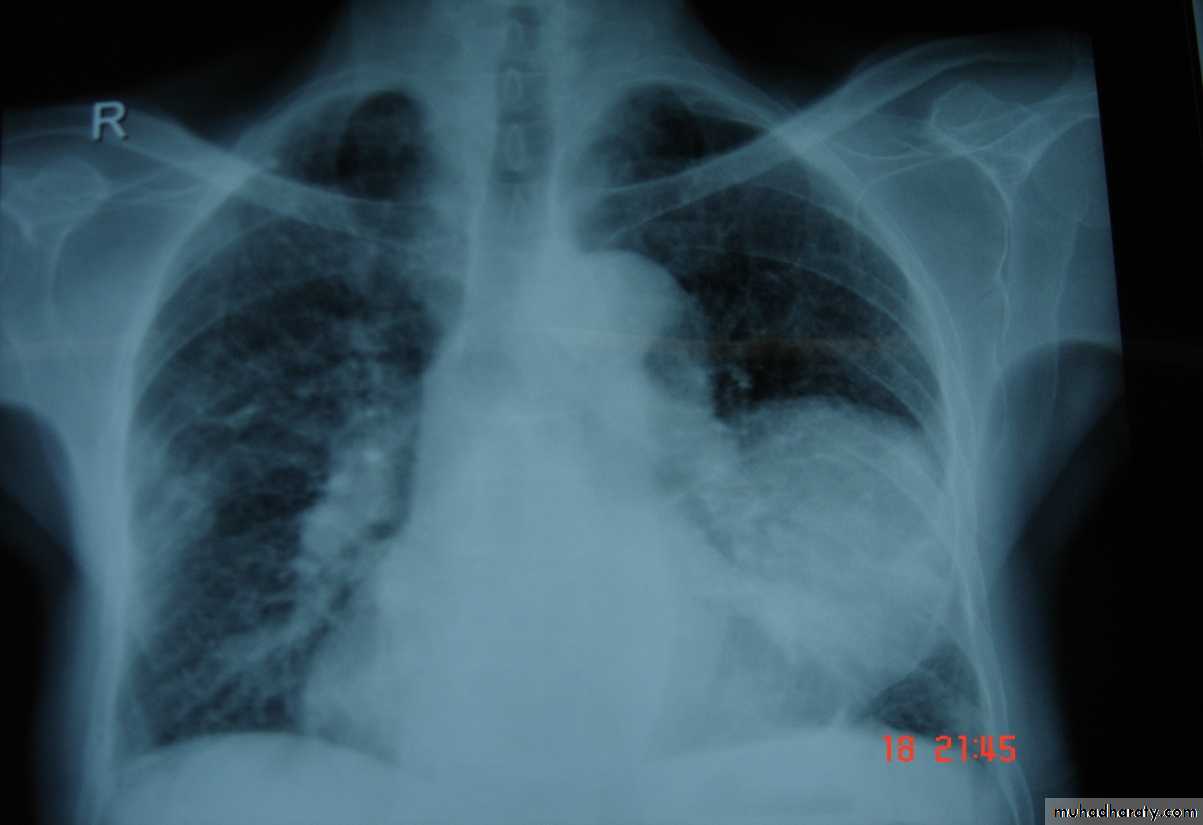
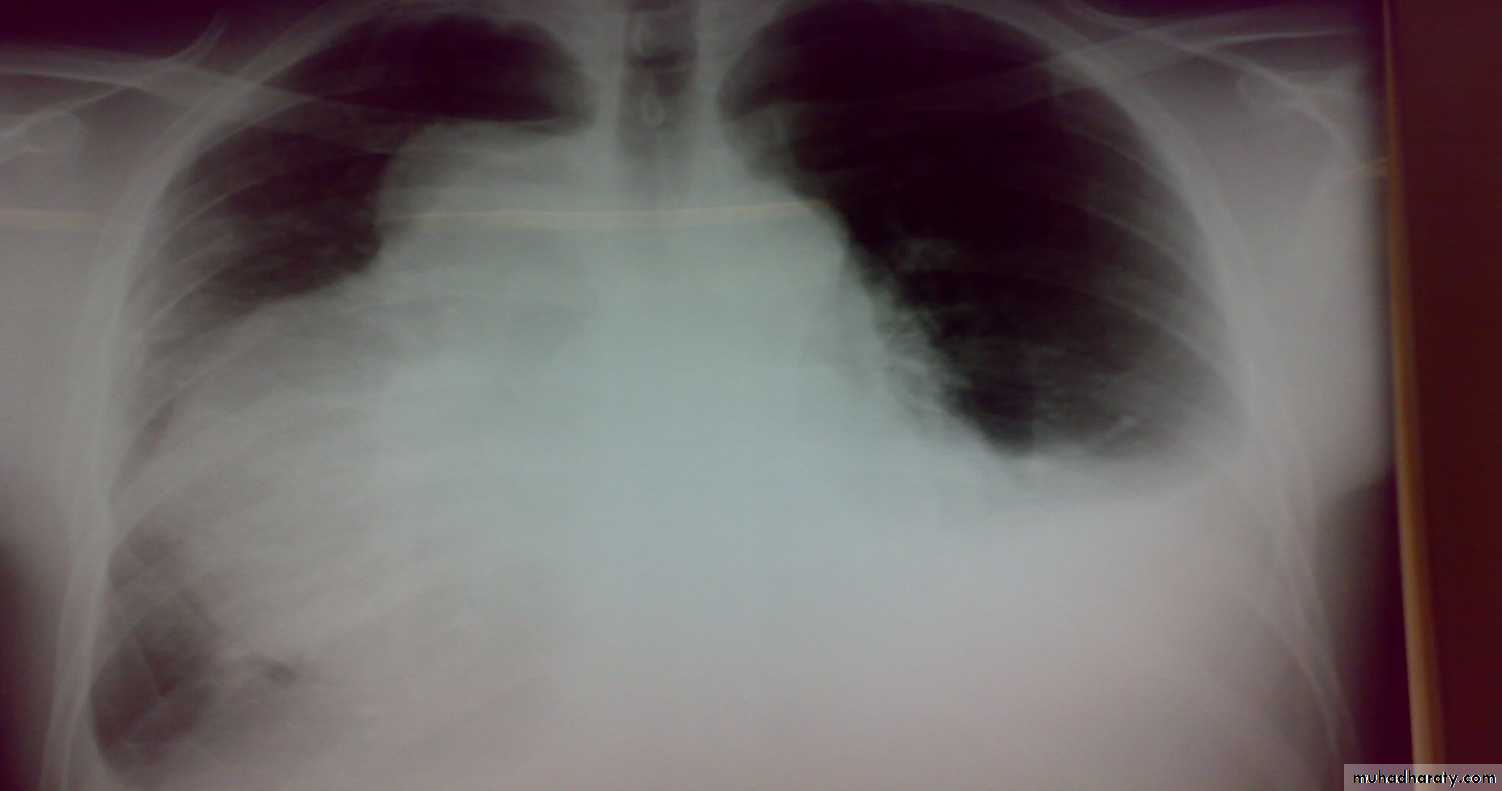
• 4-Pleural effusion

• Is the accumulation of fluid in the pleural space excessive transudation or exudation of the interstitial fluid from the pleural surface. It is signify pleural or systemic disease .
• Its effect depends on its size (mild , moderate or massive ) & the state of the underlying lung .It is classified as transudate when the protein content is less than 3g% or exudates when protein content is more than 3 gm % .Clinically patients will present with dyspnea & pleuritic chest pain
• Radio logically (concave meniscus sign)
• Transudate as in CHF
• Exudate as in malignancy
• Treatment :-1-aspiration (thoracentesis) 2-tube thoracostomy
• 3-chemical pleurodesis 4-pleuectomy to remove the pleura to stop the effusion.
• 5-Empyaema

• Is the accumulation of pus in the pleural space , it passes into three stages
• 1-Acute phase with the clinical manifestation of fever & toxicity .• 2-Transitional phase with the increased turbidity of the fluid & decrease the size of the lung .
• 3-Chronic phase with the pleural thickening ,decrease amount of the fluid & the development of the trapped lung syndrome .
• Tube Thoracostomy Tube thoracostomy or Chest Tube or ICD(Intercostal drain) Is a flexible hollow plastic tube that is inserted through the chest wall into the pleural space and connected to a bedside drainage container
• Indications:-
• 1-Pnemothorax
• 2-Pleural Effusion This effusion may be A-Empyema

• 2-Hemothorax Traumatic or Malignant Effusion

• 3-Hydro thorax 4-Chylothorax 5-Thoracic Operation (Tube Thoracostomy without trocar ) .On the lung or Mediastinum Or The esophagus 6-Postoperative (Collection or Infected space ).7-malignant Effusion drainage and giving medication through it.

• Contra-Indications:-Refractory coagulopathy Lack of cooperation by the patientDiaphragmatic Hernia Lobar EmphysemaSurgical Emphysema without underlying pneumothorax
• Technique:-
• LA or GA
• Surgical Set
• The tube may be inserted in the Emergency Dept. , ICU ,Operating Room or General Hospital Room
• Size infantile , pediatric ,adult (8 FG ------ 40 FG)
• Roughly ---- the size of adult index finger
• Sites ----
• Safe zone
• The free end of the tube ------underwater seal below the level of the chest
• Chest radiograph to be taken to check the location of the drain
• The tube stays in for as long as there is air or fluid











• How long is a chest tube used ?The tube remains in place until the lung is re-expand or the fluid is drained. Occasionally the patient require more than one chest tube Indications for Removal Clinical Mechanical Radiological
• Complications:-1-Minor Complications:-Severe pain during placement Subcutaneous hematoma or seroma Anxiety Shortness of breath (Dyspnea) Cough ( Rapid drainage of fluid )
• 2-Major Complications Hemorrhage ---haemothorax or haemoptysis Infection Reexpansion pulmonary edema Injury to the liver , spleen , diaphragm .Injury to the Thoracic aorta & the heart

Bronchoscopy
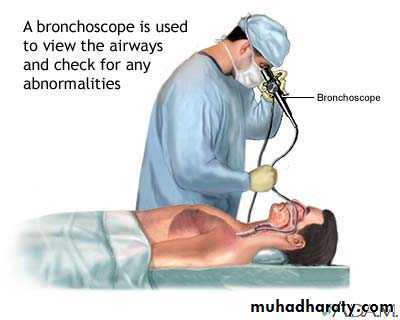
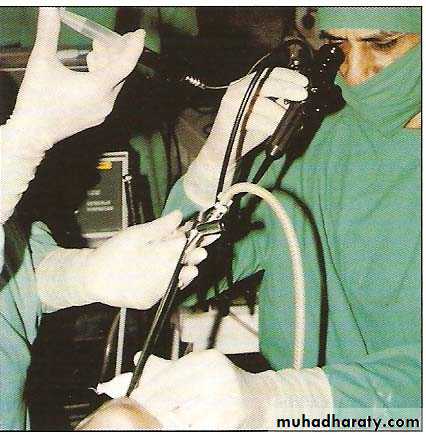
Bronchoscopy Looking into the living lungs (Chevalier Jackson 1928)Today with the major advance in technology View the fine details of the end bronchial anatomy Diagnosis of the disease Treating diseases It is the visualization of the air way using either rigid Bronchoscope (GA) or the flexible (Fiber optic Bronchoscope ) (LA) or both simultaneously .Through which we can remove FB , take BAL , brushing lesions &Trans bronchial Biopsy .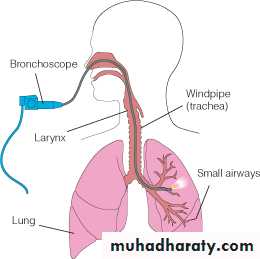
HISTORY
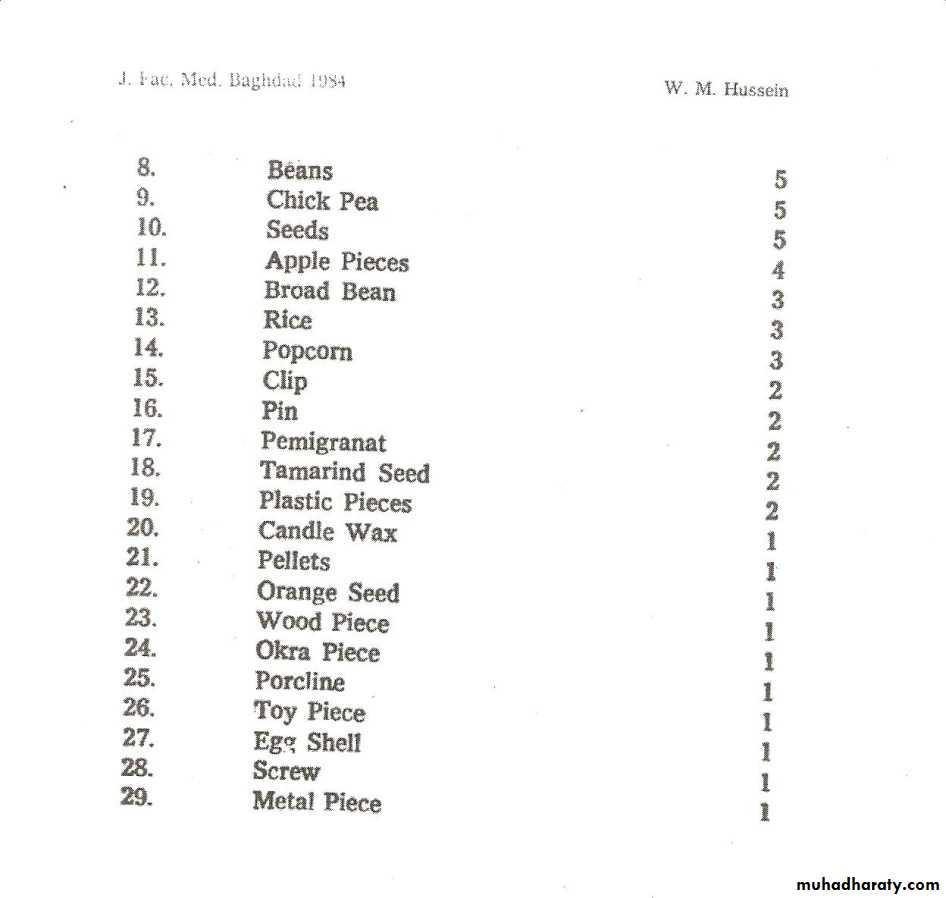
• Gustav Killian in 1897 succeeded in removing aspirated pork bone from the bronchus of a 63 –year-old farmer under cocaine anesthesia .He used external light source , a head mirror , esophagoscope and forceps to remove the bone .• He became famous & his clinic attracted patients from far and wide for his expertise in removing different kind of (FB) such as bones ,beans ,buttons ,coins & tin whistle .
Gustav Killian (The father of bronchoscopy ) , was appointed professor
of ENT at the university of Freiburg in 1892 .
Gustav Killian Bronchoscope , external light source
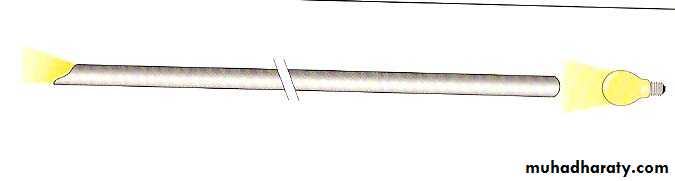
Bronchoscopy rapidly developed into a science (with the creation of a better instruments and techniques )Chevalier Jackson Founded philadelphia school of bronchoesophalogology Jackson‘s monograph first published in 1950
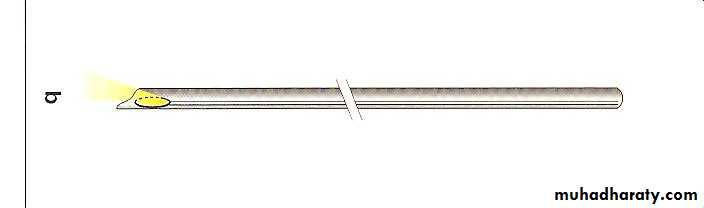
Chevalier Jackson’s Bronchoscope with a small distal bulb & built –in suction tube
• H.H.Hopkins English physicist developed the rod-lens optical telescopes which could be used with the rigid bronchoscope
Early in the 1960s Shigeto Ikeda devised a means to replace the small electric bulb with glass fibers capable of transmitting brighter light from an outside source. He presented the first flexible bronchoscope at the 1966 International Congress on Diseases of the Chest in Copenhagen.

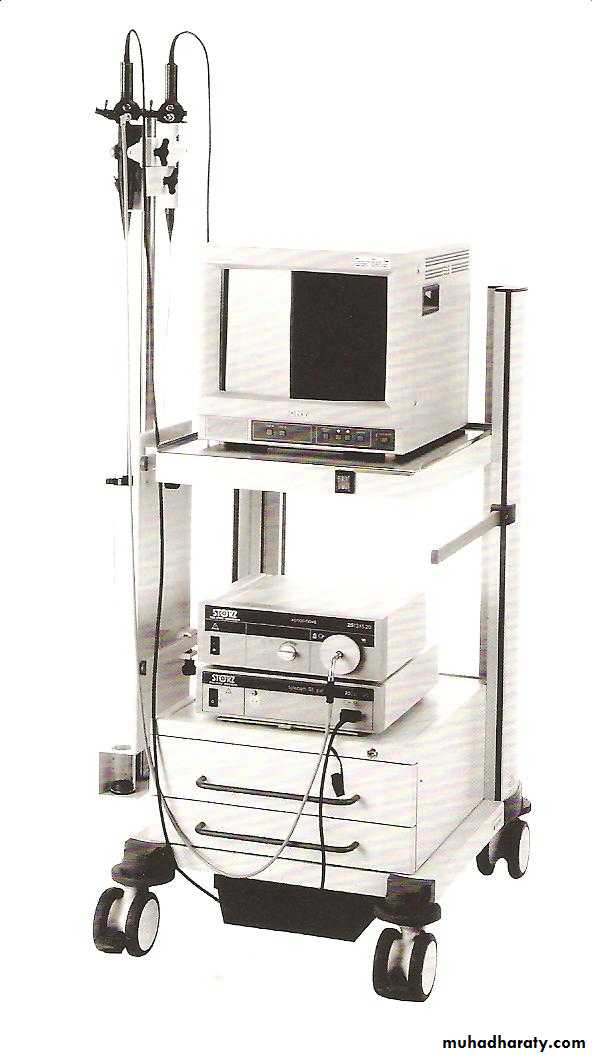
At the end of the 1980s, Asahi Pentax replaced the fiberoptic bundle with a charge-coupled sensor at the tip of the scope. This videobronchoscope allowed the bronchoscopist to look at a monitor screen instead of through the eyepiece of the scope

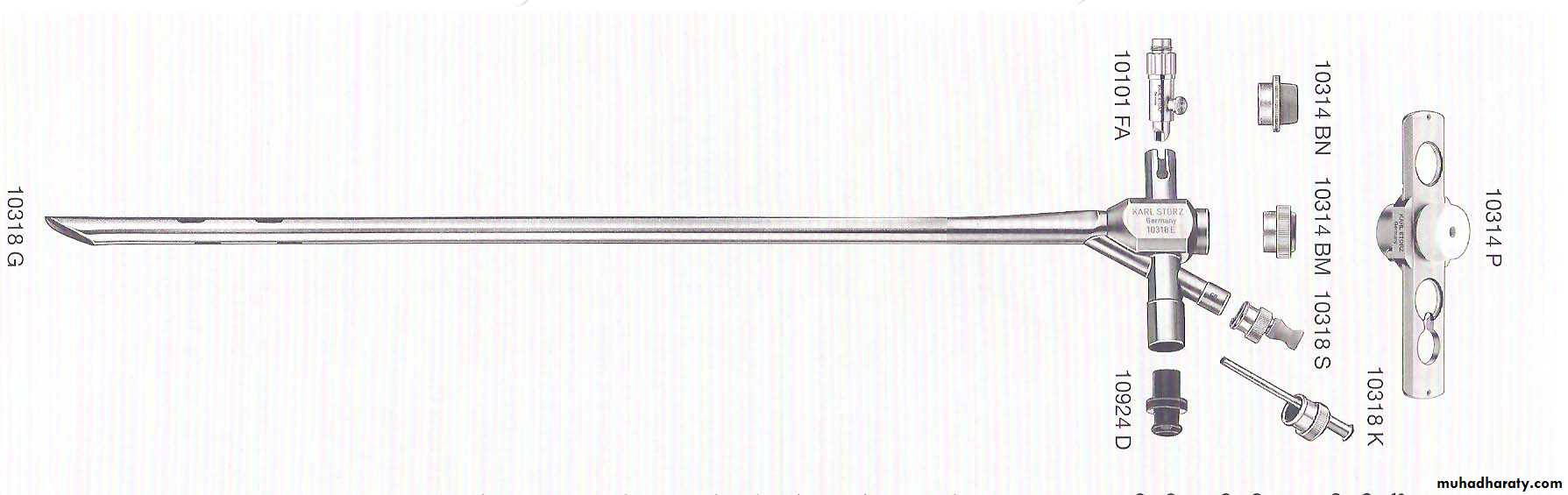
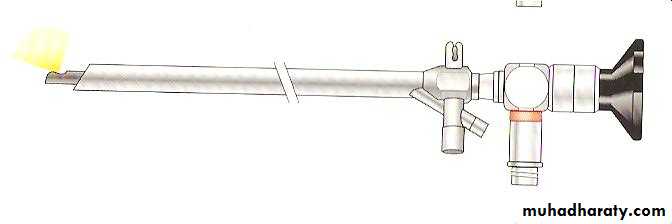
Rigid Bronchoscopes
• Hollow metal tubes , of variables sizes down to ( 3mm -9.5 mm) and variable length (20-40 cm) .These instruments usually have illumination at their tips as well as side holes near the tip to facilitate ventilation .They are always inserted trans orally .General anesthesia is recommended for its introduction .• i.e. Diagnostic and Therapeutic
• Indications for Rigid Bronchoscopy• 1-Hemoptysis
• 2-Tracheal stenosis.
• 3-Foreign body removal .
• 4-All bronchological interventions such as bougienage , removal of threads & post intervention hemoptysis.
• 5-Confirmation of cell type in case of previous , non diagnostic fiberoptic bronchoscopy .
• 6-Laser treatment
• 7-Removal of tumor
• 8-Removal of excess fibrin , mucous plug .
• 9-Bronchography .
• 10-Autofluorescence and photodynamic diagnosis .
• Endoscopey for the museum

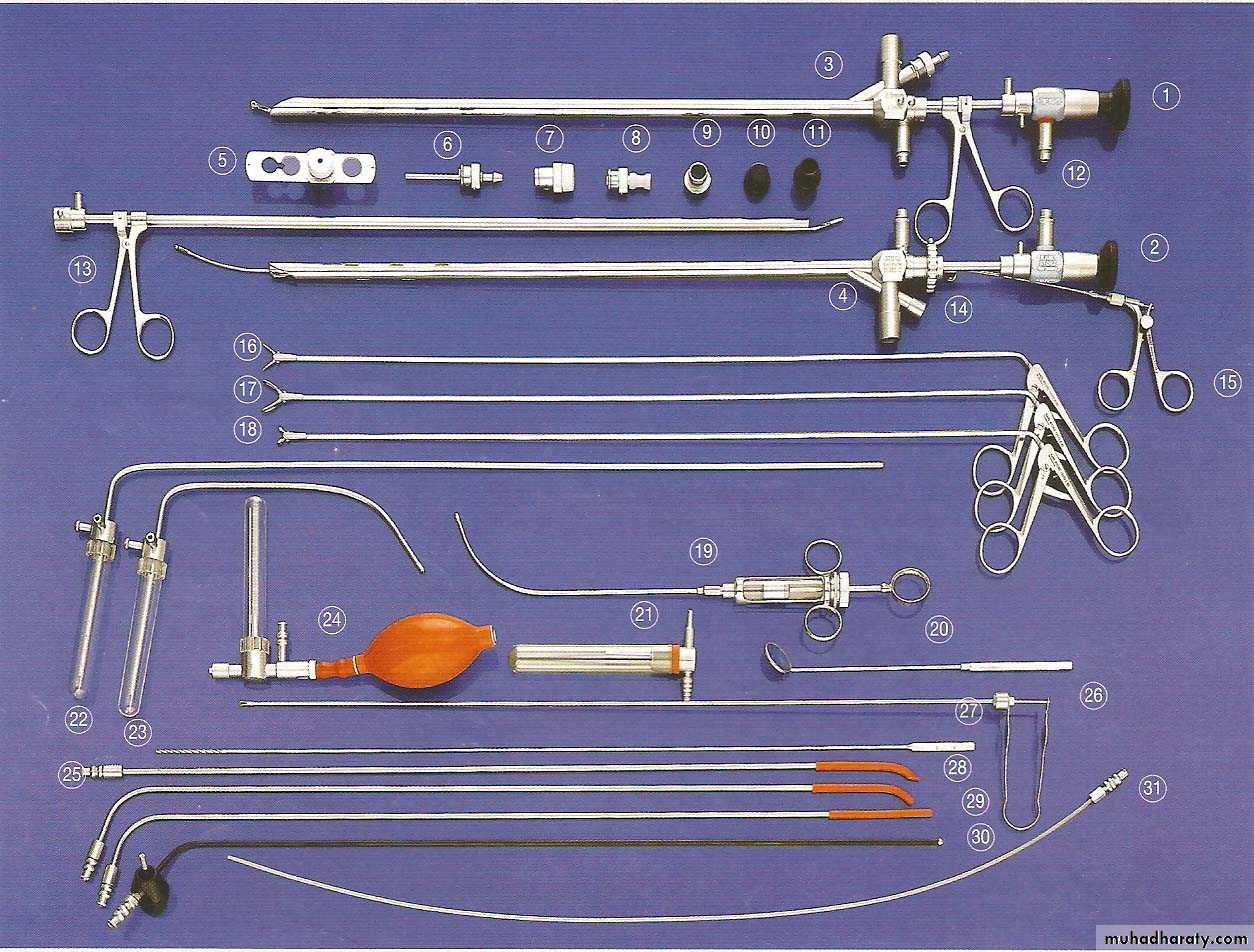
Bronchoscopy ( Adult Set )
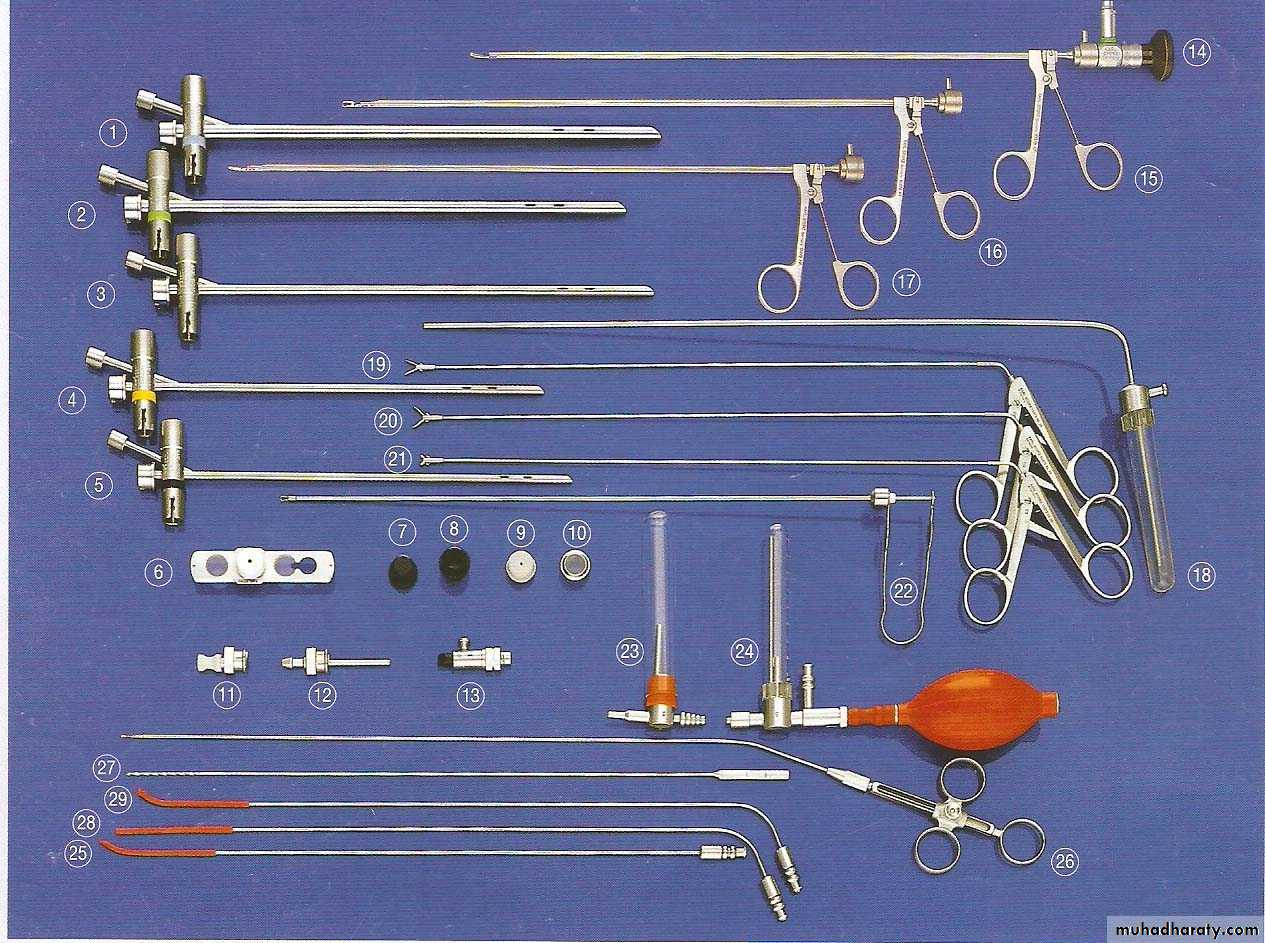
Bronchoscopy (Pediatric Set )•



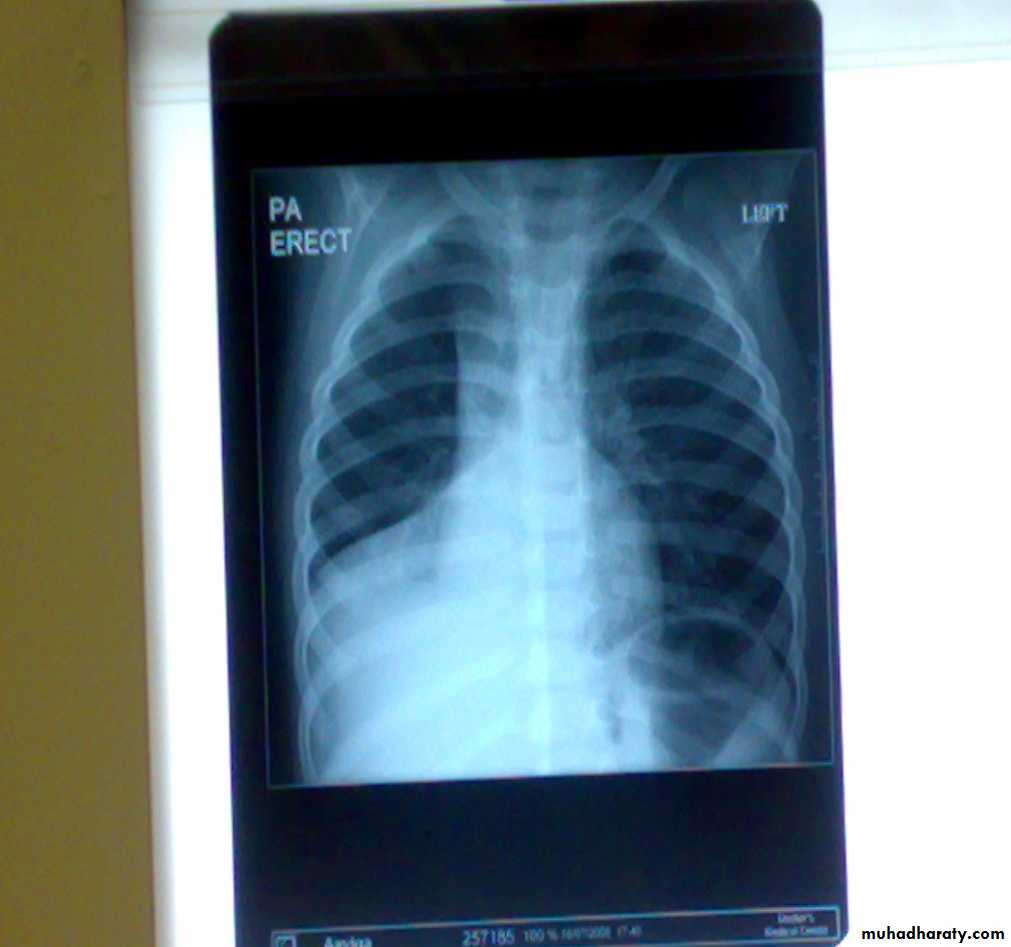


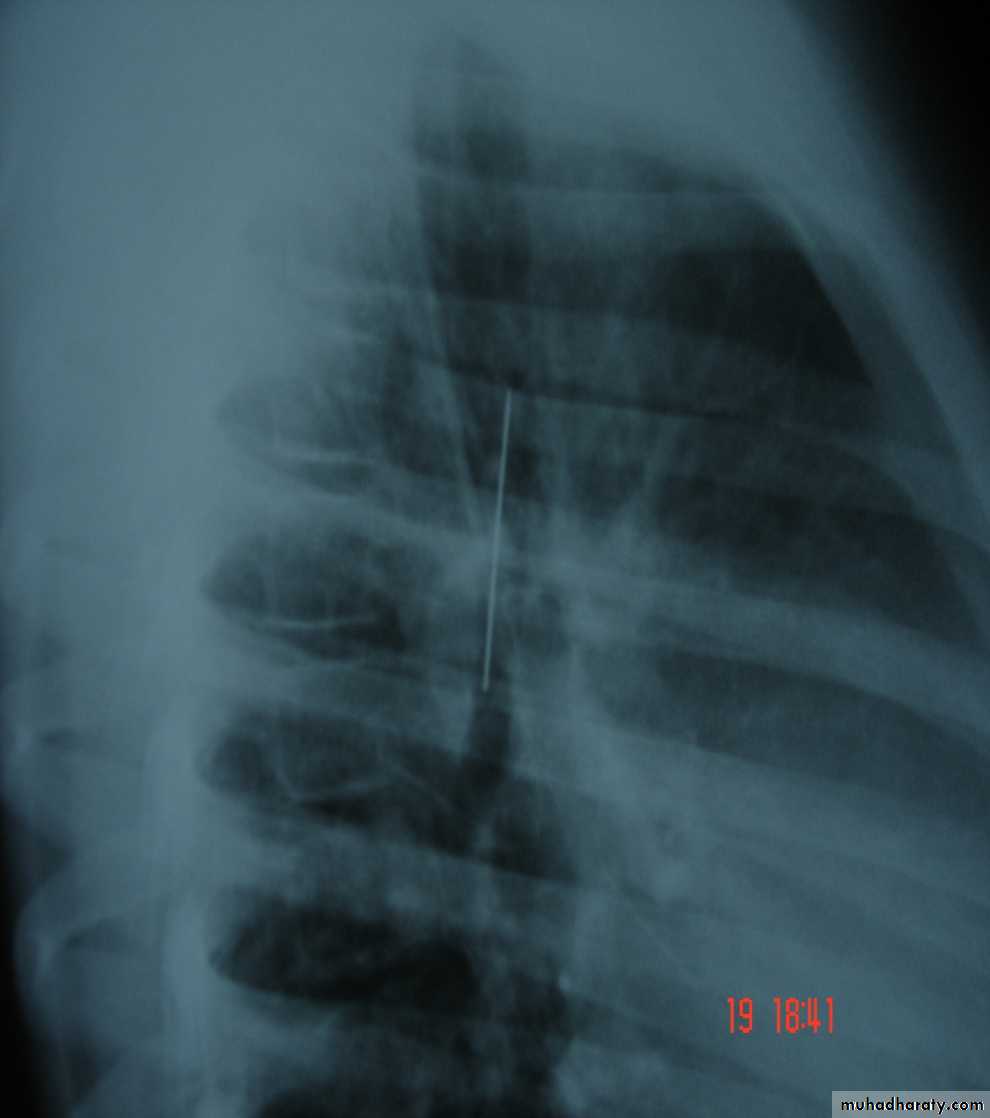
Foreign Body (RMB)
Flexible Bronchoscopy
It consists of Control section , a flexible insertion tube & a bending tip .The control section contains the eye piece ,control lever and a channel for aspiration or for introduction of solution and instruments.
• These flexible bronchoscopes have variable outside diameter (1.8 -6 mm) with inner channel ranging from (1.8 -2.6 mm) . Highly maneuverable and can reach areas in the endo bronchial tree not accessible to the rigid bronchoscopes .Can be inserted either transorally or transnasally or through the rigid bronchoscope.We have the Infantile , Pediatric , adult types and the Video –Bronchoscopes

• Major disadvantage of the flexible Bronchoscope is that it is a closed system that does not provide an airway , and the relatively small inner channel is considered to be incapable of allowing adequate suction when confronted with copious secretions or massive haemoptysis .
• It is not so much effective in the removal of foreign bodies .
Indications for flexible Bronchoscopy
1-For routine examinations .
2-Treatment of acute respiratory problems in the ICU.
3-Suction under visual control .
4-Use of catheter and brushes for cytology.
5-For obtaining secretions for bacteriological tests.
6-Localization of the bleeding site in case of hemoptysis.
7-Theraputic suction & irrigation .
8-Transbronchial lung biopsy .
9-Selective bronchography .
10-Autofluorescence & photodynamic diagnosis .
•
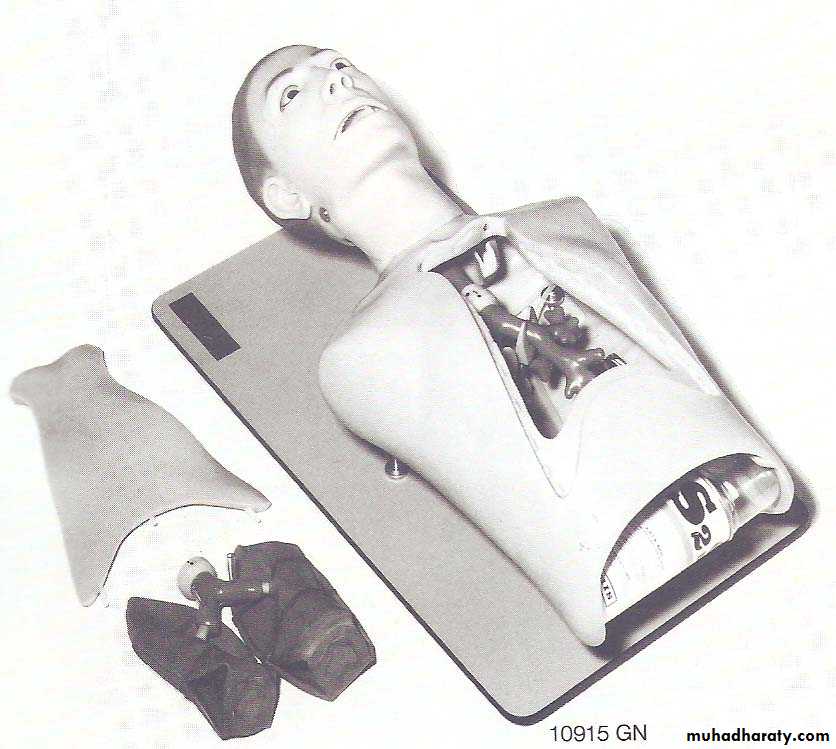
Tracheo-Bronchial Trainer

Sample collection (BAL)
Saline for irrigationLever
SuctionLecture scope
Rigid Bronchoscopy Is best avoided in the presence of Cervical spine injury thoracicto prevent hyperextension of the neck & in patient with Aneurysm of the aorta
• Flexible Bronchoscopy
• Best avoided in patient with Massive Haemoptysis & patients with air way problems
Contra indications
In cases of doubt as to whether bronchoscopy should be done or not , bronchoscopy should always be done ( Jackson’s 1915 statement ) .
In suspected cases of F.B inhalation it is better to have a negative bronchoscopy rather than to miss a F.B inside with all its pathological consequences .
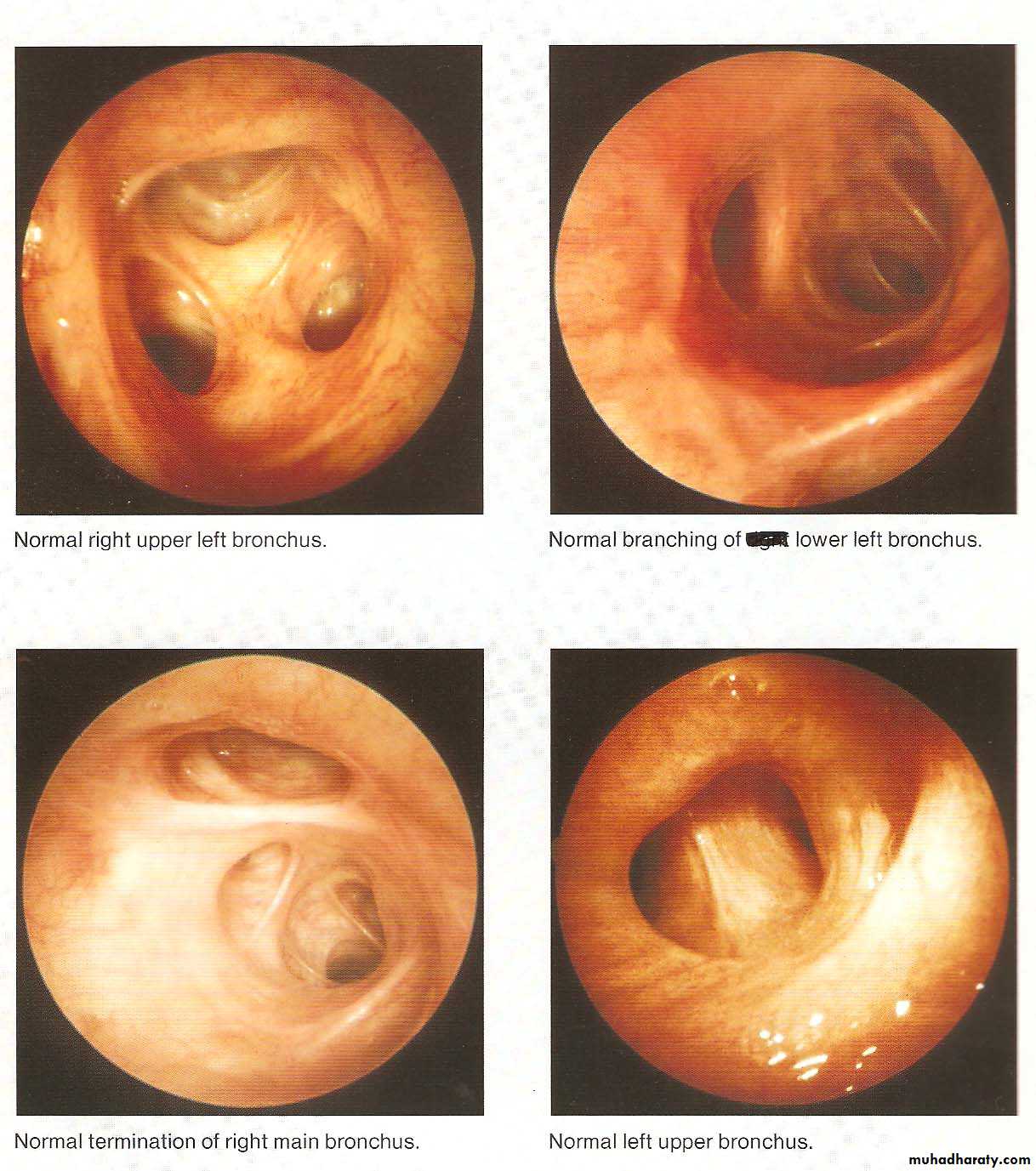
• Normal Bronchoscopic Findings
• Abnormal Bronchoscopic Findings

• COMPLICATIONS
• When bronchoscopy performed by properly trained individuals• It is a safe procedure .However a variety of other problems have been reported including
• Pneumothorax , bronchospasm , Bronchial perforation (Surgical emphysema & tension pneumothorax ) ,
• Subglottic edema , Uncontrolled bleeding , Infections
• Arrhythmias rarely ( Cardiopulmonary arrest )
• Hypoventilation (Hypoxia& hypercapnia)
• Majority related to a biopsy procedure So explorative thoracotomy may be safer than (injudicious biopsy )
• Some minor complications
• Damage of teeth , Injuries to lips or mouth
• Post bronchoscopy care
• 1-Close monitoring for 2-4 hours after the procedure
• 2-Eating and drinking is not allowed until the effect of anesthesia have worn off .
• 3-Some may advise routine CXR after performing a biopsy to check for signs of pneumothorax .
• 3-Those patients develop complications may need to stay in the hospital for additional time .
• 4-The patients may have sore throat , hoarseness ,cough or muscle ache .
• Fever up to temperature 38 “ c is common after bronchoscopy but usually for only 24 hours .
• Advances in Bronchoscopy
• 1- Brochoscopic Ultra-sound• 2-Bronchoscopic stenting (Air way prosthesis )
• 3-PDD & AF Bronchoscopy .
• 4-Bronchoscopic Laser therapy .
• 5-Bronchoscopic Electro Cautery
• 6-Cryo therapy
• 7-Brachy therapy
• 8-Photo therapy
Bronchoscopy need cooperation and mutual understanding Between
1-A well trained endoscopist2-a qualified staff
3-Expert and well trained anesthetist
Bronchoscopy
is now an integral part of respiratory medicine.
Diagnostic indications include tissue diagnosis, detection and staging of lung malignancy, evaluation of diffuse lung diseases like sarcoidosis and idiopathic interstitial pneumonias, pulmonary inspection of burn patients, identification of organisms infecting the respiratory tract and lungs.
As a therapeutic modality, bronchoscopy is used to place stents to protect airways vulnerable to collapse or occlusion, to remove foreign bodies or masses, to treat early stage endobronchial malignancy.
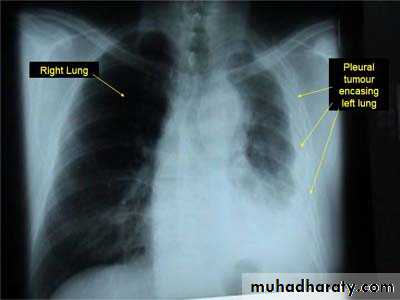
Pleural Tumors
Classified as primary and secondary tumors .Primary Pleural tumors are Mesotheiloma which may be
1-Localized benign 2- Diffuse Malignant
Malignant Mesothelioma causes chest pain , bloody pleural effusion and chest X-Ray findings of diffused pleural thickening with nodularity and limited pleural effusion .There is a possible relationship with asbestos exposure .
Metastases are uncommon .Death usually occurs within 1-2 years .It has a poor response to surgery , radiotherapy and chemotherapy .
Pleural involvement by metastatic diseases is more common than primary tumor and usually comes from lung , breast and stomach .
Benign Tumors of Trachea and Bronchi
Are rare ,more in males .They are slowly growing .Their presentation is is as a result of luminal obstruction or mucosal irritation .Patients may present with dyspnea , cough and haemoptysis .A sub glottic tumor presents with stridor ,The diagnosis is by bronchoscopy and treatment is surgical excision .E.g Papilloma , Haemangioma ,Chondroma and Fibroma
Bronchial Adenomas
1-Bronchial Carcinod
2-Muco epidermoid Tumors
3-Adenoid Cystic Carcinomas (Cylindromas )
4-Mucous Gland Adenomas
The first three are potentially malignant ,the 4th. Is benign
The first three are slowly growing , invade locally and surgical excision is the treatment of choice .
Bronchial Carcinoid Tumors
Resemble intestinal carcinoid as the cytoplasm as the cytoplasm of their cells contains neurosecretory granules .In the bronchus these tumors arise from the neuro endocrine argentafin cells of bronchial mucosa (Kultchitsky ‘s cells ) .They are grouped among APUD tumors (Amine Percursor Uptake Decaboxylation) .
They are capable of producing a number of hormones like Serotonin , histamine and gastrin .They are slowly growing tumors , but sometime they are aggresaive termed (atypical carcinoid ) .They present with cough , haemoptysis and dyspnea ) .
Carcinoid Syndrome is a rare ,presents with episodes of flushing , diarrhea and in addition to the systemic manifestations ,there may be cardiac manifestations .Elavated 5-HIAA may be detected in the urine ,which may be diagnostic .Bronchoscopic appearance is diagnostic and severe bleeding may follow a biopsy .Surgical excision is the treatment of choice .
• Carcinoma of the lung
• Affects both sexes , It is however commoner in men It has poor prognosis .
• The incidence has shown a marked rise during recent years partly because of improved methods of diagnosis and partly due to• 1-Ecessive cigarette smoking ,both active & passive smoking are implicated
• 2-Inhalation of irritants , such as silica ,cobalt dust .
• Pathology :-A-Central type is the commonest (75%).It arises in one of the main bronchi or their primary division leading to bronchial obstruction with secondary changes in the lung such as atelectasis .B-Peripheral type (25%) arises from the smaller bronchi and remains symptom less for long time .



Histologically Squamous cell Ca (SCC) 60% , smoker , centrally located ,metastasizes to mediastinal & supraclavicular LN . Adenocarcinoma (15% ) , located peripherally , more in women .Tends to metastasizes to the liver , brain ,bone & adrenals in addition to the LN Undifferentiated carcinoma (oat) cell carcinoma and large cell carcino(20-30%) which includes small ma Alveolar cell carcinoma , located peripherally ,metastasizes to the liver and adrenalsRecent classification..Non small & small cell carcinoma
• Superior sulcus tumor of Pancoast It is a low grade epidermoid carcinoma that grows slowly and metastasize late, infiltrates and involves lower root of Brachial plexus, intercostal nerves , Cervical sympathetic nerves & eroding the upper ribs ,producing pain in the shoulder & Horner's syndrome .
• Clinical features :-1- cough dry or productive2-Haemoptysis3-Chest pain4-Dyspnea5-Pleural effusion6-Anorexia & loss of weight7-Clubbing of the fingers8-Hoarseness of the voice (recurrent LN)9-Dysphagia involvement of the esophagus10-Hormonal syndromes ..ectopic ACTH , ADH, hypercalcaemia ,carcinoid syndrome
• Diagnosis
• Clinical , sputum cytology
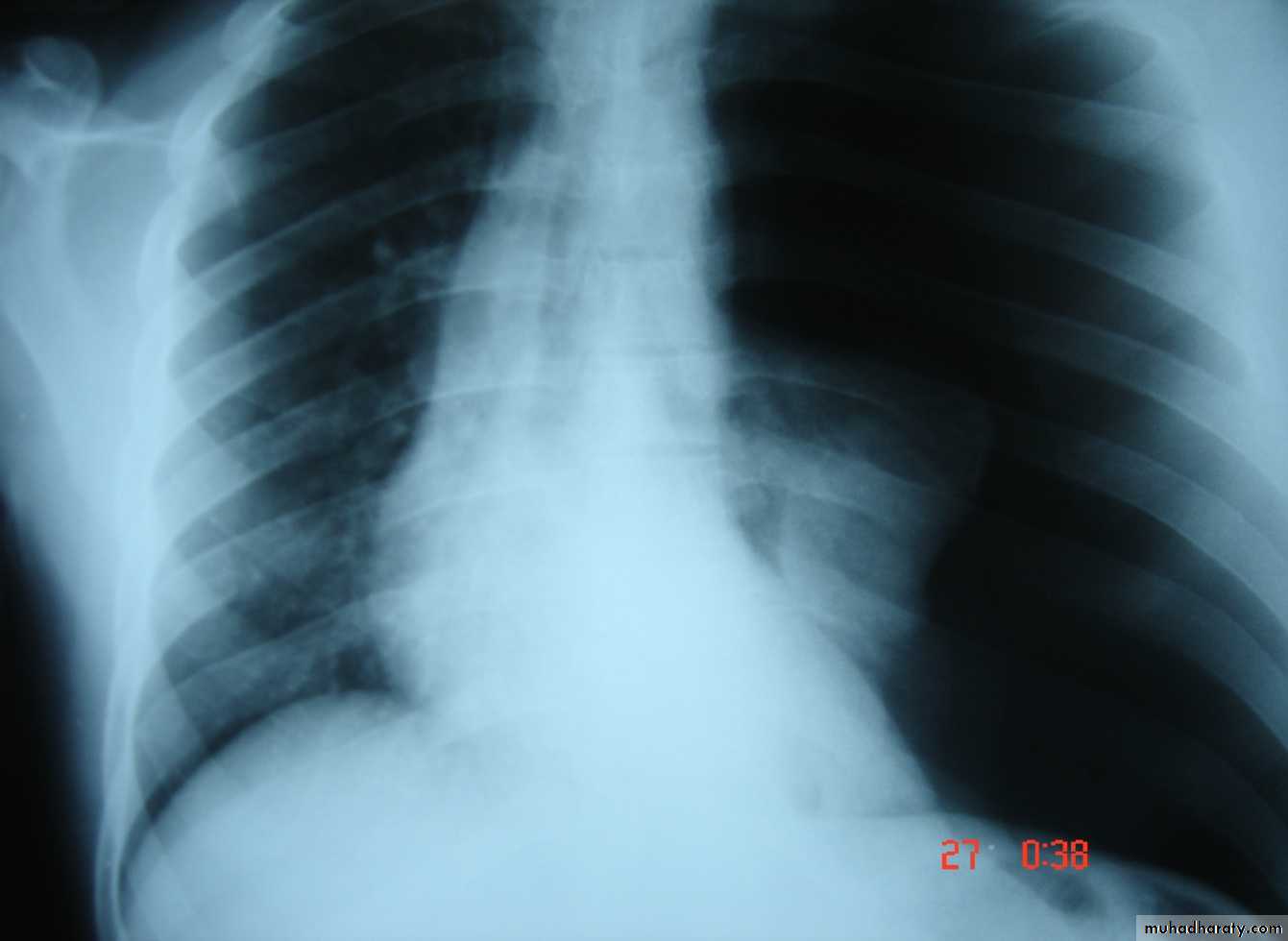
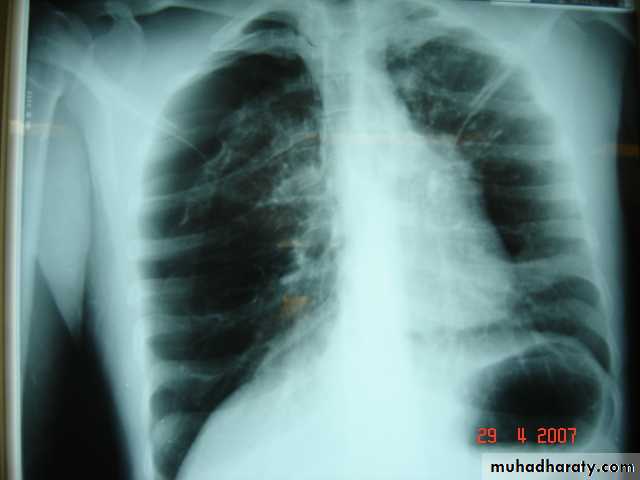
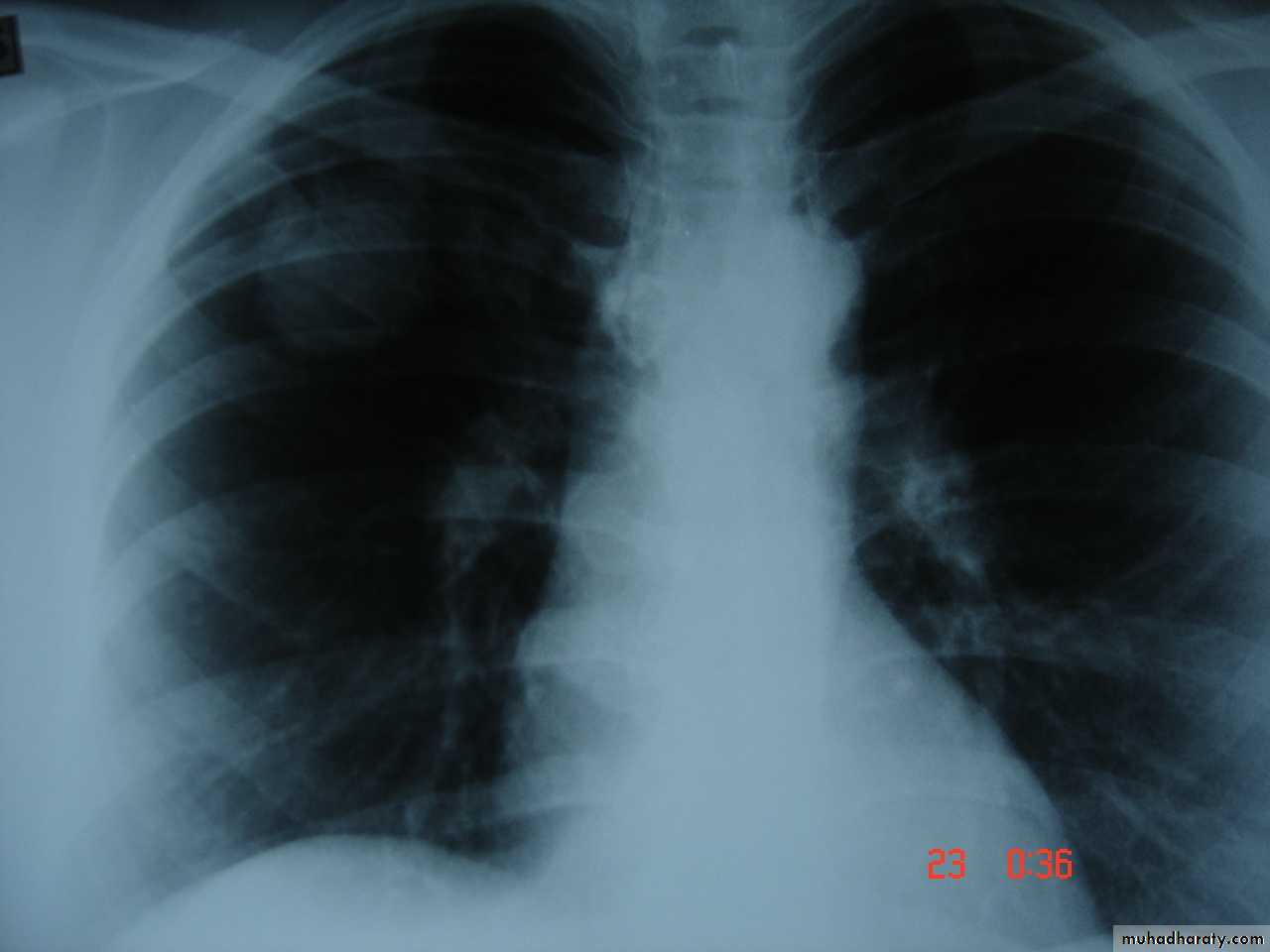
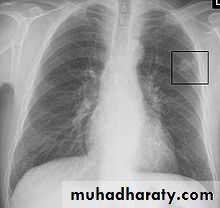
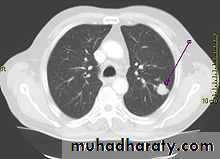
• Chest X-ray ,CT chest ..
• Bronchoscopy ,BAL ,bronchial brush &biopsy
• FNAC….or Trucut biopsy , pleural fluid aspiration & cytology
• Diagnostic Thoracoscopy & mediastinoscopy
• TNM classification for staging
• Signs of inoperability :-1-Bloody pleural effusion .positive for malignant cells2-Horner’s syndrome .3-Vocal cord paralysis4-Phrenic nerve palsy(elevated hemi diaphragm)5-SVC obstruction 6-Distant metastasis 7-If during surgery ,the tumor locally spreading or cannot be remover technically or fixed to the PA or to the heart ,it is technically irresectable


• Treatment 1-Surgery more than 50%of the patients have distant metastases at the time of diagnosis .50% Iresectable per operatively15-20 % resectability rate Surgery ..segmentecomy , lobectomy . pneumectomy
2-Radiotherapy
Pre operative or post operative
Chemo therapy vincristine or adriamycin
Bleomycin for malignant effusion
• Differential diagnosis of a solitary lung lesion (COIN LESION)
• 1-Hydatid cyst 4- Primary benign lesion• 2-Tuberculoma 5-primary malignancy of the lung
• 3-Angiomatous malformation (AV fistula) 6-metastatic tumors
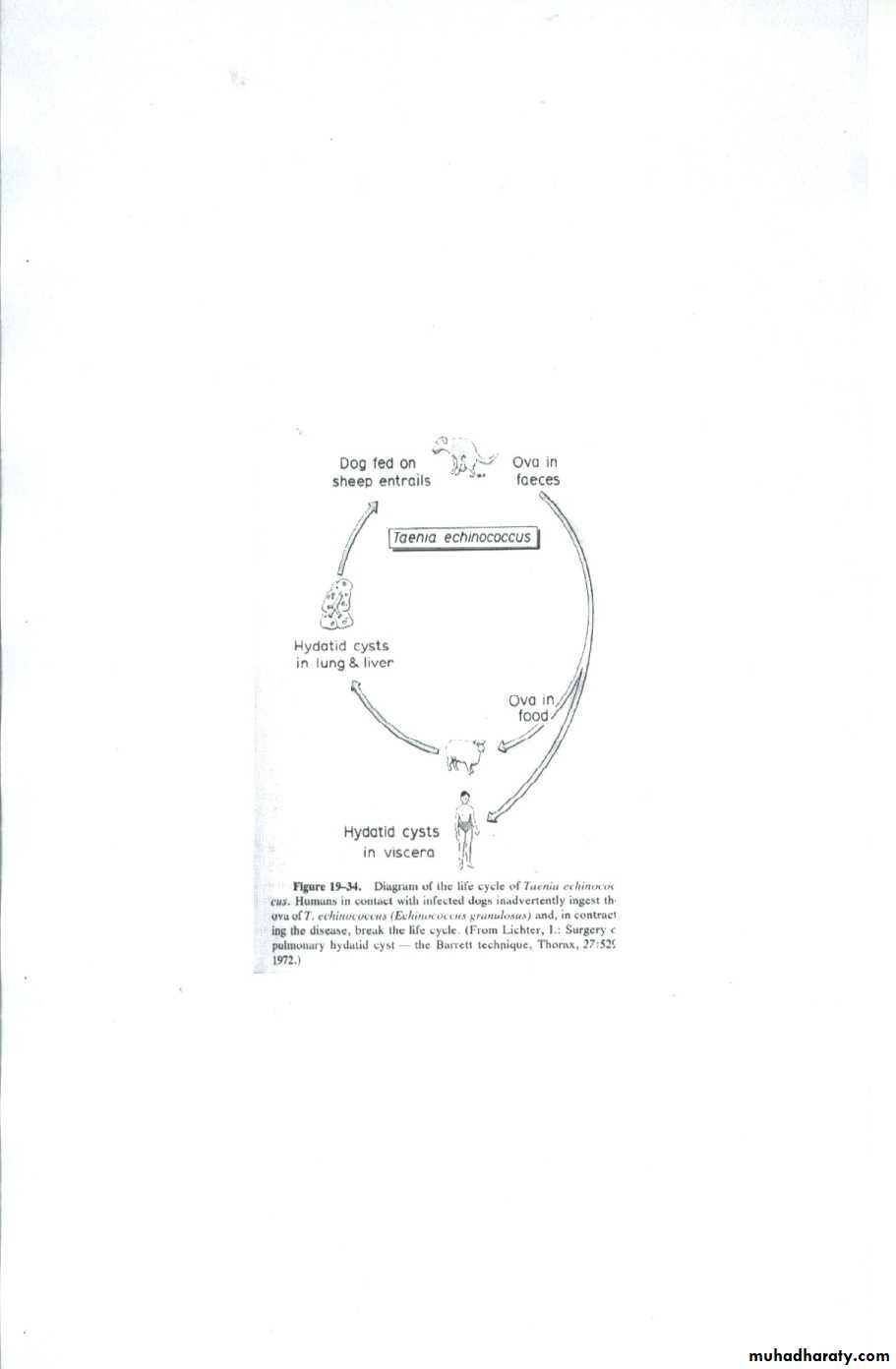
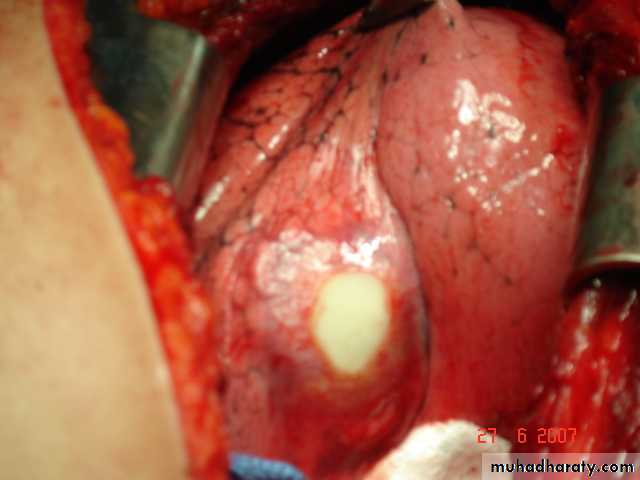
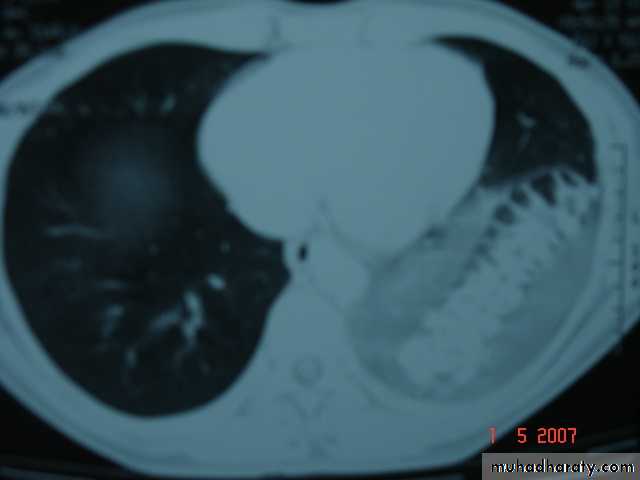
• Pulmonary Echinococcosis (Hydatid Cyst)
• Hydatid disease of the lung is caused by the small tape worm (Taenia Echinococcus ) or (Echinococcus Granulosis) .Hydatid cyst means cyst full of water .It has a life cycle between dogs & sheep .Parasites in the elementary tract of the dog shed ova that excreted in the dog faeces , contaminated the food of the sheep in which hydatid cyst will develops in the viscera . Including the lung .Infected sheep when slaughtered and its entrails are eaten by dogs , the life cycle is completed .When a human being hands or food become contaminated with canine fecal material containing ova which will be ingested .The parasitic larva burrow through the gastric mucosa and are carried to the liver in the portal venous circulation where most of them filtered out to form hydatid cyst of the liver , some escape the liver & lodge in the lung to form one or more hydatid cyst which grows slowly or rapidly over years .
• The cyst consists of a germinal layer & cyst fluid containing broad capsule & scoleses . A cellular white hyaline layers are laid down outside the cyst so that the cyst is enclosed by a laminated cyst membrane .As the cyst enlarged , it usually reaches the pleural surface . Compression of the lung tissues produces a thin fibrous layer of atelectatic lung tissue around the cyst (capsule , pericyst or adventia)

• Clinical Manifestation
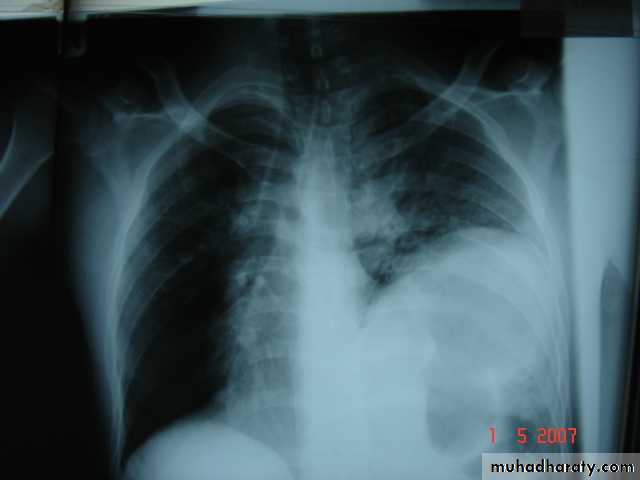
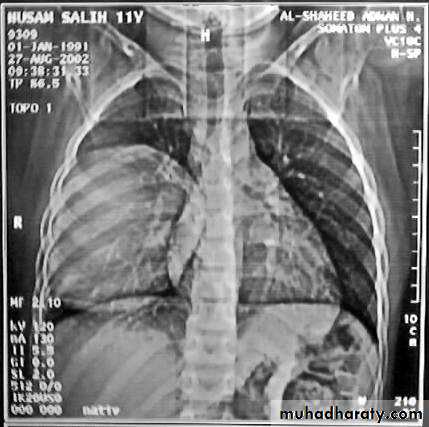
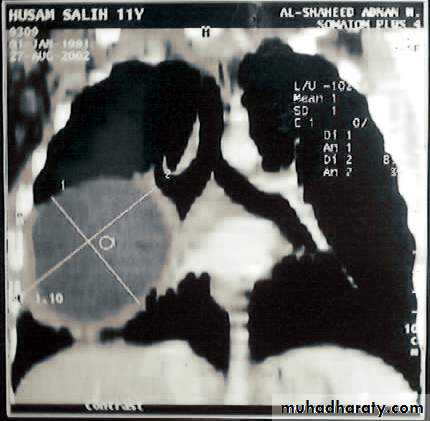
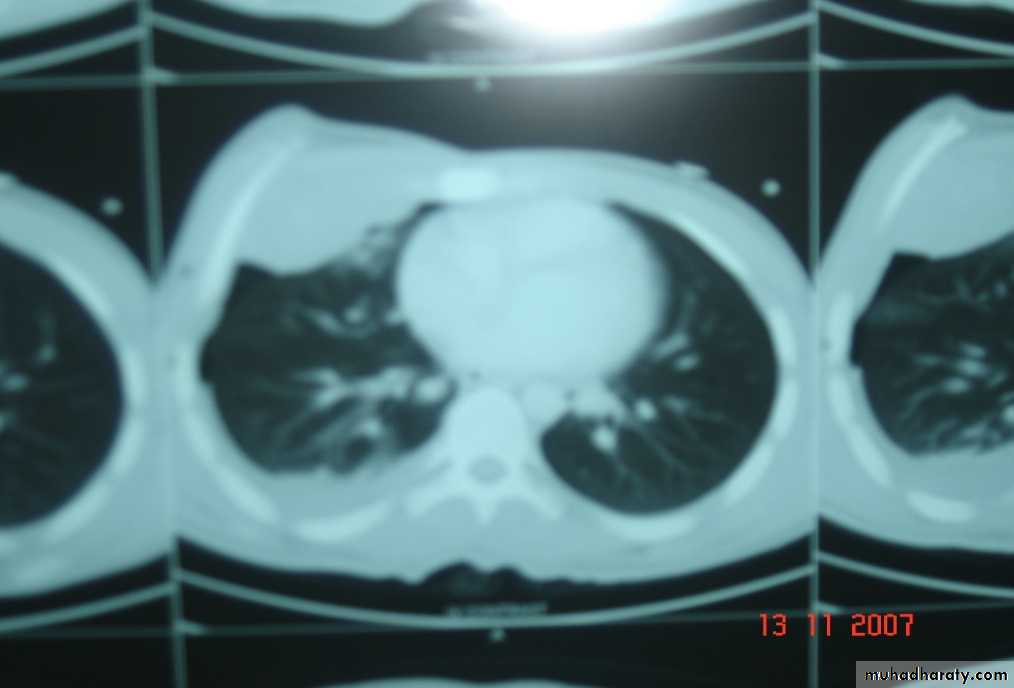
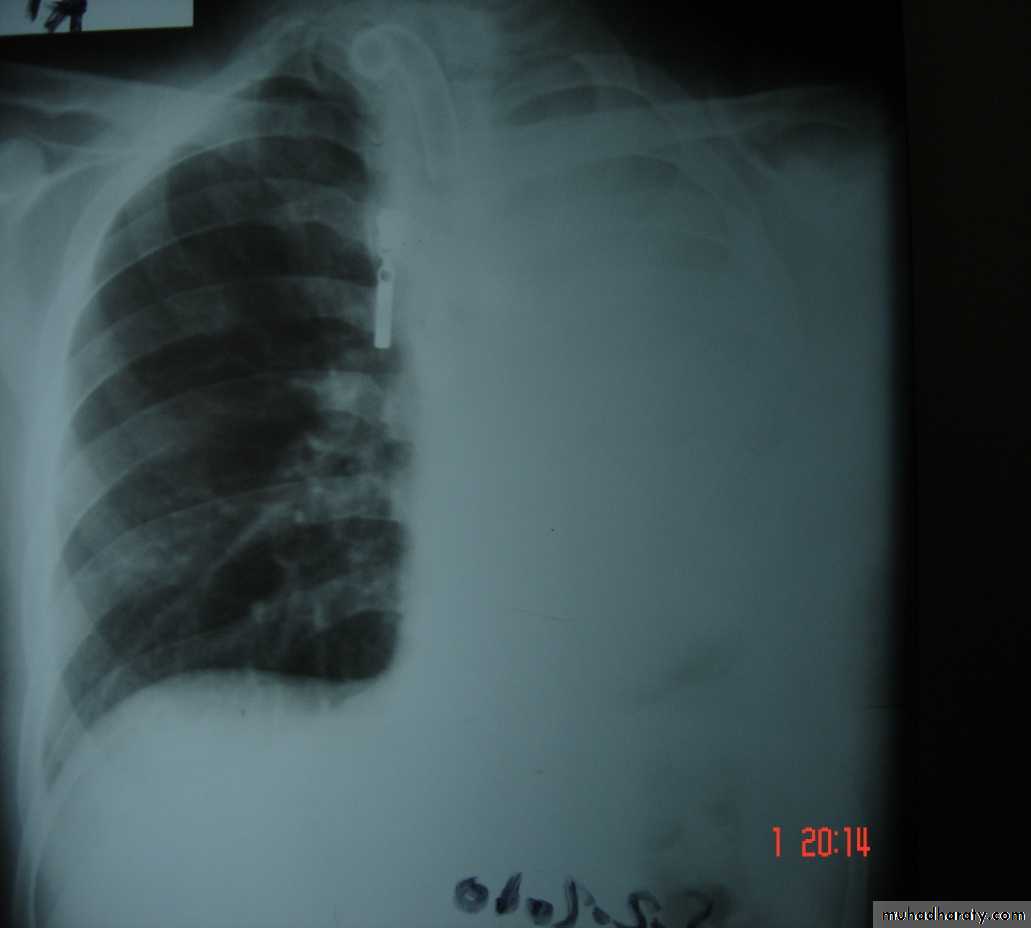
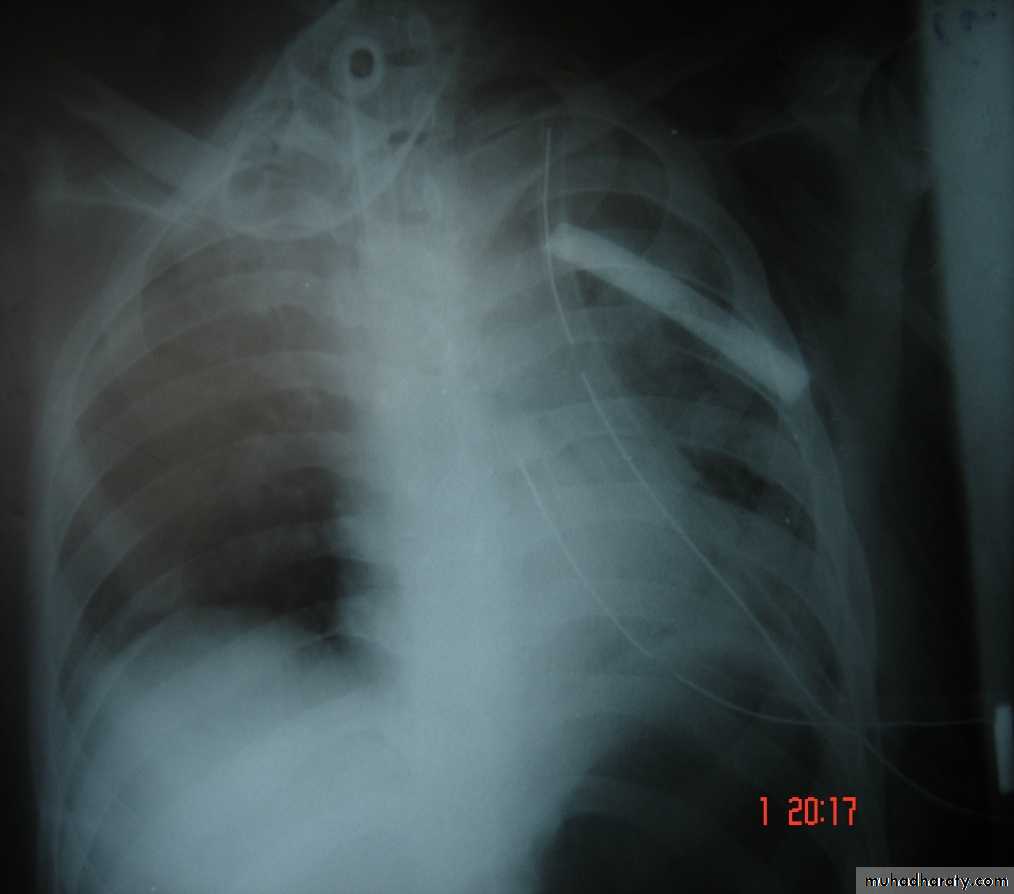
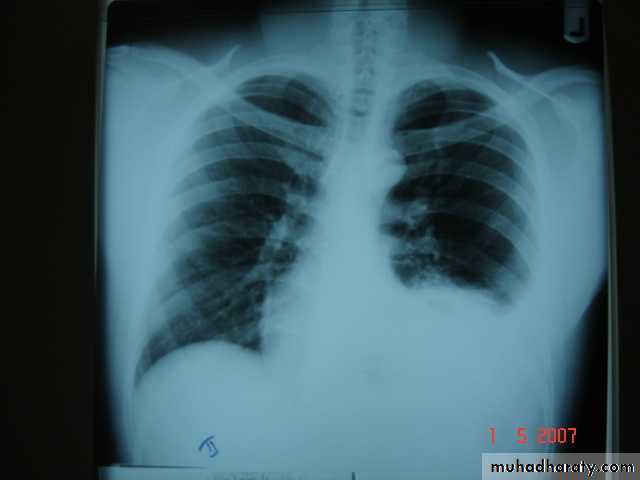
• A-Asymptomatic• Any smooth homogenous opacity of uniform density with clear cut border and little or no reaction around it on a chest X-Ray is a hydatid cyst unless proved the other wise .
• B-Cough & haemoptysis due to rupture of the cyst , or it can lead to severe dyspnea , or asphyxia ,or a hyper sensitivity reaction ,
• If the cyst get infected ,it will lead to formation of lung abscess or bronchiectatic changes .

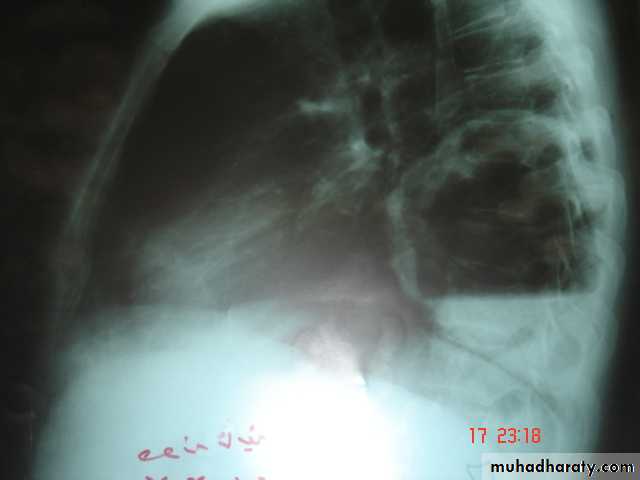
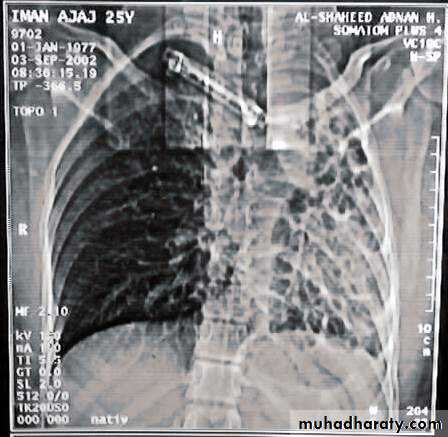
• Radiological Findings
• 1-Smooth homogenous opacity (Intact H.C).• 2-Partial rupture (per vesicular pneumocyst).
• 3-Complete rupture (Water –lilly sign) .
• 4-Formation of lung abscess(Air –fluid level) .
• 5-Completely coughed out cyst(empty cavity )
• 6-Rupture into the pleura (hydropneumothorax)


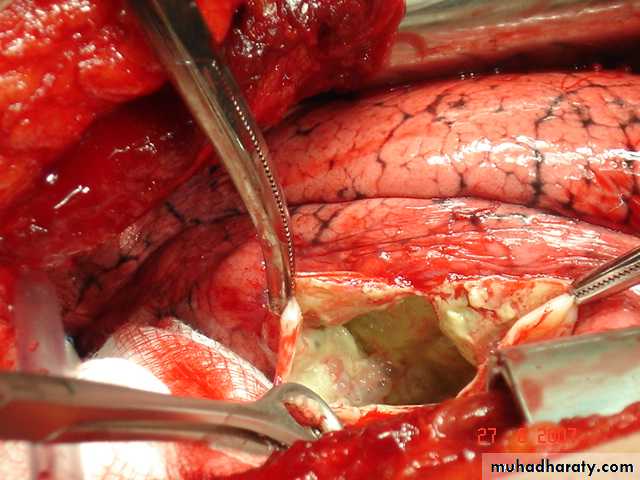
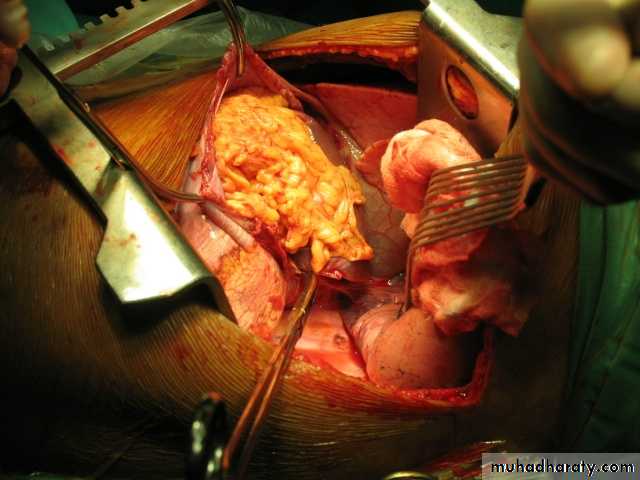
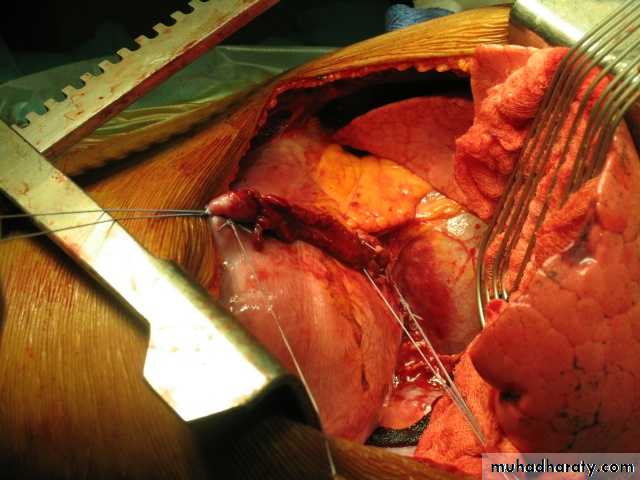
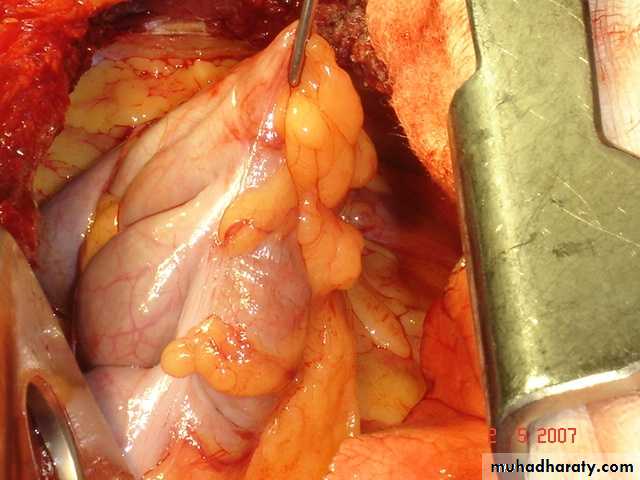
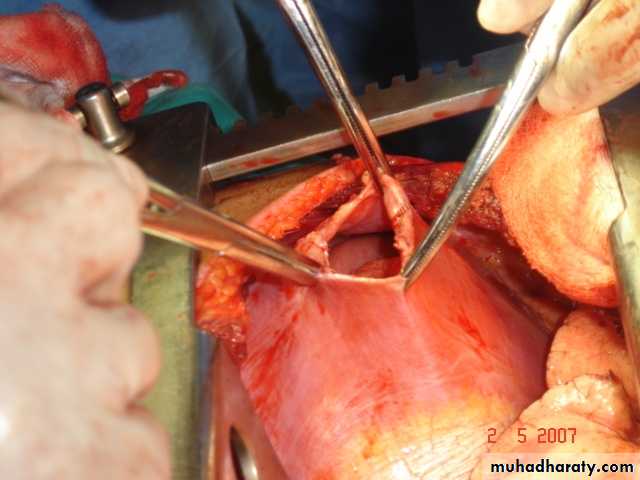
• Treatment
• Surgical• A-Inoculation means to remove it intact.
• B-Aspiration &evacuation technique
• C-Wedge resection or excision of the cyst with adjacent lung tissue.
• D-Segmentectomy ,Lobectomy or Pneumonectomy (rare ).
• Bronchiectasis
• Is a persistent abnormal dilatation of the bronchi generally beyond the sub segmental level , generally classified as three types cylindrical , varicose & saccular . The left lower lobe is more commonly involved then the right lower lobe .• Aetiology :-
• 1-Congenital causes (25%) 2-Acquired causes (75%)
• The acquired causes include air way infection (bact. Or viral)
• bronchial obstruction (F.B., neoplasm.,LN)
• It present in 40% of patients with chronic middle lobe infection (middle lobe syndrome) which involved impaired clearance of secretion mostly due to a pressure of enlarged LN.
• Congenital Bronchiectasis (Kartagner’s syndrome)
• It includes (Bronchiectasis , situs inversus ,sinusitis ,sperms hypo motility ) .It represents genetic disorder with abnormal ciliary motility so impaired clearance of sputum with the resultant bronchiectasis .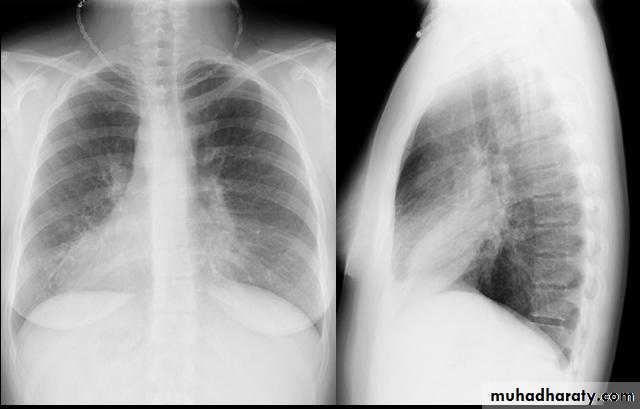
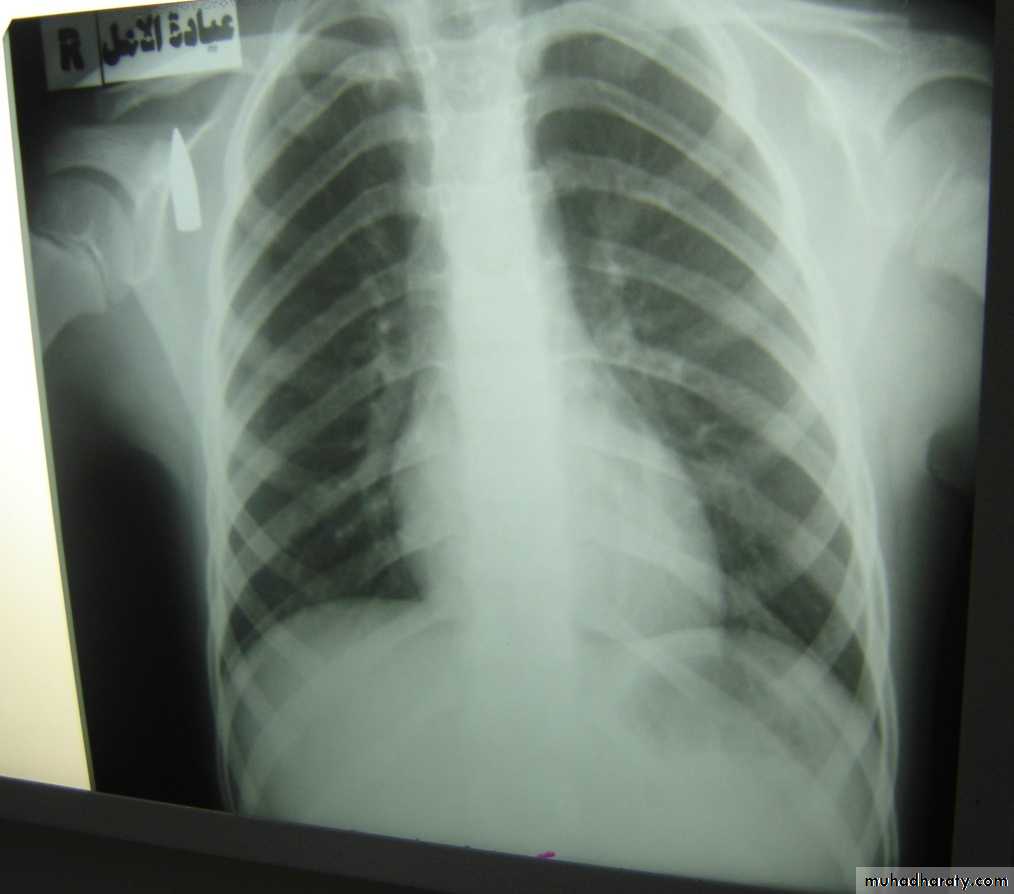
• Clinical manifestation :-The onset is mostly in childhood whereas symptoms generally appear in the second or third decade of life .The disease is more common in females .Major symptom cough with the production of purulent sputum with fetor oris .50% of the patients presented with haemoptysis .Others present with repeated RT infection .,others develop osteo arthropathy & finger clubbing which will resolve with treatment .
• Diagnosis :-
• 1-History chronic cough with purulent sputum.
• 2-Plain CXR may shows prominent vascular marking .
• 3-Bronchoscopy to diagnose obstructive lesion & to obtain bronchial wash for C&S test .
• 4-Bronchography through giving radio opaque dye through the bronchoscope & into bronchial tree ,now replaced completely by CT.
• 5-Chest CT is the single non invasive tool for both diagnosing &assessing the severity of the disease .
• 6-X-Ray paranasl sinuses to treat any excisting infection .
• 7-Pulmonary function tests very important specially in pre operative assessment .
• Treatment :-
• Medical treatment is the main stay of treatment ,it includes antibiotics , chest physiotherapy &postural drainage .
• Surgical treatment in cases of failure of medical treatment and it includes segmentectomy , lobectomy & pneumonectomy

• Lung Abscess It is a localized area of suppuration and cavitations in the lung.It includes TB , mycotic or parasitic cavitations ,bronchiectasis ,ruptured infected hydatid cyst , even pulmonary infarction with abscess formation & cavitating tumors
• Simple lung abscess (pyogenic) can occurs as a result of aspiration of a septic debris from the oropharynx into the lung or following dental or tonsillar operations .
• Esophageal diseases that lead to regurgitation &subsequent aspiration of esophageal content into the lung is another cause.
• Usually the aspiration is into the RMB leading to severe pnemonitis and liquefaction may occurs .As the liquefied necrotic material empties through the bronchus , a necrotic cavity containing pus and air is formed .The organism responsible may be streptococcus , staphylococus &eschrescia coli .
• Clinically cough & foul smelling sputum fever , pleuritic chest pain night sweat & weight loss in severe cases dyspnea & cyanosis
• Chest X-Ray
• Can shows the characteristic air fluid level ,may associated with pleural thickening , pneumothorax
• CT chest is helpful in demonstrating the abscess .
• Treatment
• 1- Primary treatment is Medical• Prolonged antibiotics treatment
• Bronchoscopy useful to remove a FB or drainage of abscess
• 2-Surgery indicated in
• Failure of medical treatment
• Massive haemoptysis
• persistent of a thick wall cavity
• when malignancy is suspected
• when empyaema develops
• Complications :-
• Empyaema , septicaemia ,metastatic brain abscess ,bronchogenic spread &development of chronicity
The Mediastinum
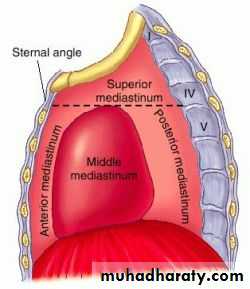
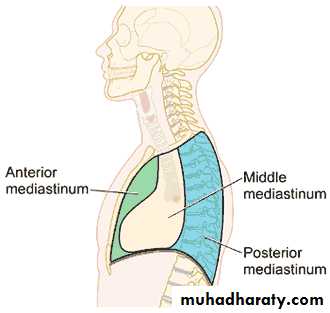
Mediastinum :-It is part of the chest , which is bounded above by the thoracic inlet , below by the diaphragm , anteriorly by the sternum , posteriorly by the dorsal vertebrae , and laterally by mediastinal pleura .It is divided by a transvere plane between the angle of Lewis anteriorly and the lower border of the 4th. Dorsal vertebra posteriorly into superior and inferior medistinum ,and the inferior medistinum is further subdivided by the presence of the pericardial sac into anterior , middle and posterior mediastinum
Mediastinal tumors or cysts occur in a chracterstic location so a mass in the superior medistinum is mostly thymoma or lymphoma ,while a neurogenic tumor occur mostly in the posterior mediastinum .Pericardial cyst or bronchogenic cysts occur in the middle mediastinum .
Mediastinitis
Causes :-1-Perforation of the esophagus or leakage from anastomosis .
2-Extension from a nearby infection (lung , vertebra ,pleura ).
3-Following median sternotomy for cardiac surgery .
Clinical manifestations :-
Fever , tachycardia , chest pain
Barium swallow is useful to demonstrate esophageal perforation.
Esophagoscopy will confirms the perforation .
Chest X-ray & CT –scan of great value in the diagnosis .
Treatment :-
1-Treatment of the cause .
2-Antibiotics according to culture and sensitivity .
3-Tube thoracostomy to drain any pleural collection .
4-Supportive therapy .
Surgical Treatment of Pulmonary Tuberculosis
Indications :-1-Massive or recurrent haemoptysis . Surgery is indicated to remove the source of bleeding .
2-Broncho pleural fistula
3-Open cavity with positive sputum resistant to 3-6 months of treatment .
4-TB bronchiectasis .
5-When malignancy is suspected as TB and malignancy can co exist .Carcinoma can arise in TB scar (Scar carcinoma ) .
5-Patients with (Trapped lung syndrome ) after chronic empyaema .
It includes segmetectomy ., lobectomy ., or pneumonectomy ., or to remove thickened adherent parietal and visceral pleura( decortication ) alone or in combination with pulmonary resection .

Superior Vena Cava Obstruction
A number of benign and malignant lesions involving the mediastinum may lead to obstruction of SVC with the production of the classical syndromeWhich characterizes by elevation of the venous pressure and edema of the face , neck and upper extremity with the appearance of the dilated venous chandelles in the chest wall and cyanosis .It may be caused by the carcinoma of the lung and in (25%) of the cases ,it may be caused by a benign lesion such as idiopathic mediastinal fibrosis .


Congenital Deformities of the Chest Wall
Pectus Excavatum in which the costal cartilages developed in a concave position and thus depress the sternum towards the vertebral column. Few patients may have cardio- respiratory problems . The best time of correction obtained at the age of 2-3 years .

Pectus carinatum ( Pigeon Breast )
Less common , consists of protrusion of the sternum ,caused by an upward curve in the lower costal cartilages , generally 4th. To 8th. Cartilages pushing the sternum forward .Surgery is the treatment of choice in symptomatic patients .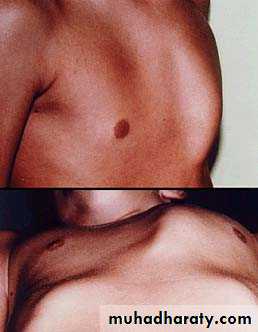
•
•
• Severe case of Pectus Carinatum


Thoracoscopy
It is the examination of the pleural cavity with an endoscope .Hans Jacobaeus was the originator of the thoracoscopy in 1910 .It is done under general anesthesia with double lumen intubation ,


Indications
1-Diagnostic1-Diagnosis of pleural diseases
2-Evaluation of carcinoma of the bronchus .
3- Biopsy of a discrete pulmonary nodules .
4-Evaluation of mediastinal mass .
Therapeutics :-
1-Treatment of pleural effusion .
2-Treatment of recurrent pneumothorax .
3-Removal of intra- pleural FB .
4-Debridement of empyaema space .
5-Dorsal sympathectomy .
There is no absolute contra indications for thoracoscopy .
• Mediastinoscopy
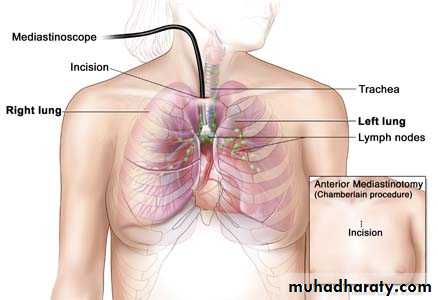
Is a surgical procedure that enables visualization of the contents of the mediastinum, usually for the purpose of obtaining a biopsy . Mediastinoscopy is often used for staging of lymph node of lung cancer or for diagnosing other conditions effecting structures in the mediastinum such as sarcoidosis or lymphoma .
It involves making an incision approximately 1 cm above the suprasternal notch of the sternum , or breast bone. Dissection is carried out down to the pretracheal space and down to the carina . A scope (mediastinoscope) is then advanced into the created tunnel which provides a view of the mediastinum. The scope may provide direct visualization or may be attached to a video monitor.
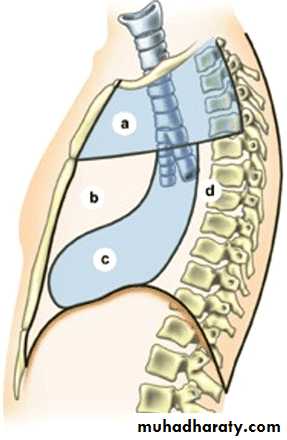
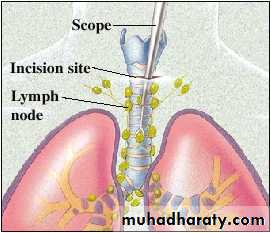
Mediastinoscopy provides access to mediastinal lymph node
Mediastinoscopy is used to explore the superior and middle part of the mediastinum. a. Superior mediastinum. b. Anterior mediastinum. c. Middle mediastinum. d. Posterior mediastinum
Mediastinoscopy is usually performed in a hospital under general anesthesia.. Once the patient is under general anesthesia, a small incision is made, usually just below the neck or at the notch at the top of the sternum. The surgeon may clear a path and feel the person's lymph nodes first to evaluate any abnormalities within the nodes. Next, the physician inserts the mediastinoscope through the incision. The scope is a narrow, hollow tube with an attached light that allows the surgeon to see inside the area. The surgeon can insert tools through the hollow tube to help perform biopsies. A tissue sample from the lymph nodes or a mass can be removed and sent for study under a microscope, or to a laboratory for further testing.
The person will remain in the surgerical recovery area until the effects of anesthesia have lessened and it is safe to leave the area. The entire procedure should require about an hour, not counting preparation and recovery time. Studies have shown that mediastinoscopy is a safe, thorough, and cost-effective diagnostic tool with less risk than some other procedures.
• Aftercare Following mediastinoscopy, patients will be carefully monitored and watched for changes in vital sign , or symptoms of complications from the procedure or anesthesia. The patient may have a sore throat from the endotracheal tube, experience temporary chest pain, and have soreness or tenderness at the incision site.
Risks
Complications from the actual mediastinoscopy procedure are relatively rare. The overall complication rates in various studies have been reported in the range of 1.3–3%. However, the following complications, in decreasing order of frequency, have been reported:hemorrhage
pneumothorax (air in the pleural space)
recurrent laryngeal nerve injury, causing hoarseness
infection
tumor implantation in the wound
phrenic nerve injury (injury to a thoracic nerve)
esophageal injury
chylothorax (chyle is milky lymphatic fluid in the pleural space)
air embolism (air bubble)
)
Causes :- 1-Blunt Trauma 2-Pentrating & perforating injuries 3-Blast injuries
1-Chest wall injury
Superficial chest wall injury affecting the skin and muscles of the chest wall without affecting the ribs or the underlying pleura as proved by normal chest x-ray .
Management is to arrest any bleeding and wound debridement with primary closure if possible .
Classification
• Chest Trauma




2-Ribs & Sternal injuries May lead to Single rib fracture the important thing is to relief pain by . analgesic , chest wall strapping or intercostal nerve block or Multiple ribs fractures , flail chest in that case four or more ribs are fractured anteriorly and posteriorly which lead to paradoxical respiratory movement with the resultant hypoxia and severe dyspnea that nictitates emergency intubation and assisted ventilation and if the patient needs prolonged intubation for more than one week then tracheostomy is indicated .

Flail chest
End tracheal tubeCosto chondral disruption
Chest wall haematoma
• 3-Pleurl injuries Can lead toA-Pneumothorax which can be partial or complete closed or open sucking or tension pnemothorax . B-Haemothorax may be mild or severe and may be with pneumothorax
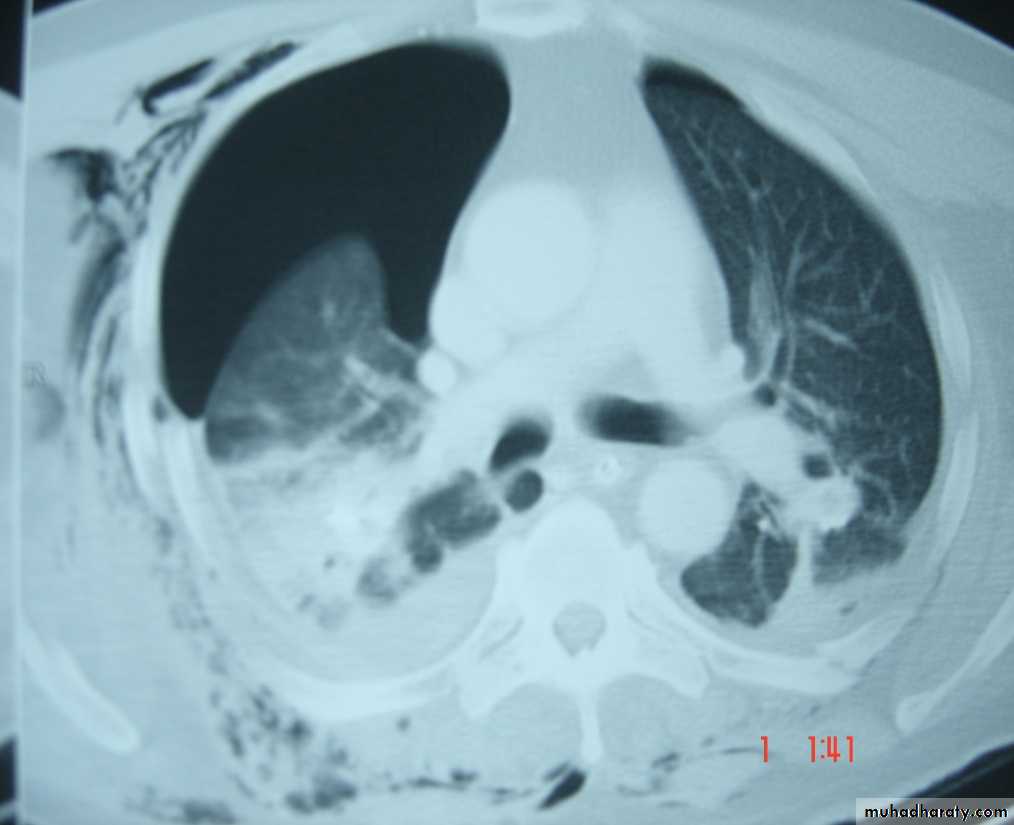
Pneumothorax
Collapsed lung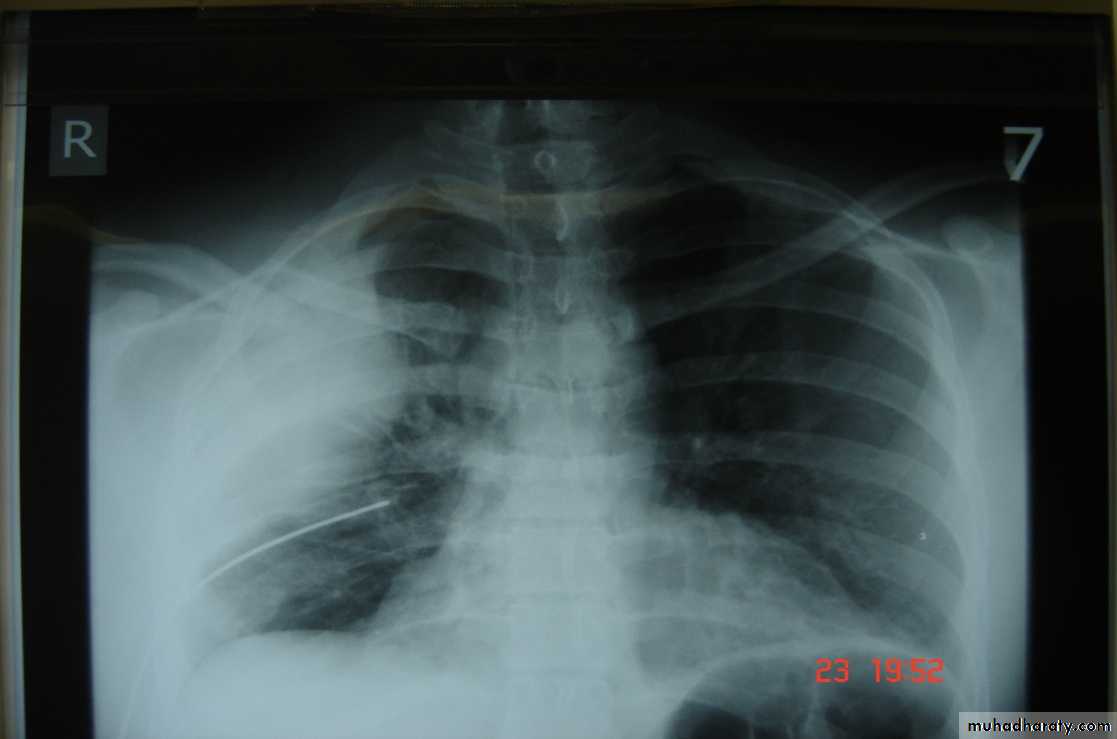
Traumatic haemothorax


Fractures
• 4-Pulmonary injuriesTrauma can lead to pulmonary contusion with interstitial edema which may lead to consolidation of the lung tissues and can be manage by antibiotics administration and clearing of secretion

• 5-Tracheo-bronchial injuries It may lead to crushing or complete tracheal separation which needs immediate air way management and repair of the trachea.Bronchial injuries can be so severe that it lead to complete separation of the bronchus which lead to pneumothorax with severe air leak, haemoptysis &haemothorax .Bronchoscopy will establish the diagnosis and surgery is mandatory to reanastomosed the bronchus .
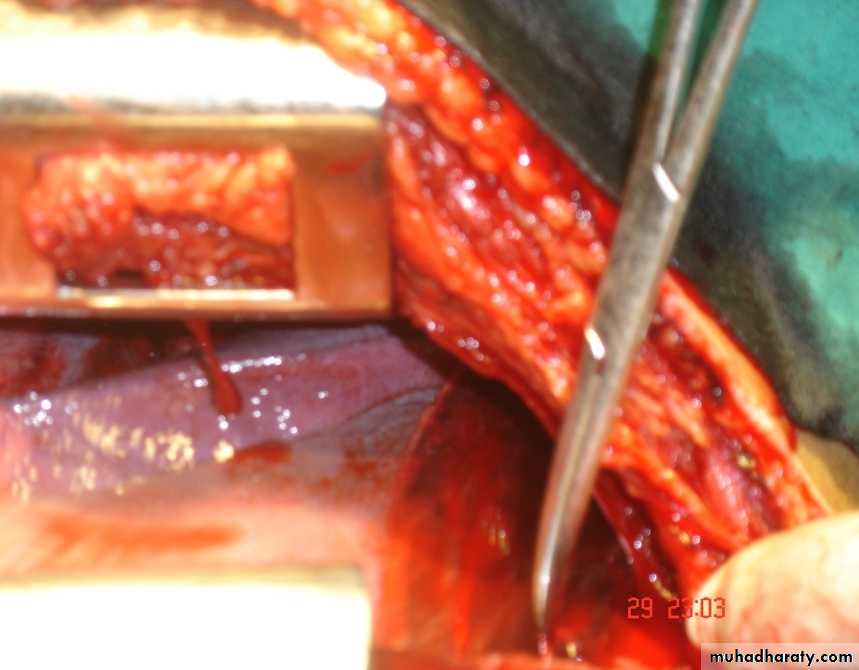
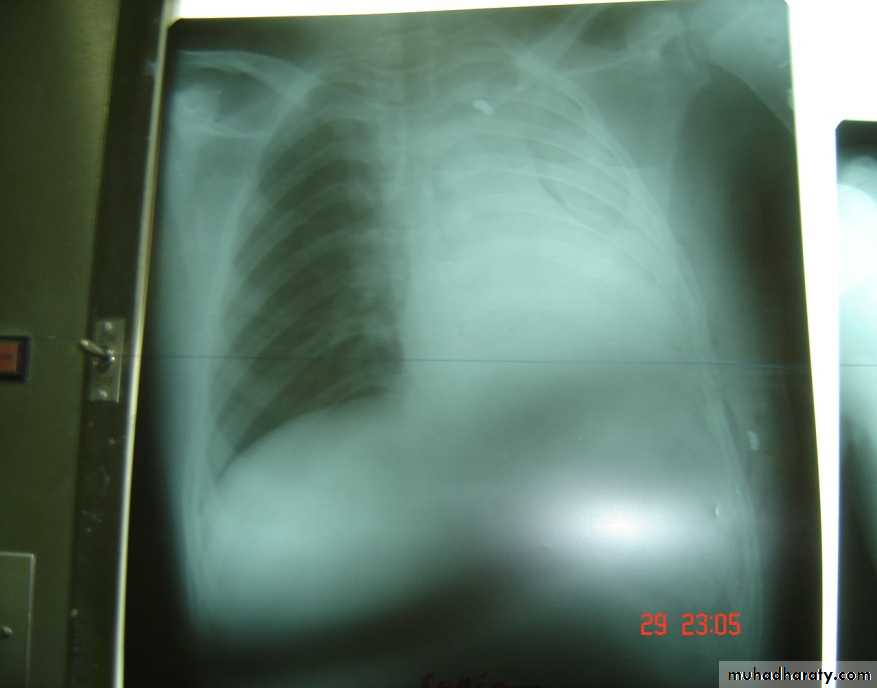
• 6-Great vessels injuriesInjuries to the thoracic aorta and its branches can occur mainly with deceleration injury . Most patients with ruptured aorta die immediately but in 10% of patients the per aortic tissues and pleura are able to maintain the intravascular pressure producing false aneurysms ,which can be diagnose by CT angiography and needs immediate surgery .

Traumatic aortic disruption is a time-sensitive injury requiring rapid and accurate diagnosis to prevent death.




Widen mediasinum
Descending aortic injuryEndo vascular stent control
• 7-Diaphragmatic injuries Trauma can lead to rupture of the diaphragm ,most commonly the left side affected ,leading to herniation of the viscera .Stomach is the most frequent organ to herniated followed by the transverse colon , spleen leading to collapse of the lung and mediastinal shift which can be seen on chest X-ray .Barium study is of great help in the diagnosis .Treatment surgery through abdominal , thoracic ,combined approach or by laparoscopy .




• 8-Esophageal injuriesThoracic esophagus rarely injured but mostly the cervical esophagus due to penetrating injury to the cervical region .Pain and dysphagia ,sometime fever .Diagnosis can be established by contrast study which will visualized the site of perforation.Treatment may be conservative by intravenous fluid , heavy antibiotics & NBM for 5-7 days which may be enough to seal the perforation , otherwise surgery is indicated to close the perforation .


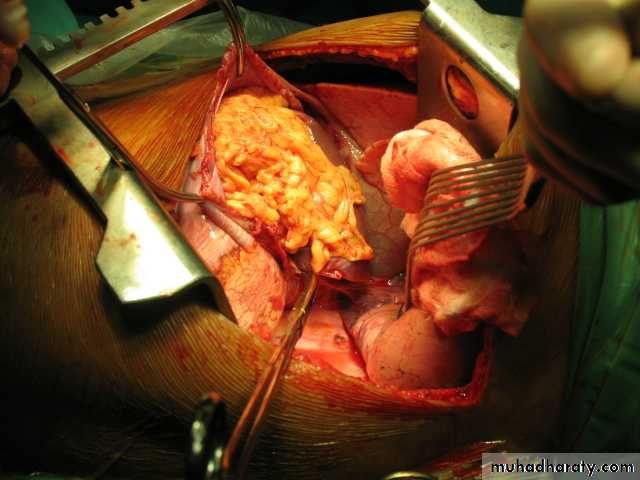
• 9-Cardic injuries May vary from superficial laceration to transmural damage which lead to atrial or ventricular septal defect or coronary artery injury .The patient may present with dyspnea ,hypotension & tachycardia .Diagnosis can be accomplished by Echocardiography .Management includes resuscitation & immediate thoracotomy or sternotomy to treat the injury .

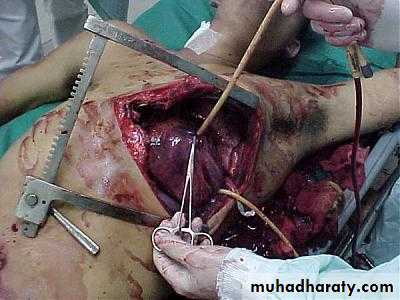

Stab to the pericardium - Resuscitative thoracotomy
"The surgeon who should attempt to suture a wound of the heart would lose the respect of his surgical colleagues" - Theodore Bilroth, 1882• Thoracotomy in chest trauma90% of chest injuries can be treated by chest tube (tube thoracostomy or intercostal drain (ICD) ).Thoracotomy may be …immediate (resuscitative thoracotomy ) ……emergency .. … elective
• Emergency Department Thoracotomy
• Resuscitative thoracotomy

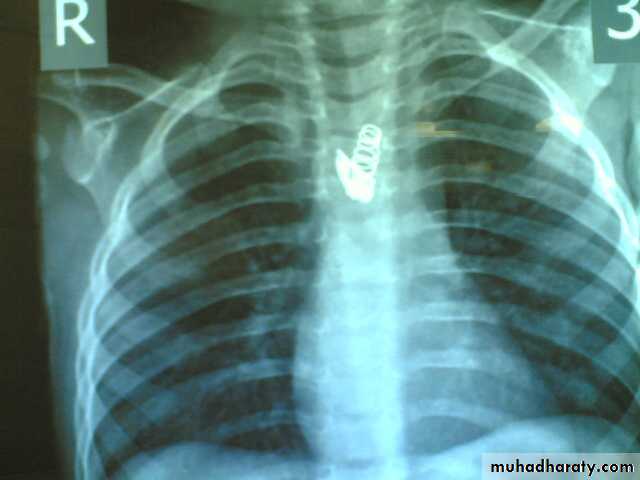
Penetrating thoracic injury
- Traumatic arrest with previously witnessed cardiac activity (pre-hospital or in-hospital) - Unresponsive hypotension (BP < 70mmHg)Blunt thoracic injury
- Unresponsive hypotension (BP < 70mmHg)
- Rapid exsanguinations from chest tube (>1500ml)
• Immediate(urgent) thoracotomy 1-Massive haemoptysis 2-Massive haemothorax/ initial dain1500 ml. or more than 200 ml /hr. for few hrs. 3-Ruptured bronchus with massive air leak 4-when great vessels injury is suspected 5- In diaphragmatic injury 6-Some cases with esophageal injury .7-In cardiac injury 8-In some cases of flail chest .
• Elective thoracotomy
• 1-Clotted haemothorax
• 2-Trapped lung syndrome
• 3-Big foreign body
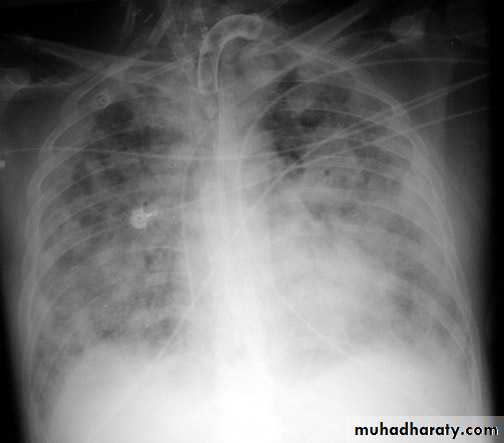
• Complications of chest injuries 1-ARDS: Syndrome of acute RF with the formation of a non –cardiogenic pulmonary edema leading to reduced lung compliance and hypoxaemia which is refractory to oxygen therapy characterized by bilateral diffuse pulmonary infiltrate on chest X-ray (white lung) .A less severe case (ALI=acute lung injury ) which consists of a non specific pathological changes in the lung in response to a specific insult . 2-Atelectasis3-Infection4-Pulmonary embolism5-Air embolism6-Traecheal complications7-Cardiac arrhythmias



• Poly trauma Team Members
Team leaderAnesthetist + assistant
General surgeon
Orthopedic surgeons
A/E physician
Two (2) nurses
Radiographer
Scribe (nurse or doctor)