1
Immunology
____________________________________________________________________
Lec. 4
ﺩ. ﻋﺎﺋﺩﺓ ﺍﻟﺩﺭﺯﻱ
Type II hypersensitivity:
Ab-dependent cytotoxic H.S.
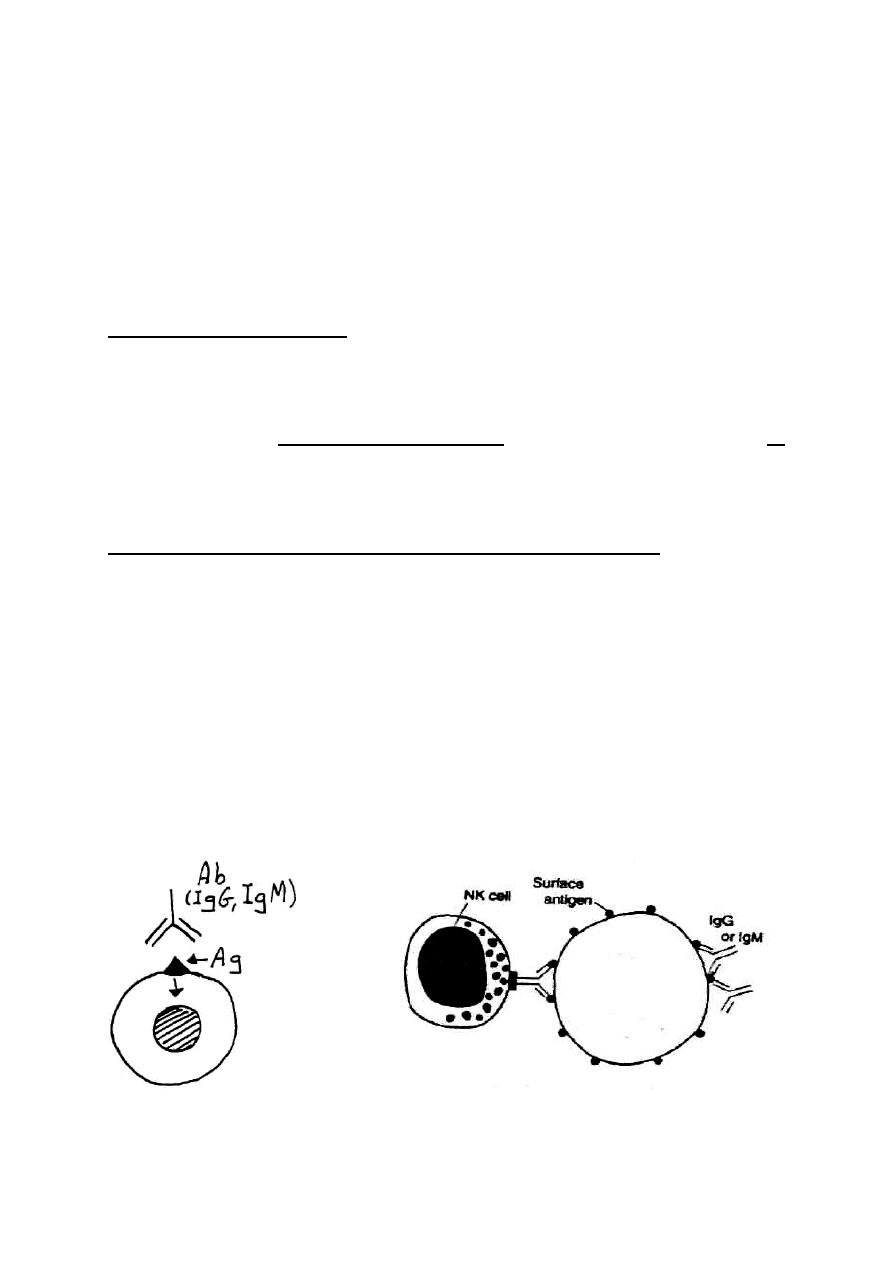
This reaction is initiated by Ab - either IgG or IgM - reacting with cell
bound Ag &, the reaction results in either destruction of target cell or
functional alteration.
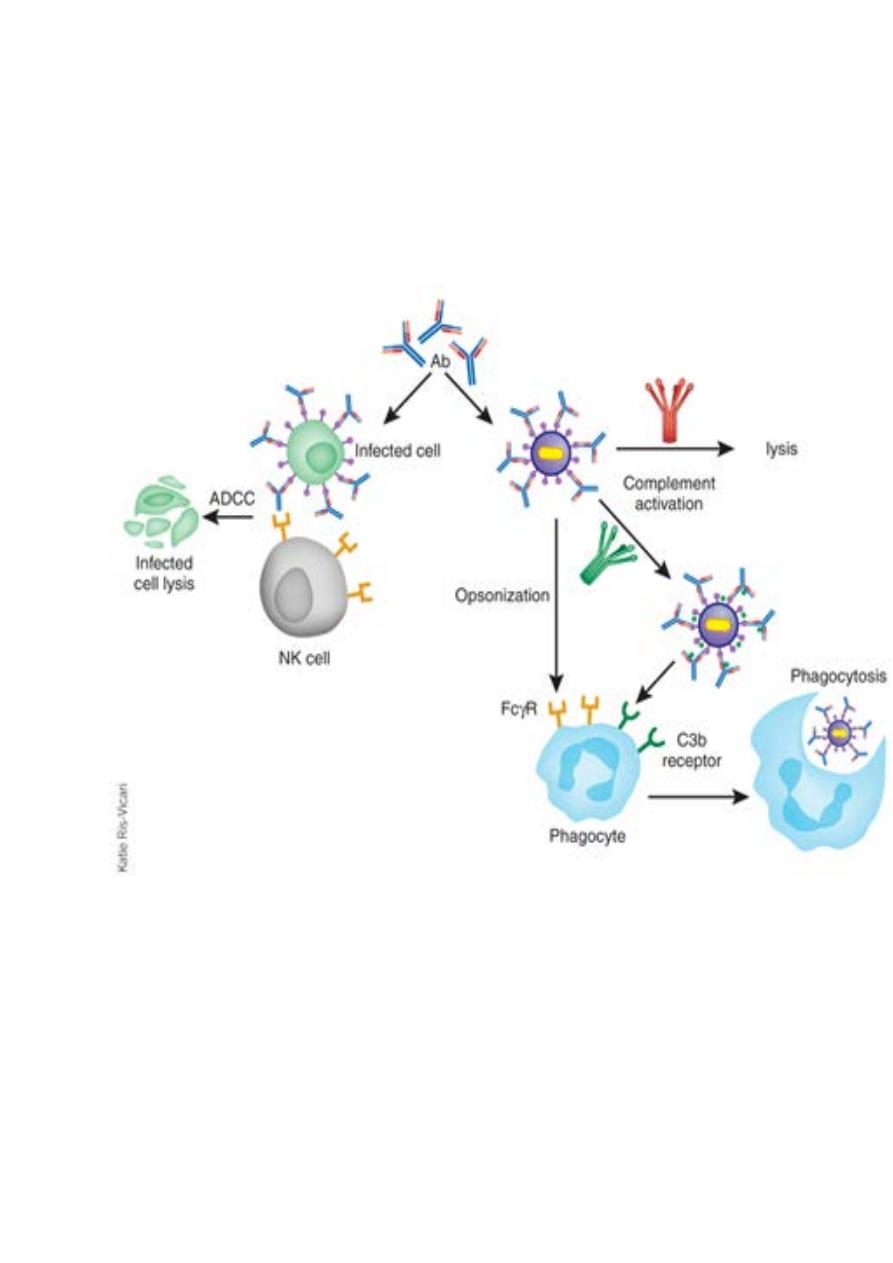
The consequences of Ab-binding to cell surface Ag are:
1- Complement is activated leading to lysis of target cell.
2- Opsonisation by:
- IgG Abs
-Complement fragments (C3b , C4b , iC3b)
3- Lysis of target cell by Ab-dependent cell-mediated cytolysis
(ADCC) through the action of natural killer (NK) cells.
2
3
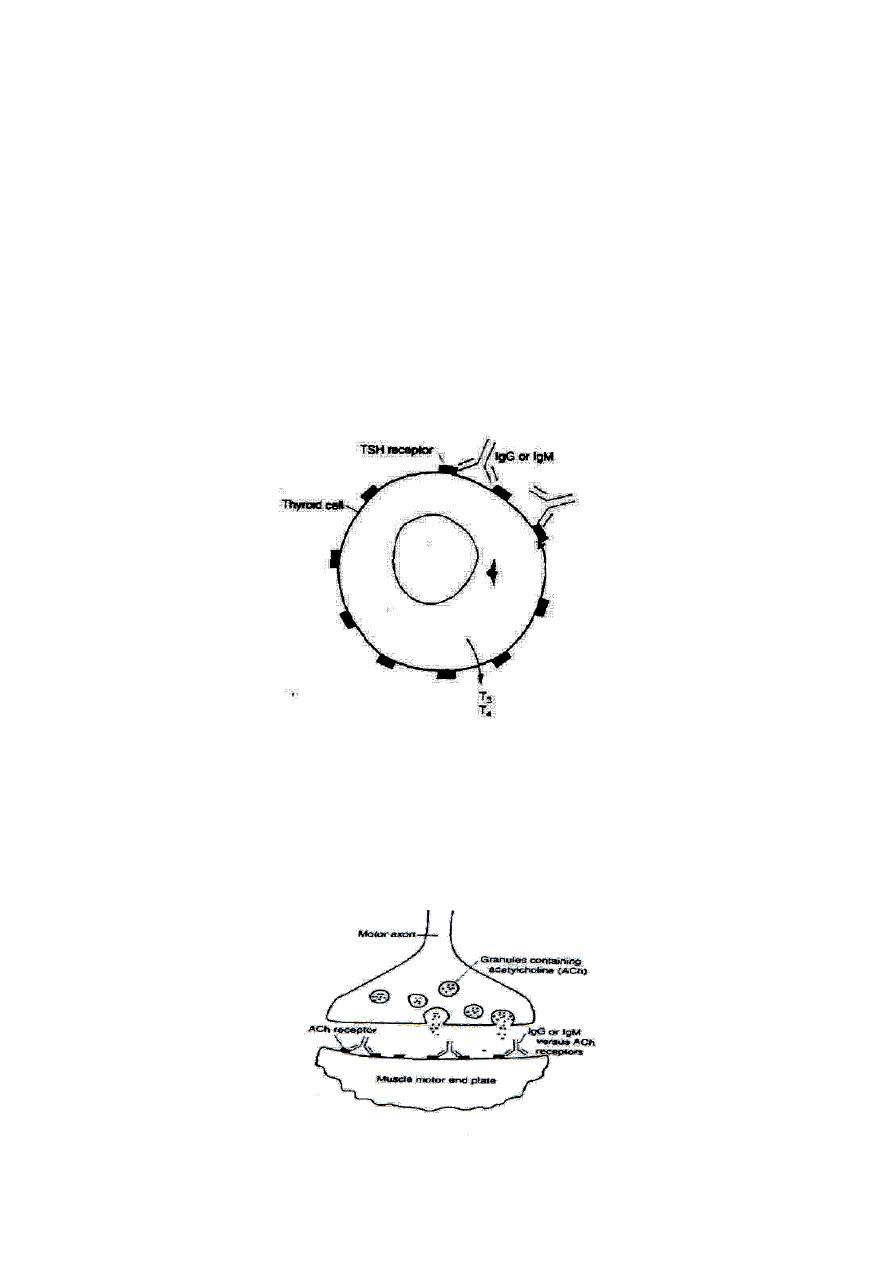
4- Functional alteration of the cell or tissue:
Sometimes the Abs binding target cell cause functional alteration of the
cell rather than destructing the cell as in Graves' disease & Myasthenia
gravis
- Graves' disease (Thyrotoxicosis, hyperthyroidism):
IgG or IgM Ab against TSH receptor on thyroid cells mimics the hormone
& causes the thyroid cell to secrete T
3
& T
4
. These auto-Abs (IgG, IgM)
are named as long acting thyroid-stimulating Abs (LATS).
- Myasthenia gravis:
IgG or IgM Abs (blocking Abs) reacts with ACh receptors & prevents
binding of ACh, thus inhibiting muscle contractions.

4
Clinical examples on type II H.S.:
1-
Miss-match blood transfusion:
This is associated with ABO system incompatibility & leads to rapid
intravascular haemolysis of RBCs.
2- Hemolytic disease of the newborn (HDN):
This disease is due to transport of IgG specific for Rhesus (Rh) protein
antigen (RhD) across the placenta,(about 85% of people are Rh+). If the
pregnant women is Rh- & the father is Rh+, there is a chance that the
fetus will be Rh+.
Erythrocytes from RhD
+
fetus leak into the maternal circulation, usually
during placental separation at time of birth. This stimulates a T-
dependent immune response, eventually resulting in the generation of
memory B-cells capable of producing IgG Ab against RhD. During
subsequent pregnancy with another Rh+ fetus, this maternal IgG can
transported across the placenta, react with fetal Rh+ RBCs,& activate
complement, producing hemolytic disease. This condition can be
prevented by treating the Rh- mother with RhoGAM (human anti-RhD
IgG Ab), at 28 weeks of gestation & again within 72 hours after birth.
This Ab eliminates the fetal Rh+ cells before they can generate RhD-
specific memory B-cells in the mother.
3-
Autoimmune diseases:
- Autoimmune hemolytic anemia
- Thrombocytopenic purpura
- Hashimoto's thyroiditis
- Good posture syndrome
- Myasthenia gravis
- Rheumatic fever
5
Type III H.S. (immune complex-mediated):
Immune complex-mediated reactions are initiated by Ag-Ab (IgG or IgM)
complexes that are formed in the blood vessels & then deposited in
tissues. This is followed by complement activation & cellular recruitment
including polymorph neutrophil. Inflammation is the main feature of this
reaction & the inflammatory response results in:
- Edema due to fluid accumulation.
- Erythema due to RBC accumulation.
- Indurations due to leukocyte infiltration.
Pathogenic mechanism of type III H.S.:
Pathogenesis involves an interplay of Ag , Ab , complement, &
neutrophils.
1- The first step is the intravascular formation of soluble immune
complexes.
a. Antigens: ex. auto-antigens, microbial antigens……etc
b. Antibodies: IgG &IgM ,both capable of activating complement.
2- Small immune complexes cause damage because they escape
phagocytosis, penetrate the endothelium of blood vessel walls & are deposited
on vascular basement membrane.
3-Complement is activated, & C3a & C5a are released. These are
anaphylatoxins that cause mast cell degranulation & the release of
vasoactiveamines. This increases permeability of vascular endothelium.
C5a is also chemotachtic for neutrophils which then infiltrate the area &
release lysosomal enzymes that destroy basement membrane. In
addition neurophils have receptors for C3b, move into the area in
response to C5a chemotaxin. In the process of attempting to engulf the
immune complexes, these phagocytic cells degranulate & release
proteolytic enzymes & other toxic molecules that injured tissues in area.
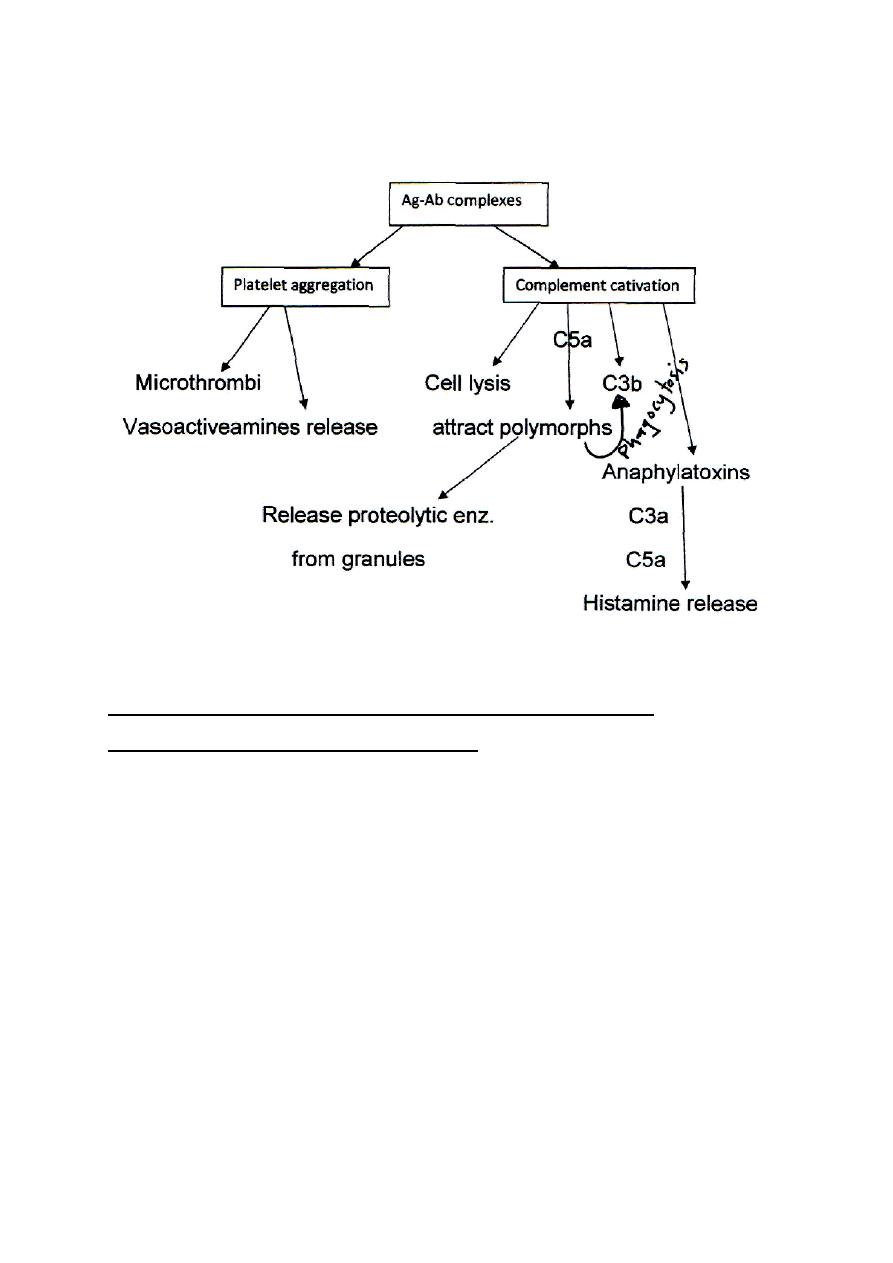
6
4-
Platelets also interact with immune complexes, this leads to
platelet aggregation & micro thrombus formation.
Immune complex mediated type III H.S. is of two types:
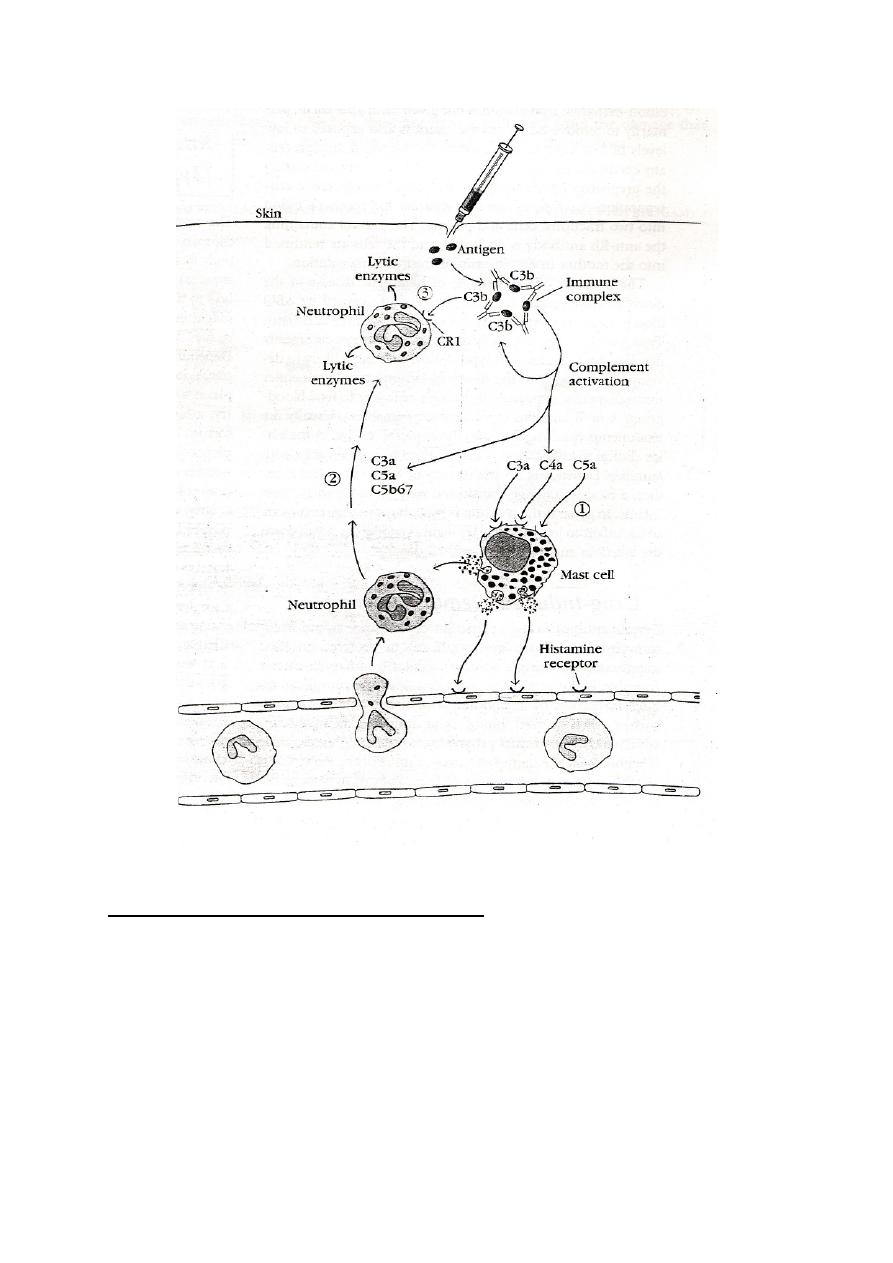
1- Local type III H.S. (arthus reaction)
- It occurs at the zone of Ab access. Immune complexes develop in
individuals who have pre-existing Ab to the Ag.
Arthus reaction: is a skin reaction followed injection of antigen
intradermally or subcutaneously into an animal that has high levels of
circulating Abs specific for that Ag leading to formation of immune
complexes. A red, local swelling develops at the site of injection within 4-
8 hours & disappears after 10-12 hours. Clearance is by opsonisation
through Fc, C3b & C4b receptors on neutrophils & macrophages.
7
Clinical example on local type III H.S.:
Extrinsic allergic alveolitis (Hypersensitivity pneumonitis): it is local
type III H.S. to inhalant Ags including:
- Farmer's lung due to inhalation of fungal spores present in dust of
mouldy hay.
- Pigeon fancier's disease due to inhaled serum protein in dust of
dried pigeon feces.
8
- Allergic bronchopulmonary aspergillosis due to inhalation of
spores of fungus aspergillum.
- Drug induced H.S. pneumonitis
→ drugs, industrial materials e.g.
nitrofurantoin, cromolyn... etc.
Clinical features:
- Cough, dyspnoea, fever, chills
- 4-8 hours after exposure
- Disappear 18-24 hours
2- Systemic (generalized) type III H.S:
- It occurs at the zone of Ag excess
- It follows injection of large doses of foreign Ag (serum, drug).
When large amount of Ag enter the blood stream & bind to Ab ,
circulating immune complexes can form. These Ag-Ab complexes are
small size molecules diffuse through the blood & deposited at various
sites, activating complements, & causing tissue damage. These immune
complexes can accumulate on :
- Basement membrane of capillaries & large blood vessels causing
vasculitis & arteritis.
- Glomerular basement membrane causing glomerular nephritis
- Synovial membrane causing arthritis
Clinical examples on systemic type III:
1- Serum sickness:
It is a complication of serum therapy following injection of massive doses
of foreign protein in human like injection of horse anti-diphtheria serum
or horse anti-tetanus serum.

9
Typically, within days or weeks after exposure to foreign serum Ags , an
individual manifest a combination of symptoms called serum sickness.
These include fever, rashes, edema, erythema, lymphadenopathy,
arthritis, & glomerulonephritis.
2- Post-streptococcal glomerular nephritis:
Following streptococcal pharyngitis, immune complexes are deposited in
glomerular basement membrane leading to protein urea & hemturia.
3- Systemic lupus erythematosus
4- Rheumatoid arthritis