1
Parasitology
.د
هيفاء
المحاضرة ا
ثانية
Blood flukes (Schistosomes)
There are five main species of schistosomes infect human:
1- S. haematobium: occurs primarily in the Old World. Nearly all of Africa and
portion of Middle East, including Iraq, Saudi Arabia, and Iran which considered as
endemic regions.
2- S. mansoni: in Africa esp. Egypt, Sudan and Libya, Arabian Peninsula, and
Central and South America.
3- S. japonicum: is limited to the Far East (China, Indonesia, and Philippines).
General features of schistosomes from other trematodes
1-have separated sexes (diecious).
2-adults live in blood vascular system.
3-adult digestive system has no muscular pharynx, but characterized by formation
of single intestinal canal by the union of bifurcated intestinal caeca.
4-production of non-operculated eggs (eggs with spine).
5-no redia formation.
6-have forked tailed cercariae (infective stage to man).
7-no metacercariae formation.
8-infect human by penetration of unbroken skin by cercariae.
2
Morphology
Adult worms are elongated and resemble roundworms, apparently as an
adaptation to living in blood vessels. The male worm is long and has a cylindrical
appearance but it is actually flattened behind the ventral sucker ,because it is
incurved ventrally to form a gynaecophoric canal in which the longer and more
slender female rests and projecting free at each end, but enclosed in the middle.
Both male and female worms are provided with oral and ventral suckers; in the
males the ventral sucker is large and powerful. The digestive tract has no pharynx,
and the esophagus forks just anterior to the ventral sucker, but the forks reunite
in the middle portion of the body to continue as a single tube. The male worm has
several testes just behind the ventral sucker. The female has an elongated ovary
situated in the fork where the intestinal caeca rejoin. Anterior to the ovary is a
straight uterus contains a small number of eggs. Schistosomes live for many years
in human.
S. haematobium S. mansoni S. japonicum
Adult
-Habitat vesicle plexus inf. mesenteric vein sup. mesenteric vein
(veins of bladder) (veins of large intestine) (veins of small intestine)
-Size*: male 10-14 × 0.9mm 6-12 × 1.1mm 10-20 × 0.5mm
female 16-20 × 0. 10-20 × 0.16mm 20-30 × 0.3mm
-integument with fine with coarse smooth
tuberculation tuberculation (no tuberculation)
-Caeca* reunite late reunite early reunite very late
(united intestine)* short long very short
-Size, arrangment 4-5 6-9 (7) 6-8 (7)

3
and No. of testes Small small, clustered large , linear
-Position of ovary post. 1/2 ant. 1/2 middle
-Uterus* long with 10-50 short with 1-4 long with 50-200
Ova ova ova
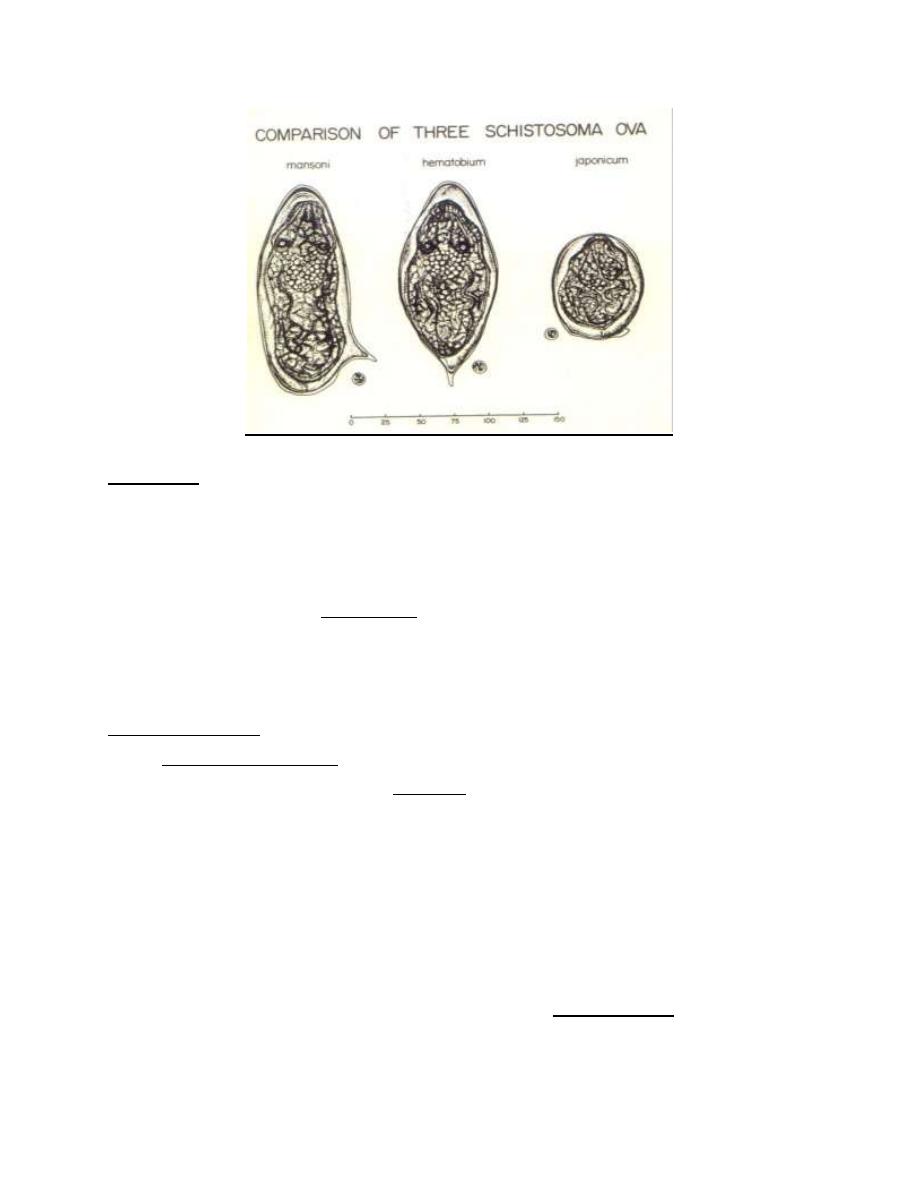
Egg
-Shape oval with terminal oval with lateral round with short
spine spine lateral spine
-Size (µ)* 150 × 62 140 × 61 85 × 60
-Mode of voiding Urine feces feces
-React. to Ziehl
Neelsen stain* negative positive positive
Snail (I . H) Bulinus trancatus Biomphalaria Oncomelania
في الجدول تعني لالطالع فقط* ةملاع :ةظحلام
Schistosomas in copula
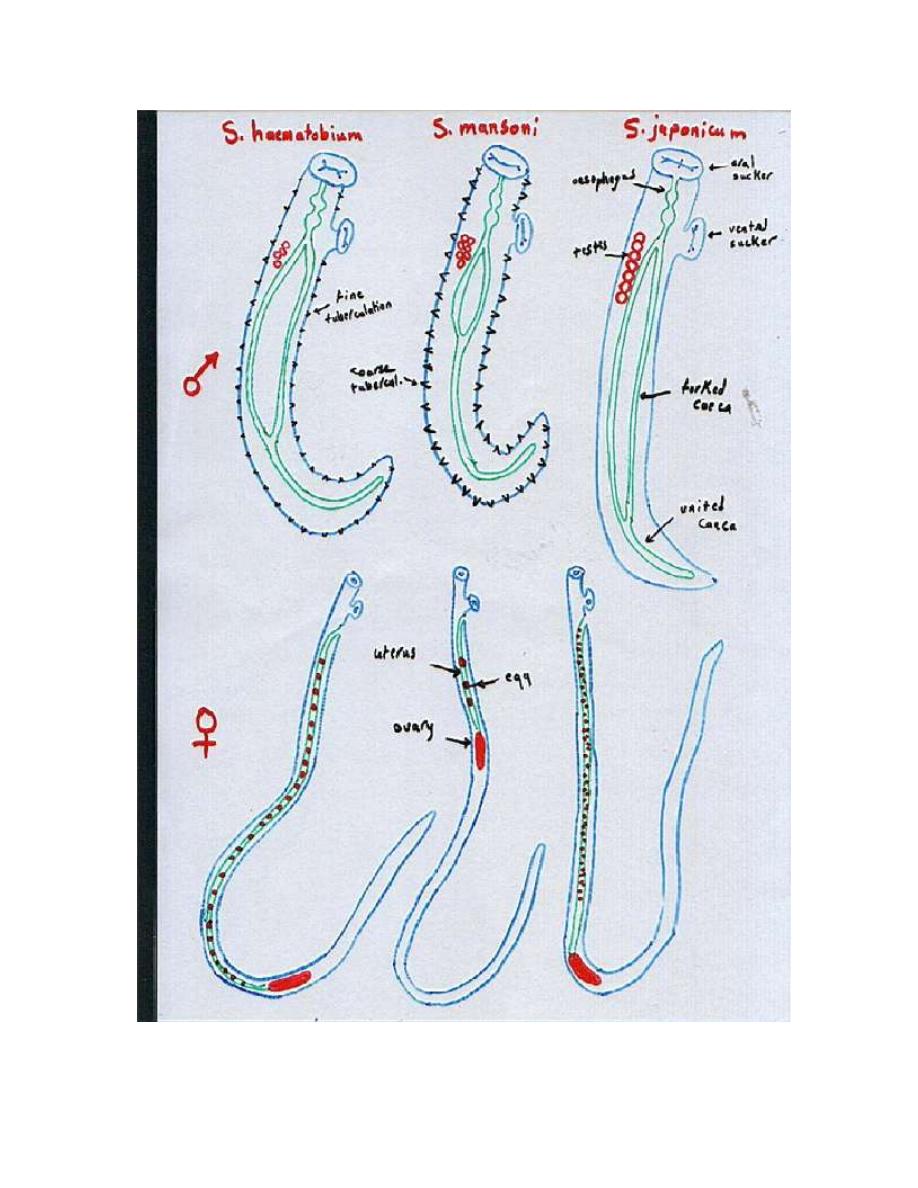
4
Morphology of both male and female of Scistosoma haematobium,S.mansoni and
S. japonicum
5
Life cycle
Schistosomes have indirect life cycle which involves 2 hosts, the definitive
(vertebrate) and the intermediate (invertebrate – snail-). Schistosome eggs are
passed in urine (S. haematobium) or feces (S. mansoni and S. japonicum) and
contain a fully mature miracidium (1
st
larval stage). Eggs hatch by rupture if
liberated into fresh water. The miracidium that escape swims by cilia in search of
an appropriate snail host. If successful, it penetrates the snail. In a susceptible
snail, the miracidium loses its outer ciliated epidermal layer and develops into a
mother sporocyst (2
nd
larval stage), then this sporocyst burst out and give rise to
many daughter sporocysts (3
rd
larval stage), then each daughter sporocyst filled
with the final larval stages, the circariae. Thus one miracidium can give rise to
thousands of cercariae, all of the same sex.
The cercariae begin to emerge from snail few (4-7) weeks after the snail infection,
and they can survive in fresh water for almost 74 hours. When man enters the
water, infection takes place by direct penetration of the cercariae through the
skin of man, often between the hair follicles, by means of 1-the anterior spines
and 2-the cytolytic secretion of the cephalic glands. The tail is shed in the
penetration process and immature schistosomes (schistosomula) remain in the
subcutaneous tissues for about 2 days then enter peripheral lymphatics or venous
vessels. These are carried to the lung and from the lung to the portal vessels (liver
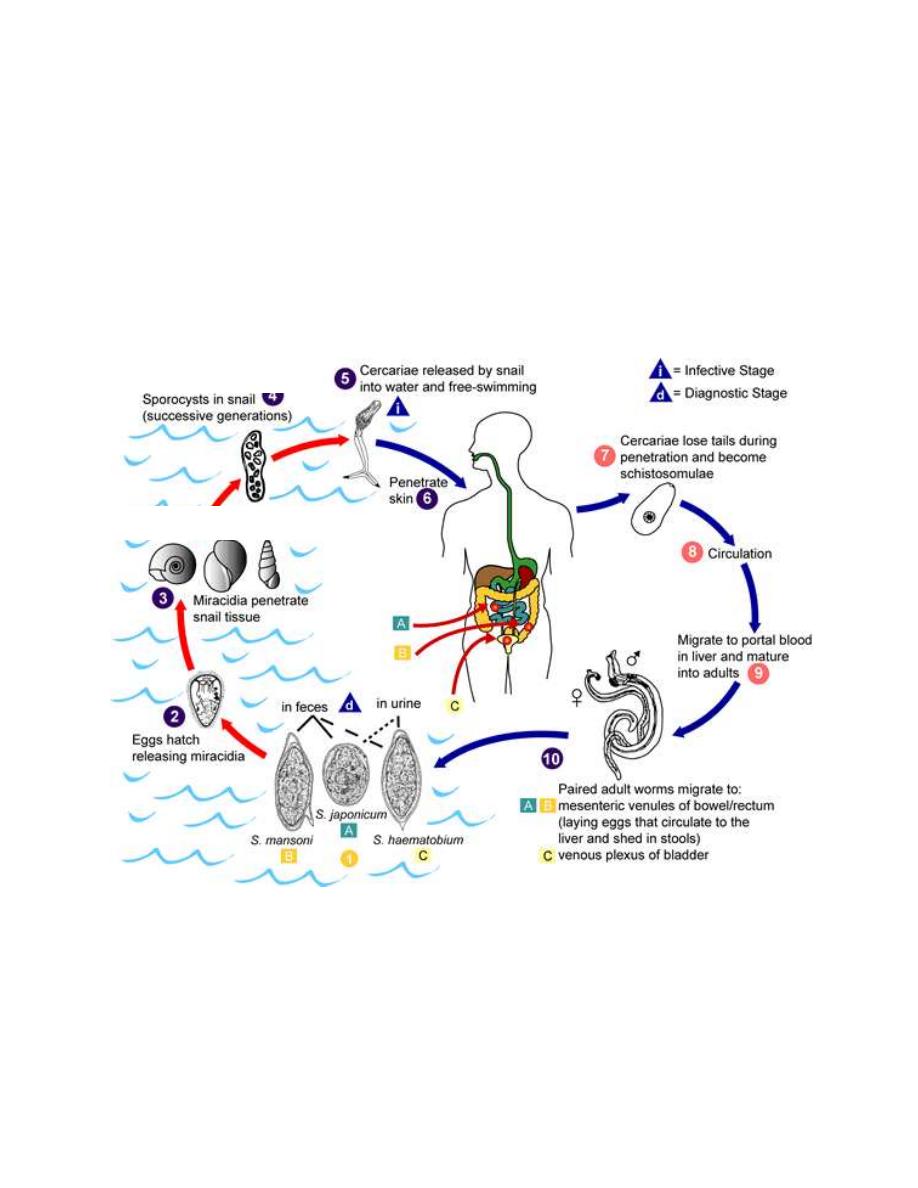
6
sinusoid) where they begin their growth into adult schistosomes (maturation in
the liver sinusoid takes about 6 weeks) which mate and remain in pairs. Two
weeks or longer after maturation to adults, the maturing worms commence a
migration against the flow of the blood in the portal system to their final location
in mesenteric veins (S. mansoni and S. japonicum) or vesicular veins (S.
haematobium). Eggs of (S. mansoni and S. japonicum) appear in the stools 25-28
days after the penetration of cercariae and those of S. haematobium in the urine
after 54-84 days. The lifespan of the adult worm ranges from 5 to 10 years.
Life cycle of Schistosoma Species
Oncomelania Bulinus Biomphalaria
Mother and daughter
7
-The reservoir host
1-S. haematobium: humans are the only important host.
2-S. mansoni: humans are apparently the only important host, but rodents may
carry infection in some areas.
3-S. japonicum: many domestic animals (cats, dogs, cattles, horses and pigs) as
well as some wild animals.
-The intermediate host
1-S. haematobium and S. mansoni: aquatic snails
2- S. japonicum: amphibious (semiaquatic) snails.
Pathogenesis and clinical features
The pathogenesis of human schistosomiasis is mainly related to egg deposition
and liberation of antigens of adult worms and eggs.
The body structure of the schistosomes seems clearly an adaptation to an
intravascular existence. The females leave the male worms to deposit their eggs
in small venules close to the lumen of the intestine or bladder. The worms dilate
the vessels when they penetrate it for oviposition and withdraw as the eggs are
laid, so that the eggs are wedged firmly into the small vessels. Sharp spines on the
eggs of S. mansoni and S. haematobium probably assist in the retention in the
blood vessels. An enzyme elaborated by the miracidium diffuses through the egg
shell and helps to digest the overlying tissue. The action of this enzyme, together
with necrosis of the tissue caused by pressure and the effect of the spine, works
to liberate the egg from the tissues into the lumen of the intestine or bladder.
Infected persons with schistosomes may be asymptomatic or may manifest a
spectrum of disease condition.
-Clinical manifestations of schistosomiasis
: are divided into
schistosome dermatitis, acute schistosomiasis, and chronic schistosomiasis.
-Schistosome dermatitis (swimmer’s itch)
Many schistosome cercariae that ordinary infect birds and semiaquatics mammals
are capable of penetration into human skin but not of producing a permanent

8
infection. Fresh-water lakes as well as some marine beaches are plagued by the
presence of cercariae of the blood flukes of aquatic birds, which cause dermatitis
known as swimmer’s itch. Schistosome dermatitis or swimmer's itch is seen
mainly when avian cercariae penetrate the skin and are destroyed. This
manifestation is not common and milder in human schistosomiasis. Schistosome
dermatitis is a sensitization phenomenon, because it occurs in previously exposed
persons. The cercariae are destroyed in the epithelial layers of the skin. They
evoke an acute inflammatory response with edema, early infiltration of
neutrophils and lymphocytes, and later invasion of eosinophils. A pruritic papular
rash occurs within 24 hours after penetration of cercariae, reaching maximal
intensity in 2 to 3 days.
-Acute schistosomiasis, or Katayama fever
Acute schistosomiasis, or Katayama fever occurs with the beginning of
oviposition, usually 20 to 50 days after primary exposure and infection with S.
mansoni and S. japonicum. It rarely follows infection with S.haematobium.
Although asymptomatic in endemic areas, acute schistosomiasis is becoming a
frequent and major clinical problem in nonimmune individuals from urban regions
who are exposed for the first time to a heavy infection in an endemic area. This
febrile condition is thought to be a hypersensitivity reaction to schistosomal
antigens. Patients complain of a flu like illness with fatigue, headache, arthralgia
and night sweats, smetimes with hepatosplenomegaly, cough, dyspnea and chest
pain. Acute schistosomiasis is a self-limiting condition and most symptoms resolve
without any treatment within 4-6 weeks. Acute disease is more frequently
observed in individuals living outside the endemic areas of schistosomiasis,
because modulation of the immune response by antigens or idiotypes transferred
from mother to child decreases the frequency of this manifestation in subjects
living in endemic areas.