1
Lecture: 2
Parasitology
ﺩ.ﻫﻴﻔﺎء ﺩﺍﻭﺩ
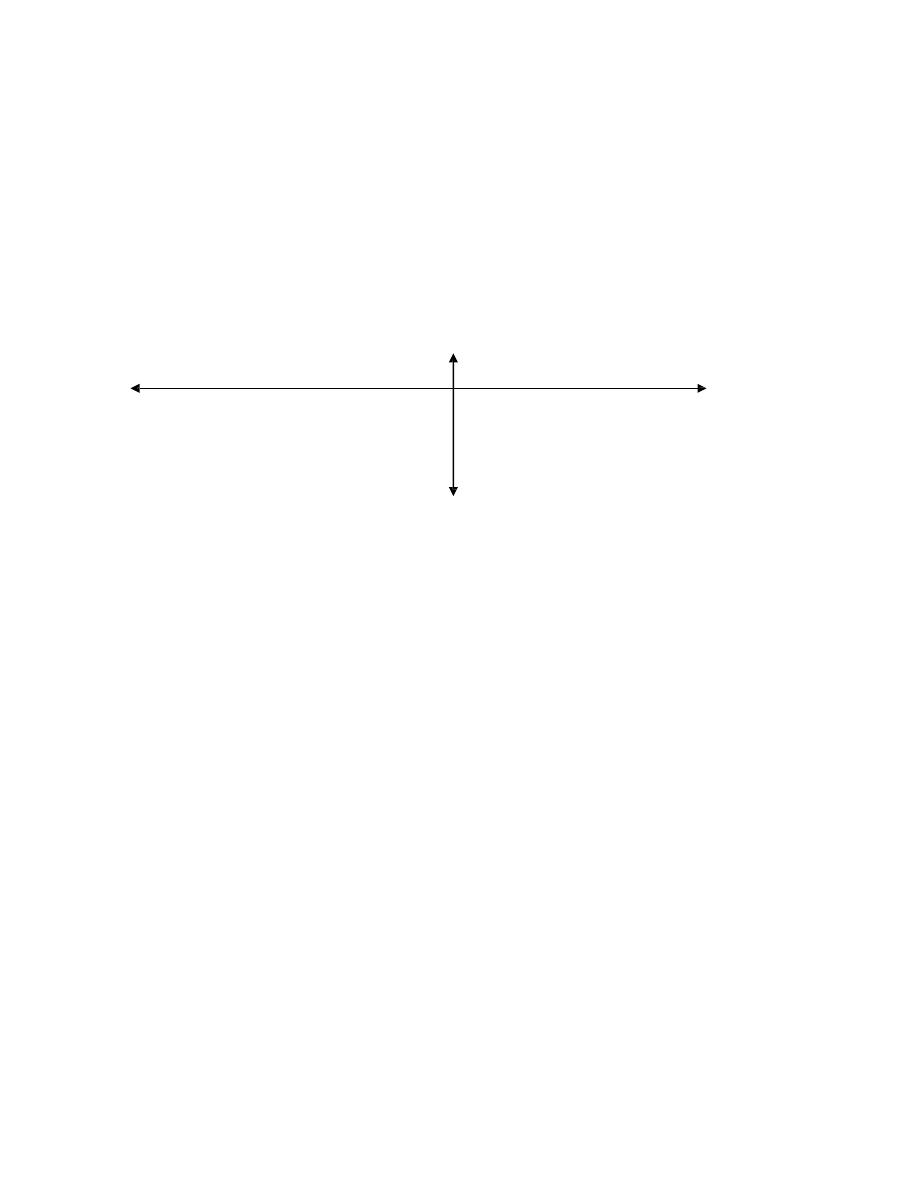
Cutaneous leishmaniasis
Old World cutaneous leishmaniasis (oriental sore) also called Delhi
boil, Baghdad boil, Aleppo boil, is produced by Leishamnias belonging
to Leishmania tropica complex. There are 3 serologically and
biochemically distinct species of L. tropica complex:-
1- L. tropica
2- L. major
3- L. aethiopica
All are transmitted by sand flies belonging to the genus Phlebotomus.
1- L. tropica: also known as L. tropica minor.(causes dry sore or
urban cutaneous leishmaniasis).
• Produce chronic disease that if not treated, lasts for year or
longer.
• with 2month – 3year incubation period
• It is characterized by the production of dry lesions that
ulcerate only after several months
• Lesions are usually single and occur primarily on the face.
• It is found in urban areas, it is found in Iraq and around the
Mediterranean basin and in Asia Minor, Afghanistan, India and
Kenya.
• The dog may be a natural host, but it is not thought to be an
effective reservoir for humans.
2- L. major: also called L. tropica major (causes wet sore or rural
cutaneous leishmaniasis).

2
•Produces an acute infection with duration of 3-6 months.
•With as little as 2 weeks incubation period.
•The lesions occur primarily on the lower limb.
•The lesions are moist and tend to ulcerate very early.
•There may be secondary or satellite lesions.
•
L. major occurs in Asia Minor, Middle East (Iran, Syria, Palestine
and Jordan) and in north and middle Africa.
•It is primarily a disease of rural areas.
•Reservoir hosts (Rodents) are important source of human
infection.
3- L. aethiopica(causes diffuse cutaneous leishmaniasis):
•Produces a chronic disease similar to that caused by L. tropica.
•Seen in the high lands of Ethiopia and in Kenya and possibly in
south Yemen.
•The Rock hyrax is a reservoir host of this specie
Symptoms
The first sign of the infection is a small red papule, which may itch
intensely and grow to 2 cm or more in diameter. In L. major infection,
the papule is covered with serous exudates (moist lesion) and
ulcerates early.
The papules are dry (dry lesions) and ulcerate only after several
months in L. tropica and L. aethiopica infection.
In uncomplicated cases there are no systemic manifestations and since
the disease is self-limiting, the patient seldom seeks medical assist.
Ulcer may associate with local disfiguration, pyogenic complication,
pain and some time septicemia.
Although the usual cutaneous lesion (dry or moist)
healsspontaneously, in certain instances such healing does not occur
by itself.
3
These cases (no spontaneous healing) may be considered to represent
the two poles of the spectrum of response:
1- Anergy
2- Hypersensitivity
(Spontaneous healing)
(Wet) moist lesion
Anergy
hypersensitivity
(Diffuse cutaneous leishmaniasis)
(leishmaniarecidiva)
Dry lesion
1- The anergic patient is incapable to produce a response to
infection, which therefore (amastigotes) can proliferate
indefinitely and forming many lesions filled with parasites. this
type of disease , known as diffuse cutaneous leishmaniasis is
probably the results of :
a) A deficient cell-mediated immunity.
b) Some characteristics of the parasite itself, as it is seen primarily
in infections caused by L.aethiopicaand L.Mexicana.
2- The hypersensitive patient is capable of excellent antibody and
cellular responses but cannot completely eliminate the parasites,
so as the central lesion heals, active peripheral ones continue to

4
form. This type of response known as leishmaniasisrecidiva , may
be seen with any of the cutaneous leishmaniasis.
Pathogenesis
When the bite of infected sand fly liberate promastigotes into the skin
→ the parasite proliferates as amastigotes in the macrophages and
other endothelial cells of the capillaries and small blood vessels of
immediate area →lyses of the amastigotes occurs following activation
of the macrophages by sensitized lymphocytes → a granulomatous
reaction results in the formation of a localized nodule → which
ulcerate when the blood supply to the area is compressed by the
parasite-induced damage → a pyogenic infection develops in the open
ulcer bed, and as host immunity increase → the ulcer heals.
Resistance to re-infection
Resistance to re-infection with the same species following primary
infection is nearly absolute.Infection with L.major protects the host
against subsequent L. tropica infection, but infection with L.tropica
does not counter the same immunity to subsequent challenge with L.
major.
Mode of transmission
1- Insect bite: a main mode of transmission (vector born
transmission).
2- Blood transfusion: a rare mode of transmission.
Diagnosis
1- Usually made in endemic areas on clinical grounds
2- Microscopic detection of amastigotes (L.D. bodies) within large
monocytic cells in Giemsa stained smear obtained by aspiration of
fluid from beneath the ulcer bed, especially its active borders.

5
Scraping taken from the ulcer surface do not reveal the
organisms, which are destroyed in areas secondarily infected with
bacteria.
3- Culture: on NNN (Novy-MacNeal-Nicolle) media or other media.
Culturing of material obtained by aspiration or biopsy may
demonstrate promastigote forms.
4- Animal inoculation: aspirate or biopsy material may be inoculated
subsequently into the nose of a hamster and the animal watched
for nasal inflammation.
5- Leishmanin skin test (Montenegro test): involves the forearm
intradermal injection of 0.1 ml suspension of killed promasitigote,
this test is used to measure delayed hypersensitivity. Positive
result is indicated by an induration of 5mm or more in 48-72
hours. In cutaneous leishmaniasis this test is positive.
6- Immunological test (serology): has limited role in diagnosis
because patient shows no detectable level of circulating
antibodies.
Treatment
1- Sodium stibogluconate (Pentostam)
2- Pentamidine (isothionate)
3- Meglumineantimoniate
4- Amphotericin B
6
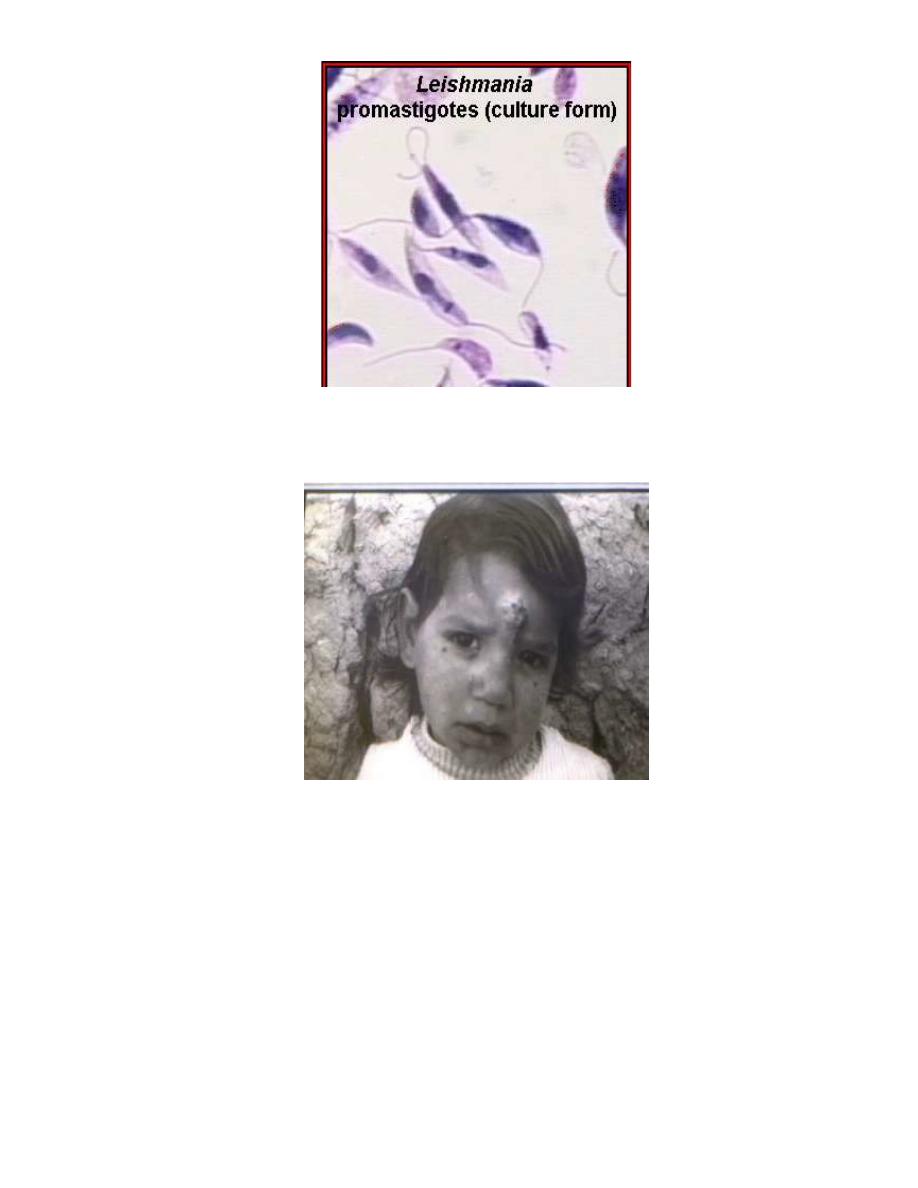
Dry sore (Urban cutaneous leishmaniasis)
7
Wet sore (Rural cutaneous leishmaniasis)