Medical Education & Research challenges
PhD MD FRCP DCN , DTM&HProfessor of Inf. Diseases & Clinical Immunology
Baghdad, Iraq
Overview of infectious Diseases
Al- Abbasi A. M
INTRODUCTION TO INFECTIOUS DISEASES
Third Year CurriculumAL- Abbasi A.M.




Some demographic facts on Iraq
Population growth rate = 3%More than 24% living in the capital Baghdad
• Iraqi Land area is 435,000 Km 2
• Population = 32.1 million ,75% urban
• Total fertility rate = 4.9Pop. Below 15 years = 46.3%, 65 years & over =3%
Family Size 7.8
Mean agemales 59.2 year
Females 62.3 year ╬ year 2001
National income / Capita
865 American dollars
Crude birth rate
Crude fatality rate
39.4/ 1000
10.6/ 1000 ╬ year 1997

Preventable infections diseases caused sharp increase in the fatality rates for all ages after substantial regression
before 1990.
Status of Infectious Diseases
for the year 2003-2004 - on




Salmonellosis, Shigellosis , Compylobacteriosis,helmenths Parasitic diseases, viral Diarrhea, food poisoning , chemical poisoning …etc.
• no
• CFR
• Disease
• 1,804,374 (rate of infection =5-8/child)
• 0.14
• ARI
• 750,000 Rate = 3-6/child
• 0.08
• Diarrheal Dis.
• More than 29,000 case
• Typhoid fever• 19.824
• Viral Hepatitis
• (enterically transmitted)
• 23.790
• Pulmonary TB
• 3.218
• Kala- Azar



Student
C.V ProgramTeaching
British style 1960
Medical Education


Perfect diagnosis . good training
Prudent use of drugsEnvironmental Contamination & Radiation
Chemical Contamination
Emerging & Reemerging diseases
Good Surveillance System
Hospital Contamination &
Nosocomial infectionsMultiple antimicrobial resistant microbes



Definitions
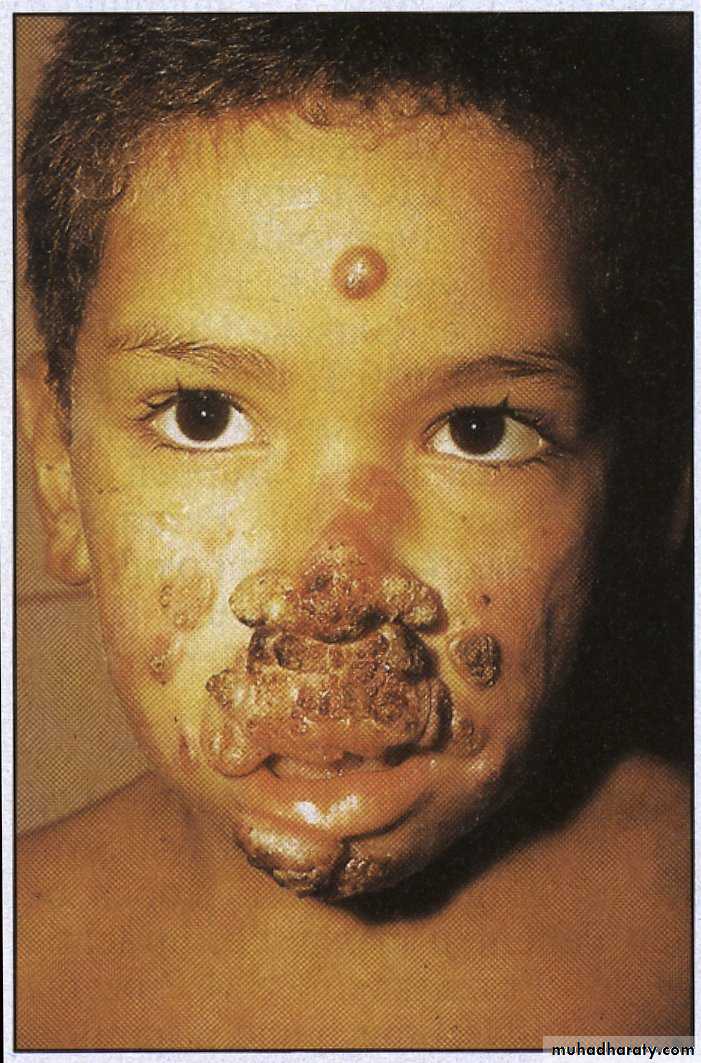
Infection - the pathological state resulting from the invasion of the body by pathogenic microorganisms.
Infection is the invasion of a host bodily tissues
by disease-causing organisms, their multiplication, and the reaction of host tissues to these organisms and the toxins they produce.Contagious disease

Infectious Agents &Some Definitions
PrionsViroids
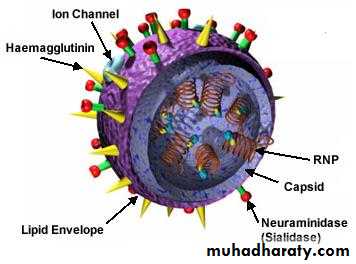
Viruses
Chlamydia
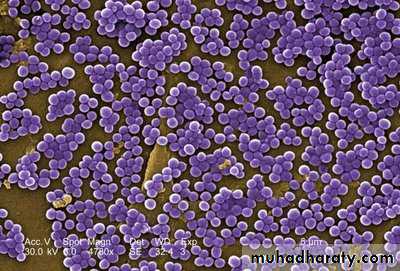
Bacteria
Fungi
Parasites
Helminthes
Co infection
Super infection
Autoinfection
Opportunistic infection
Virulence
Latent infection
Incubation period
Zoonosis


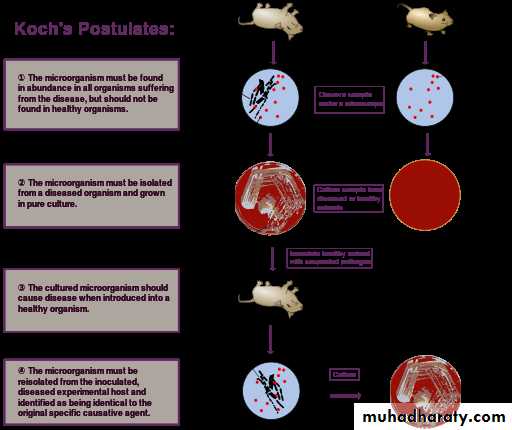
Koch's postulates
The microorganism must be found inabundance in all hosts suffering
from the disease, but should not be
found in healthy host.
The microorganism must be isolated
from a diseased host and grown in
pure culture.
The cultured microorganism should cause disease when introduced into a healthy host.
The microorganism must be re isolated from the inoculated, diseased experimental host and identified as being identical to the original specific causative agent.
However, Koch abandoned the universalist requirement of the first postulate altogether when he discovered asymptomatic carriers of cholera and, later, of typhoid fever.
Asymptomatic or subclinical infection carriers are now a common feature of many infectious diseases, especially viruses as polio, herpes simplex, HIV, and hepatitis C.
As a specific example, all doctors and virologists agree that poliovirus causes paralysis in just a few infected subjects, and the success of the polio vaccine in preventing disease supports the conviction, poliovirus is the causative agent.
The second postulate may also be suspended for certain microorganisms or entities that cannot (at the present time) be grown in pure culture, such as prions responsible for Creutzfeldt–Jakob disease.
Scenarios Requiring Empiric Implementation of Precautions Airborne Precautions
Vesicular rashMaculopapular rash with coryza and fever
Cough, fever, upper lobe pulmonary infiltrateCough, fever, any pulmonary infiltrate in an HIV-infected patient (or patient at risk for HIV infection)
Fever, respiratory symptoms in a person with recent contact with SARS patient or recent travel to area with SARS transmission*
Scenarios Requiring Empiric Implementation of PrecautionsDroplet Precautions
-Meningitis
-Petechial or ecchymotic rash with fever
-Paroxysmal or severe persistent cough during periods of pertussis activity


Scenarios Requiring Empiric Implementation of Precautions Contact Precautions
Acute diarrhea with likely infectious etiology in incontinent or diapered PatientDiarrhea in adult with recent antibiotic use
Vesicular rash*
Respiratory infections in infants and young Children
History of infection or colonization with MDR Organisms
Abscess or draining wound that cannot be Covered
Fever, respiratory symptoms in a person with recent contact with SARS patient or recent travel to area with SARS transmission*
Scenarios with Known or Suspected Diseases or Pathogens Airborne Precautions
Measles
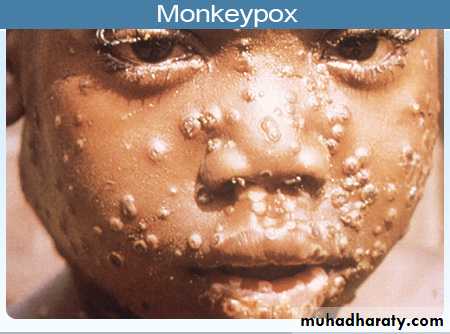
Monkey pox
Tuberculosis, pulmonary or
laryngeal
SARS
Smallpox
Varicella
Zoster (disseminated or immune
compromised patient)


Scenarios with Known or Suspected Diseases or Pathogens Droplet Precautions
Adenovirus (infants, children)*Diphtheria, pharyngeal
Haemophilus influenzae meningitis, epiglottitis
H. influenzae pneumonia (infants, children)
Influenza
Meningococcal infections


Scenarios with Known or Suspected Diseases or Pathogens Droplet Precautions
MumpsMycoplasma pneumonia
Parvovirus B19
Pertussis
Plague, pneumonic
Rubella
Streptococcal (group A) pharyngitis,
pneumonia, scarlet fever
(infants or young children)

Scenarios with Known or Suspected Diseases or Pathogens Contact Precautions
Abscess, not covered or drainagenot contained
Adenovirus (infants, children)*
Cellulitis (uncontrolled drainage)
Clostridium difficile diarrhea
Conjunctivitis, acute viral
Decubitus ulcer, infected and drainage not contained
Diphtheria, cutaneous



Scenarios with Known or Suspected Diseases or Pathogens Contact Precautions
Escherichia coli O157:H7 colitis (diapered orincontinent patient)
Enteroviral infections (infants, young children)
Furunculosis (infants, young children)
Hepatitis A (diapered or incontinent patient) AHSV (neonatal; disseminated; severe primary mucocutaneous)
Impetigo
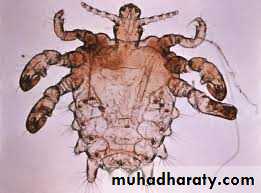
Lice
MDR bacteria (e.g., MRSA, VRE, VISA, VRSA)
infection or colonization

Scenarios with Known or Suspected Diseases or Pathogens Contact Precautions
MonkeypoxParainfluenza infection (infants, children)
Rotavirus (diapered or incontinent)
RSV infection (infants, children,immunocompromised) Rubella,
congenital
SARS
Staphylococcus aureus major skin,
wound or burn infection
Scabies

Scenarios with Known or Suspected Diseases or Pathogens Contact Precautions
Shigella (diapered or incontinent)Smallpox
Streptococcal (group A) major skin, burn or wound infection
Varicella
Viral hemorrhagic fevers
Yersinia enterocolitica enteritis
(diapered or incontinent)
Zoster (disseminated or immunocompromised)






Clinical ImmunologyDefense Mechanisms
Non ImmunologicalSkin
Mucous membrane
Saliva, tears
Respiratory cilia
Cough & expectoration
Gastric acidity
Peristalsis
Flash of urine
Vaginal acidity
Immunological
Complement system
Phagocytosis
Opsonization
Antibody Compl. Fixation
Neutralization
Lyses
Agglutination
Cell Mediated Immunity
Thank You