
Antipsychotics
Dr.Nasser A. H. Al-Harchan
Dr.Nasser A. H. Al-Harchan
Asst. Prof. of Pharmacology
College of Medicine
Baghdad University

Schizophrenia
Schizophrenia
n
n
Etiology
Etiology
n
Exact etiology unknown
n
Genetic predisposition
n
Intrauterine, birth or postnatal complications
n
Viral CNS infections
n
Environmental stressors (biochemical or social)
n
No evidence of association with poor
parenting

Schizophrenia
Schizophrenia
n
n
Pathophysiology
Pathophysiology
n
No consistent neuropathology or
biomarkers for schizophrenia
n
? Increased dopamine in mesolimbic
pathways causes delusions and hallucinations
n
? Dopamine deficiency in mesocortical and
nigrostriatal pathways causes negative
symptoms (apathy, withdrawal)
n
Hallocinogens produce effect through action
on 5-HT2 receptors

Schizophrenia
Schizophrenia
n
n
Antipsychotics
Antipsychotics
n
Typical / Conventional antipsychotics
n
Atypical antipsychotics
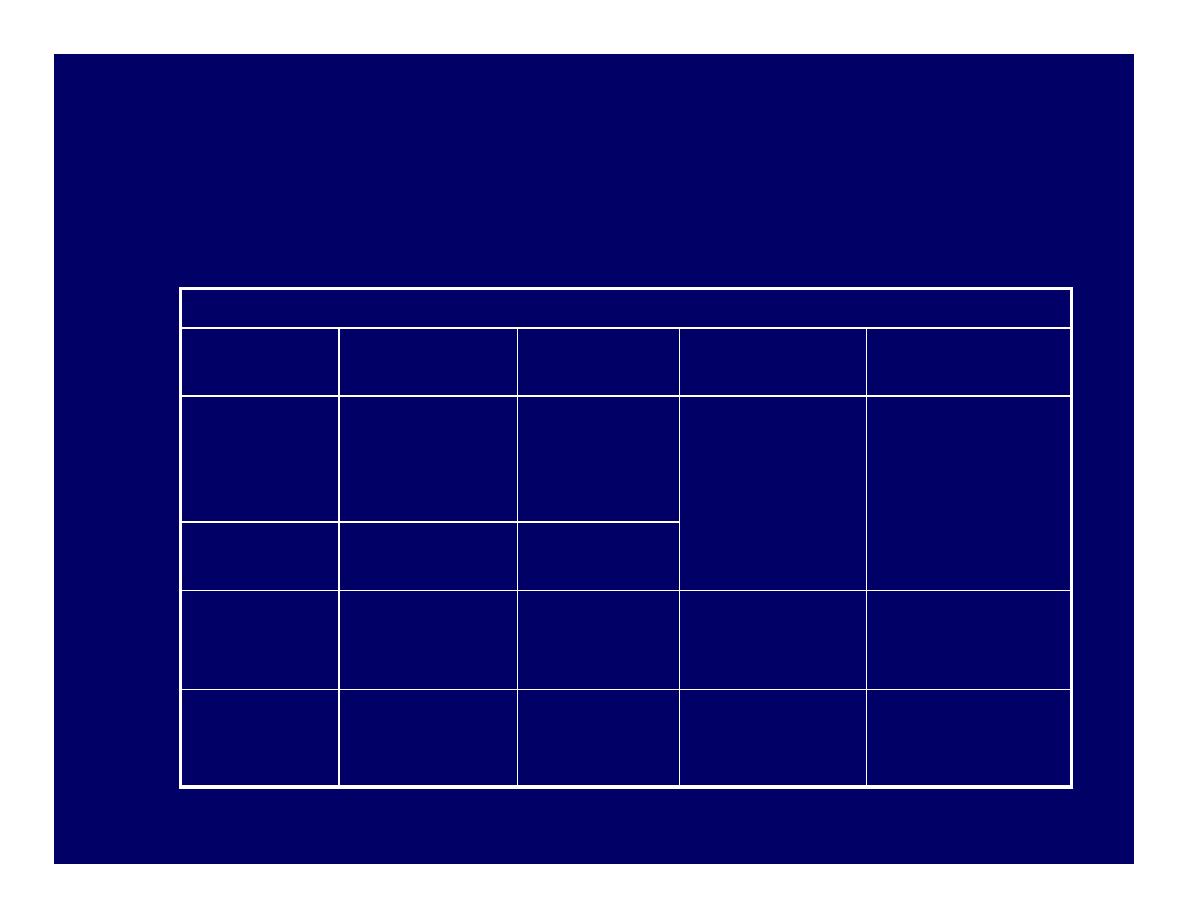
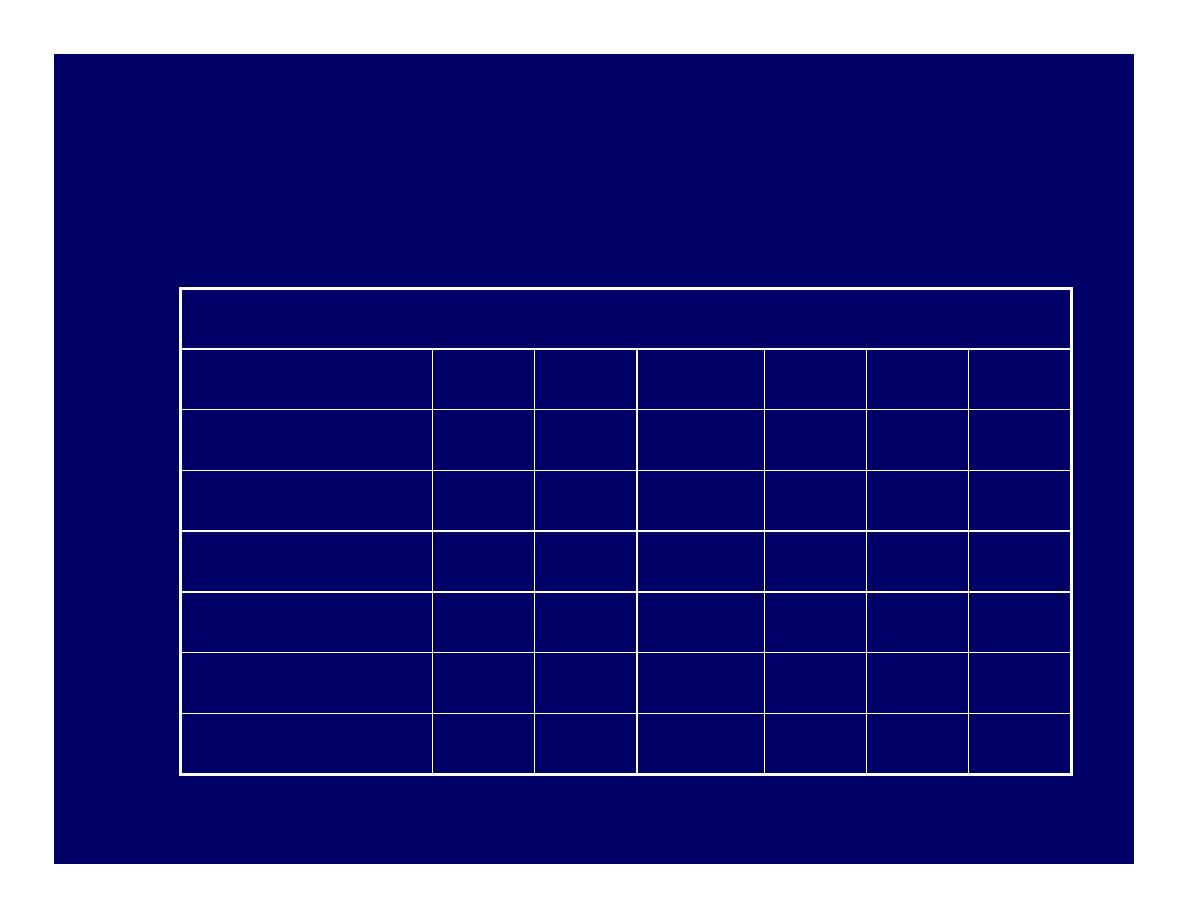
Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
Dopamine receptors in various tracks
Dopamine receptors in various tracks
Track
Track
Origin
Origin
Innervations
Innervations
Function
Function
Antipsychotic
Antipsychotic
effect
effect
Mesolimbic
Mesolimbic
Midbrain,
Midbrain,
Ventral
Ventral
tegmental
tegmental
Limbic
Limbic
structure,
structure,
nucleus
nucleus
accumbens
accumbens
Emotional and
Emotional and
intellectual
intellectual
ò
òHallucinations,
Hallucinations,
deulsions,
deulsions,
disordered
disordered
cognition
cognition
Mesocortical
Mesocortical Ventral
Ventral
tegmental
tegmental
Frontal
Frontal
cortex
cortex
Nigrostriatal
Nigrostriatal
Substantia
Substantia
nigra
nigra
Basal ganglia
Basal ganglia Extrapyramidal
Extrapyramidal
system
system
movement
movement
ñ
ñMotor
Motor
symptomatology
symptomatology
Tubero
Tubero--
infundubular
infundubular
Hypothalamus
Hypothalamus Pituitary
Pituitary
gland
gland
Regulate
Regulate
endocrine
endocrine
functions
functions
ñ
ñPlasma
Plasma
prolactin levels
prolactin levels

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Mechanism of action
Mechanism of action
n
Blocks receptors for dopamine,
acetylcholine, histamine and
norepinephrine
n
Current theory suggests dopamine2 (D2)
receptors suppresses psychotic symptoms
n
All typical antipsychotics block D2 receptors
n
Close correlation between clinical potency and
potency as D2 receptor antagonists

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Properties
Properties
n
Effective in reducing positive symptoms during
acute episodes and in preventing their
reoccurrence
n
Less effective in treating negative symptoms
n
Some concern that they may exacerbate negative
symptoms by causing akinesia
n
Higher incidence of EPS / sedation /
anticholinergic Adverse effects

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Potency
Potency
n
All have same ability to relieve symptoms
of psychosis
n
Differ from one another in terms of
potency
n
i.e. size of dose to achieve a given response
n
When administered in therapeutically
equivalent doses, all drugs elicit
equivalent antipsychotic response

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Low potency
Low potency
n
Chlorpromazine, thioridazine
n
n
Medium potency
Medium potency
n
Perphenazine
n
n
High potency
High potency
n
Trifluoperazine, thiothixene, fluphenazine,
haloperidol, pimozide
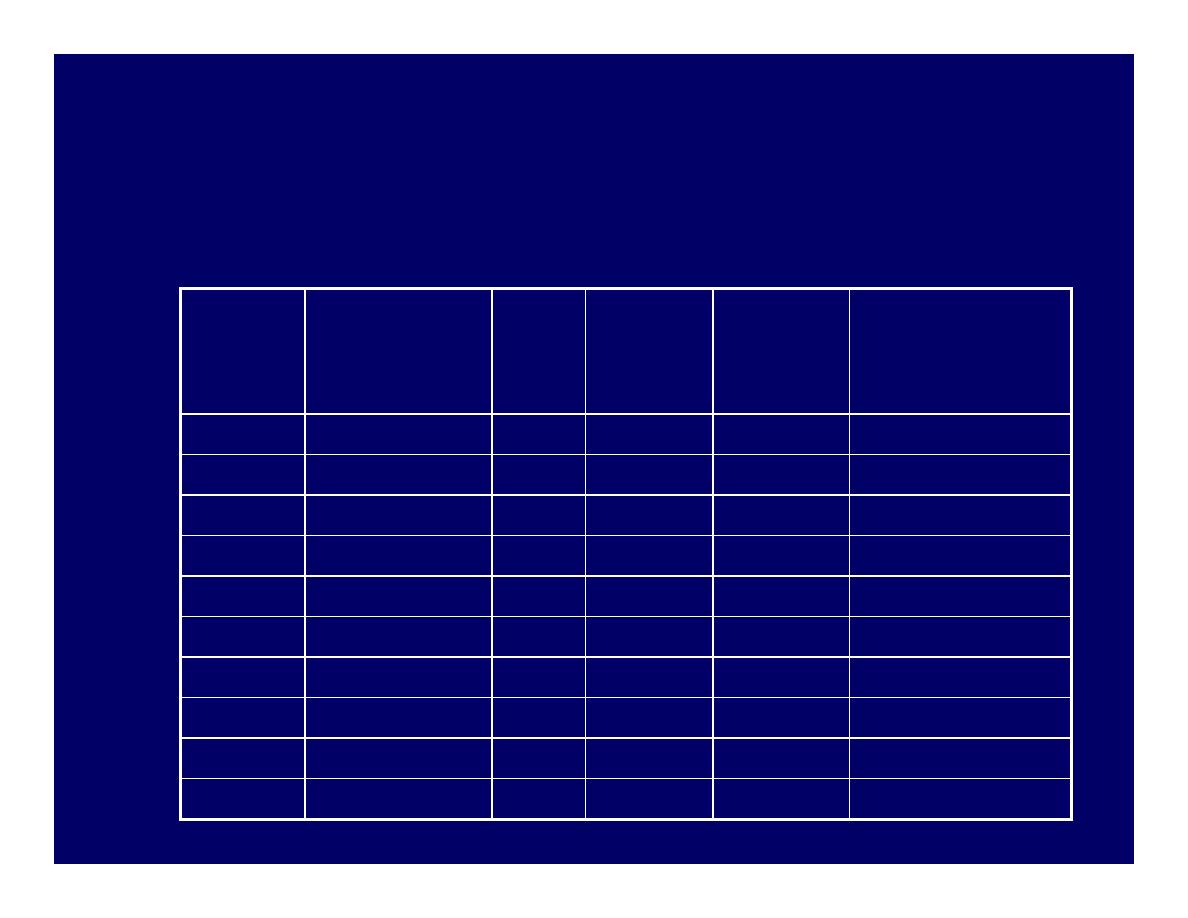
Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
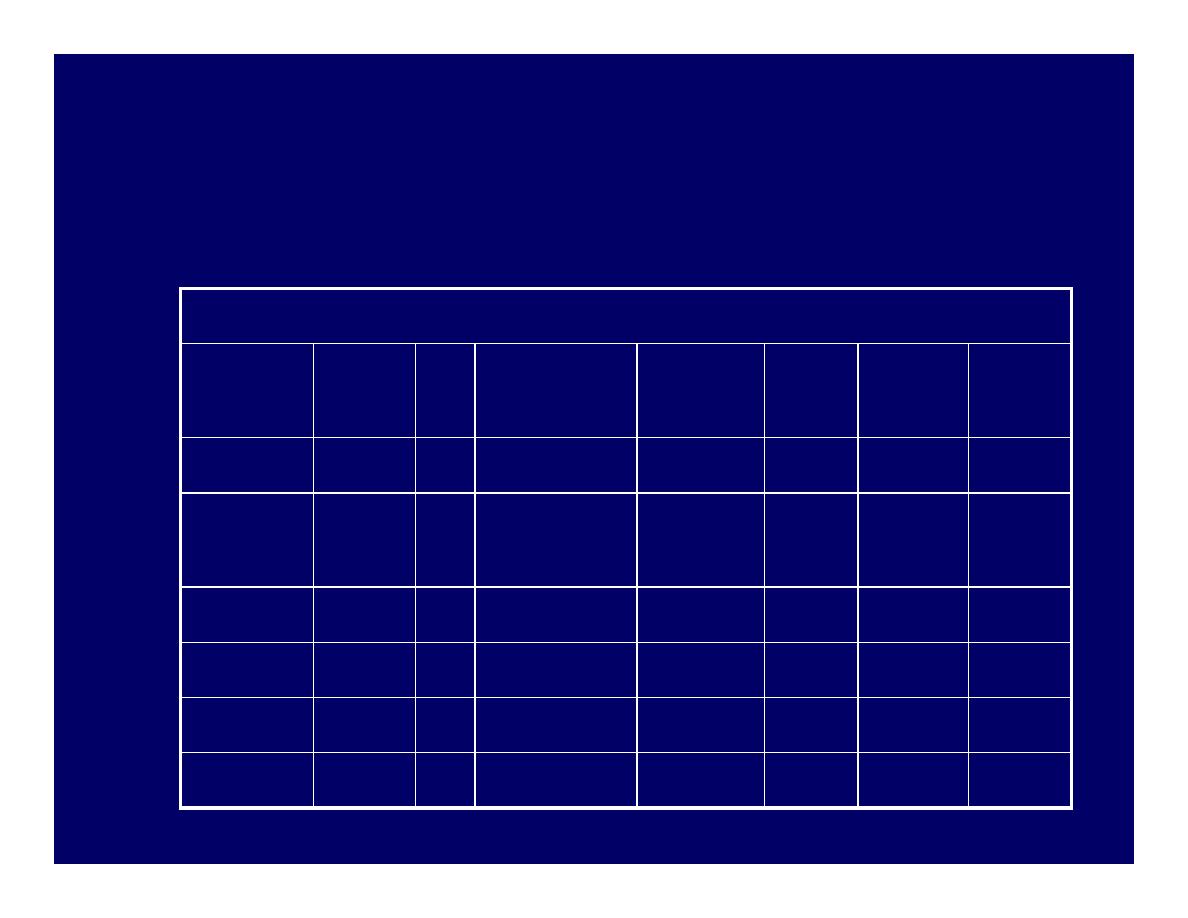
Potency
Potency
Drug
Drug
Equiv
Equiv
oral
oral
dose
dose
(mg)
(mg)
EPS
EPS
Sedation
Sedation
Anticholinergic s/e
Anticholinergic s/e
Low
Chlorpromazine 100
Moderate High
Moderate
Pericyazine
NA
Low
High
Low
Thioridazine
100
Low
High
High
Moderate Perphenazine
10
Moderate Moderate
Low
High
Trifluoperazine
5
High
Low
Low
Thiotheixene
2
High
Low
Low
Fluphenazine
2
High
Low
Low
Haloperidol
2
High
Low
Low
Pimozide
0.5
High
Moderate
Moderate
Sulpiride
200
Low
Moderate
Low
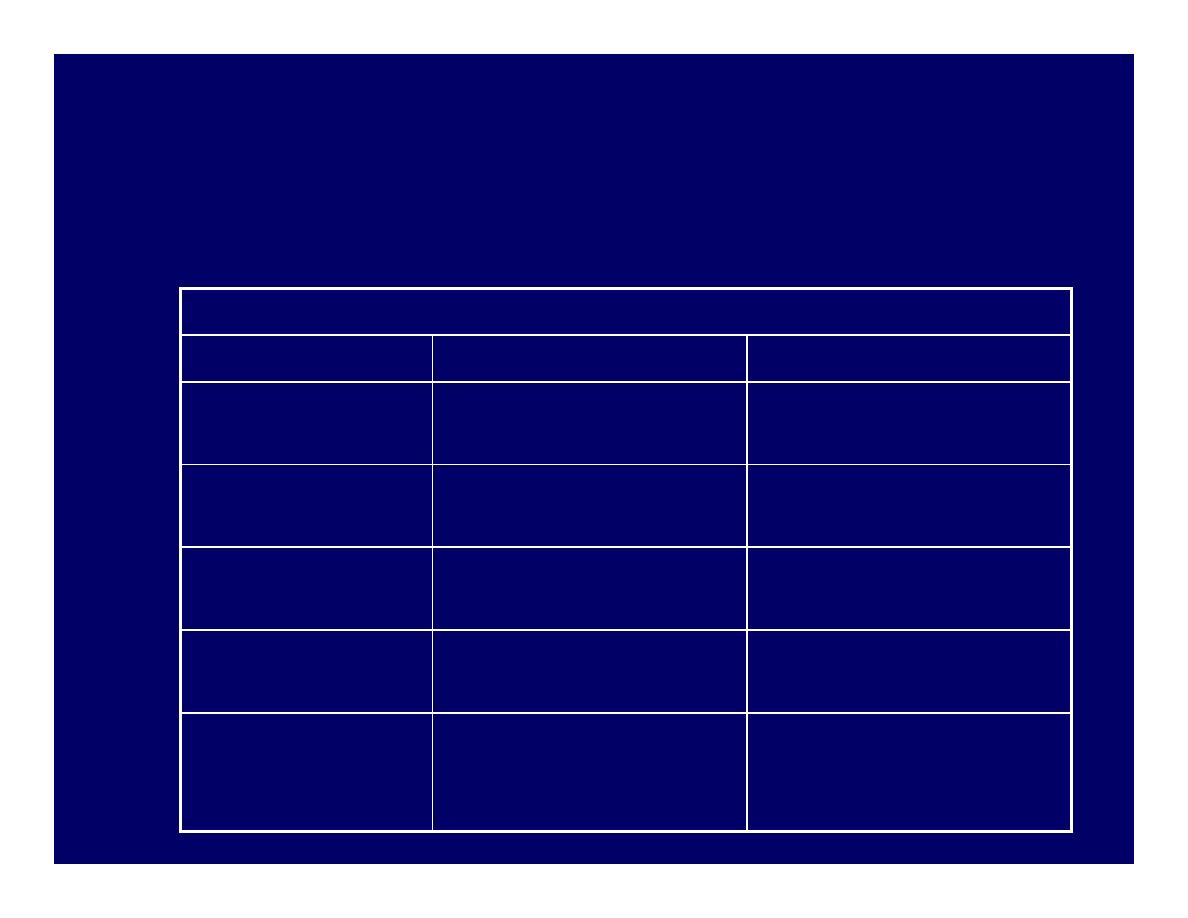
Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
Comparison of representative antipsychotics
Comparison of representative antipsychotics
Drug
Drug
Advantages
Advantages
Disadvantages
Disadvantages
Chlorpromazine
Chlorpromazine
Generic, inexpensive
Generic, inexpensive
Many adverse effects
Many adverse effects
(esp. autonomic)
(esp. autonomic)
Thioridazine
Thioridazine
Slight EPS, generic
Slight EPS, generic
Cardiotoxicity (QT
Cardiotoxicity (QT
prolongation)
prolongation)
Fluphenazine
Fluphenazine
Generic, depot
Generic, depot
available
available
(?)
(?) increased tardive
increased tardive
dyskinesia
dyskinesia
Thiothixene
Thiothixene
(?)
(?) decreased tardive
decreased tardive
dyskinesia
dyskinesia
Uncertain
Uncertain
Haloperidol
Haloperidol
Generic, injection and
Generic, injection and
depot A/V, few
depot A/V, few
autonomic s/e
autonomic s/e
Prominent EPS
Prominent EPS
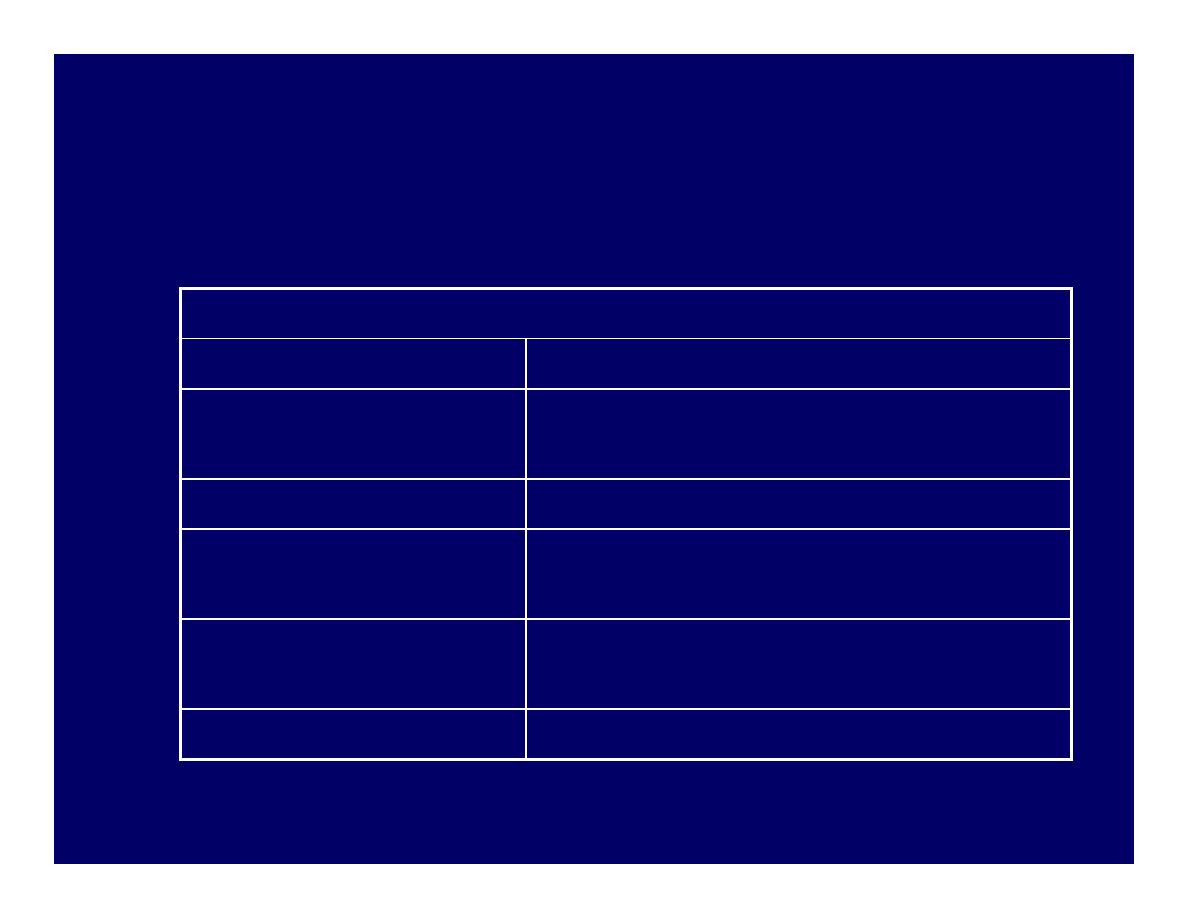
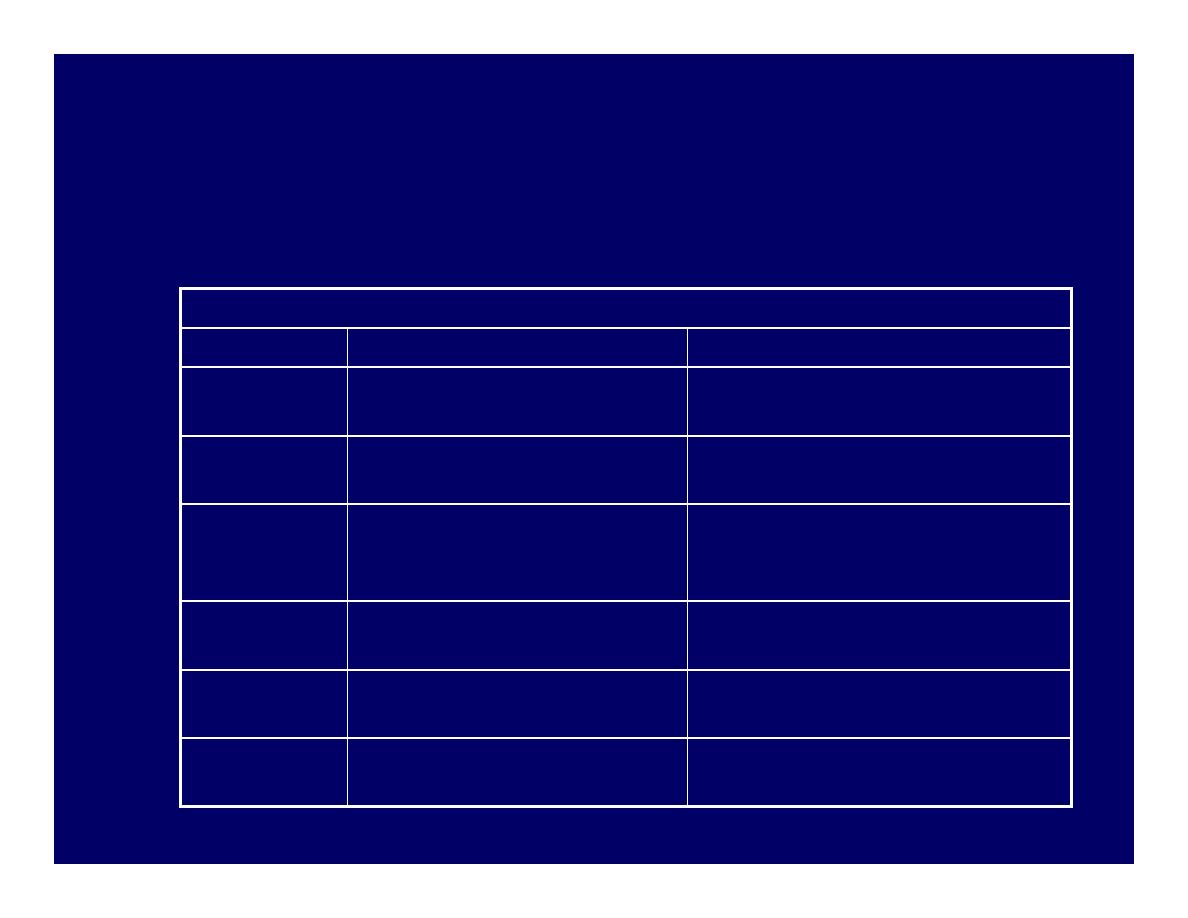
Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
Receptor blockade and Adverse effects
Receptor blockade and Adverse effects
Receptor type
Consequence of blockade
D2 dopaminergic
Extrapyramidal symptoms; prolactin
release
H1 histaminergic
Sedation
Muscarinic cholinergic Dry mouth, blurred vision, urinary
retention, constipation, tachycardia
Alpha1-adrenergic
Orthostatic hypotension; reflex
tachycardia
5-HT2 serotonergic
Weight gain

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Adverse effects
Adverse effects
n
Extrapyramidal symptoms (EPS)
n
Early reactions – can be managed with drugs
n
Acute dystonia
n
Parkinsonism
n
Akathisia
n
Late reaction – drug treatment unsatisfactory
n
Tardive dyskinesia (TD)
n
Early reactions occur less frequently with low potency
drugs
n
Risk of TD is equal with all agents

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Adverse effects
Adverse effects
n
Acute dystonia
n
Develops within a few hours to 5 days after first dose
n
Muscle spasm of tongue, face, neck and back
n
Oculogyric crisis (involuntary upward deviation of eyeballs)
n
Opisthotonus (tetanic spasm of back muscles, causing trunk
to arch forward, while head and lower limbs are thrust
backwards)
n
Laryngeal dystonia can impair respiration
n
Management
n
Anticholinergics (Benztropine, diphenhydramine IM/IV)
n
Lower or split dosing
n
Switch agent
n
Add scheduled benztropine / diphenhydramine with
antipsychotic

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Adverse effects
Adverse effects
n
Parkinsonism (neuroleptic induced)
n
Occurs within first month of therapy
n
Bradykinesia, mask-like facies, drooling, tremor,
rigidity, shuffling gait, cogwheeling, stooped posture
n
Shares same symptoms with Parkinson’s disease
n
Management
n
Centrally acting anticholinergics (scheduled benztropine
/ diphenhydramine / benzhexol with antipsychotics) and
amantadine
n
Avoid levodopa as it may counteract antipsychotic
effects
n
Switch to atypical antipsychotics for severe symptoms

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Adverse effects
Adverse effects
n
Akathisia
n
Develop within first 2 months of therapy
n
Compulsive, restless movement
n
Symptoms of anxiety, agitation
n
Management
n
Beta blockers (propranolol)
n
Benzodiazepines (e.g. lorazepam)
n
Anticholinergics (e.g. benztropine, benzhexol)
n
Reduce antipsychotic dosage or switch to low potency
agent

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Adverse effects
Adverse effects
n
Tardive dyskinesia (TD)
n
Develops months to years after therapy
n
Involuntary choreoathetoid (twisting, writhing,
worm-like) movements of tongue and face
n
Can interfere with chewing, swallowing and
speaking
n
Symptoms are usually irreversible

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Adverse effects
Adverse effects
n
Tardive dyskinesia (TD)
n
Management
n
Some manufacturers suggest drug withdrawal at earliest
signs of TD (fine vermicular movements of tongue) may
halt its full development
n
Gradual drug withdrawal (to avoid dyskinesia)
n
Use lowest effective dose
n
Atypical antypsychotic for mild TD
n
Clozapine for severe, distressing TD
n
Inconsistent results with
n
Diazepam, clonazepam, valproate
n
Propranolol, clonidine
n
Vitamin E

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Other Adverse effects
Other Adverse effects
n
Neuroleptic malignant syndrome (NMS)
n
Rare but serious reaction, 0.2% of patients on
neuroleptics
n
High fever, autonomic instability, mental status
changes, leaden rigidity, elevated CK, WBC,
myoglobinuria
n
Management
n
Discontinue antipsychotic
n
Paracetamol for hyperthermia
n
IV fluids for hydration
n
Benzodiazepines for anxiety
n
Dantrolene for rigidity and hyperthermia
n
Bromocriptine for CNS toxicity

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Other Adverse effects
Other Adverse effects
n
Neuroleptic malignant syndrome (NMS)
n
After symptom resolution
n
Some suggest to wait for at least 2 weeks before
resuming
n
Use lowest effective dose
n
Avoid high potency agents
n
Consider atypical antipsychotics
n
However, NMS has been reported from
patients taking clozapine, risperidone,
olanzapine and quetiapine

Typical / conventional
Typical / conventional
antipsychotics
antipsychotics
n
n
Other Adverse effects
Other Adverse effects
n
Prolactinemia
n
D2 receptor blockade decreases dopamine inhibition of
prolactin
n
Results in galactorrhea, amenorrhea, loss of libido
n
Managed with bromocriptine
n
Sedation
n
Administer once daily at bedtime
n
Seizures
n
Haloperidol has a lower risk of seizures
n
Anticonvulsants (beware or possible interaction with
antipsychotic)

Atypical antipsychotics
Atypical antipsychotics
n
n
Refers to newer agents
Refers to newer agents
n
n
Also known as
Also known as
n
“Serotonin-dopamine antagonists”
n
Postsynaptic effects at 5-HT2A and D2
receptors

Atypical antipsychotics
Atypical antipsychotics
n
n
Mechanism of action
Mechanism of action
n
Similar blocking effect on D2 receptors
n
Seem to be a little more selective, targeting the
intended pathway to a larger degree than the
others
n
Also block or partially block serotonin receptors
(particularly 5HT2A, C and 5HT1A receptors)
n
Aripiprazole: dopamine partial agonist (novel
mechanism)

Atypical antipsychotics
Atypical antipsychotics
n
n
Properties
Properties
n
Available evidence to show advantage for
some (clozapine, risperidone, olanzapine)
but not all atypicals when compared with
typicals
n
At least as effective as typicals for
positive symptoms
n
May be more efficacious for negative and
cognitive symptoms (still under debate)

Atypical antipsychotics
Atypical antipsychotics
n
n
Properties
Properties
n
Less frequently associated with EPS
n
More risk of weight gain, new onset
diabetes, hyperlipidemia
n
Novel agents, more expensive

Atypical antipsychotics
Atypical antipsychotics
n
n
Potency
Potency
n
All atypical antipsychotics are equally
effective at therapeutic doses
n
Except clozapine
n
Most effective antipsychotic
n
For resistant schizophrenia
n
2
nd
line due to life-threatening side effect
Atypical antipsychotics
Atypical antipsychotics
Relative receptor
Relative receptor--binding of atypical antipsychotics
binding of atypical antipsychotics
Drug
Drug
D
D11
D
D22
55--HT
HT22
a
a11
M
M11
H
H11
Clozapine
Clozapine
++
++
++
++
+++
+++
+++
+++ +++
+++ +
+
Risperidone
Risperidone
--
+++
+++ +++
+++
+++
+++ --
+
+
Olanzapine
Olanzapine
++
++
++
++
+++
+++
++
++
+++
+++ ++
++
Quetiapine
Quetiapine
--
+
+
++
++
+++
+++ +
+
+
+
Ziprasidone
Ziprasidone
+/
+/--
++
++
+++
+++
++
++
--
+
+
Aripiprazole
Aripiprazole
+
+
+++
+++ ++
++
++
++
--
+
+
Atypical antipsychotics
Atypical antipsychotics
Comparison of representative atypical antipsychotics
Comparison of representative atypical antipsychotics
Drug
Drug
Advantages
Advantages
Disadvantages
Disadvantages
Clozapine
Clozapine
For treatment
For treatment--resistant cases,
resistant cases,
little EPS
little EPS
Risk of fatal agranulocytosis
Risk of fatal agranulocytosis
Risperidone
Risperidone
Broad efficacy, little or no EPS
Broad efficacy, little or no EPS
at low doses
at low doses
EPS and hypotension at high
EPS and hypotension at high
doses
doses
Olanzapine
Olanzapine
Effective with positive and
Effective with positive and
negative symptoms, little or
negative symptoms, little or
no EPS
no EPS
Weight gain
Weight gain
Quetiapine
Quetiapine
Similar to risperidone, maybe
Similar to risperidone, maybe
less weight gain
less weight gain
Dose adjustment with associated
Dose adjustment with associated
hypotension, bd dosing
hypotension, bd dosing
Ziprasidone
Ziprasidone
Perhaps less weight gain than
Perhaps less weight gain than
clozapine, Inj A/V
clozapine, Inj A/V
QT prolongation
QT prolongation
Aripiprazole
Aripiprazole
Less weight gain, novel
Less weight gain, novel
mechanism potential
mechanism potential
Uncertain
Uncertain
Atypical antipsychotics
Atypical antipsychotics
Relative incidence of Adverse effects
Relative incidence of Adverse effects
Drugs
Drugs
Sedatio
Sedatio
nn
EPS
EPS Anticholinergic
Anticholinergic
Orthostasis
Orthostasis Seizure
Seizure
Prolactin
Prolactin
elevation
elevation
Weight
Weight
gain
gain
Clozapine
Clozapine
++++
++++
+
+
++++
++++
++++
++++
++++
++++
00
++++
++++
Risperidone
Risperidone
+++
+++
+
+
++
++
+++
+++
++
++
0
0 to
to
++++
++++
++
++
Olanzapine
Olanzapine
+++
+++
+
+
+++
+++
++
++
++
++
+
+
+++
+++
Quetiapine
Quetiapine
+++
+++
+
+
++
++
++
++
++
++
00
++
++
Ziprasidone
Ziprasidone
++
++
+
+
++
++
++
++
++
++
00
+
+
Aripiprazole
Aripiprazole
++
++
+
+
++
++
++
++
++
++
00
+
+

Atypical antipsychotics
Atypical antipsychotics
n
n
11
st
st
line atypical antipsychotics
line atypical antipsychotics
n
All atypicals except clozapine
n
NICE recommendations
n
Atypical antipsychotics considered when choosing 1
st
line treatment of newly diagnosed schizophrenia
n
Treatment option of choice for managing acute
schizophrenic episode
n
Considered when suffering unacceptable Adverse
effects from a conventional antipsychotic
n
Changing to an atypical not necessary if typical
controls symptoms adequately and no unacceptable
Adverse effects

Atypical antipsychotics
Atypical antipsychotics
n
n
22
nd
nd
line atypical antipsychotic
line atypical antipsychotic
n
Clozapine
n
Most effective antipsychotic for reducing symptoms
and preventing relapse
n
Use of clozapine effectively reduce suicide risk
n
1% risk of potentially fatal agranulocytosis
n
Acute pronounced leukopenia with great reduction in
number of neutrophil
n
Clozapine should be introduced if schizophrenia is
inadequately controlled despite sequential use of 2 or
more antipsychotic (one of which should be an atypical)
each for at least 6-8 weeks)

Atypical antipsychotics
Atypical antipsychotics
n
n
Clozapine
Clozapine
n
Rare cases of myocarditis and cardiomyopathy
n
Fatal
n
Most commonly in first 2 months
n
CSM recommendations
n
Physical exam and medical history before starting
n
Persistent tachycardia esp. in first 2 weeks should
prompt observation for cardiomyopathy
n
If myocarditis or cardiomyopathy, stop clozapine
n
Inform patients for unexplained fatigue, dyspnea,
tachypnea, chest pain, paipitation and ask them to
report these signs and symptoms immediately

Non
Non--antipsychotic agents
antipsychotic agents
n
n
Benzodiazepines
Benzodiazepines
n
Useful in some studies for anxiety, agitation,
global impairment and psychosis
n
Schizophrenic patients are prone to BZD abuse
n
Limit use to short trials (2-4 weeks) for
management of severe agitation and anxiety
n
n
Lithium
Lithium
n
Limited role in schizophrenia monotherapy
n
Improve psychosis, depression, excitement, and
irritability when used with antipsychotic in some
studies