Introduction of pharmaceutical care and clinical pharmacy
New professional and responsibilityDr. Sabah g. Al-dabbagh
• The physician has traditionally been responsible for a patient's drug therapy.• However, due to;
• * The evolution of health care systems.
• * The diverse nature of consumer lifestyle.
• Both make it extremely difficult or impossible for any single physician to undertake this increasingly complex duty.
• So, the physician requires help to manage all of the increased complexities of drug use.
• The pharmacist is the logical choice, who has a good and intensive knowledge concerning drug and drug therapy through his or her 6 years of higher education in different drug-related areas.
• The new professional practice is not intended to replace the role of the physician or any other practitioner but rather to meet a need in the health care system that has arisen.
Increased in complexities of drug use is mainly due to:
• * Multiple prescriber of medications for a single patient.
• * The explosion of drug products.
• * Drug information presently on the market.
• * The increased complexity of drug therapy.
• * The significant level of drug-related morbidity and mortality
• associated with drug use.
• * The high human and financial cost of drug misadventuring
• (ADRs , drugs interaction and side effects or any unwanted
• pharmacological action).
Aims of Pharmaceutical Care
Effective drug therapy
Safe drug therapy
Economic drug therapy
Improve quality of life
Will the patient take the therapy?
What does the patient view as an improved quality of life?• Pharmaceutical care is a generalist practice, where the practitioner takes responsibility to:
1. identify patient's drug - related needs.
• 2. resolve patient's drug - related needs.
3. prevent patient's drug - related needs
• Primary health care: include all a patients' health care needs,
• Pharmaceutical care: involves only the patient’s drug-related needs i.e. all of the patients drug-related needs.
• 1975 Micheal et al; defined the pharmaceutical care as:
• The care that a given patient requires and receives which assures safe and rational drug usage.• 1980 Brodie et al; concluded, that pharmaceutical care include the determination of the drug needs for a given individual ( before, during, after treatment) to ensure optimally safe and effective therapy.
• 1988 Hepler; described pharmaceutical care as a conventional relationship between a patient and pharmacist in which the pharmacist performs drug use control functions.
1990 Hepler and strand: conclude Pharmaceutical care as:
The direct interaction of the pharmacist with the patient for the
purpose of caring for the patients drug-related needs
• 1992 strand et al : initiated a 3 year project,
• known as Minesota pharmaceutical care project, serves as
• the foundation for significant portion of which has become
• the practice of pharmaceutical care.
Strand et al describe two sets of responsibilities dealing with a patient's drug therapy for this new professional:
1.
* All of a patient's drug therapy was appropriates
* The most effective possible.
* The safest available.
2.
* Identify drug therapy problems.* Resolve drug therapy problems.
* Prevent any drug therapy problems.
• * The level of drug-related morbidity and mortality is significant,
• * Drug development has increasingly produced numerous therapeutic agents often at a rate frequently referred to as “explosive “not all of these have been new drug classes but rather new brands in old classes.• Also the vast number of "copycat" or "me-too" drugs produced by companies.
• * When the particular morbidity patterns are identified and potential markets defined, competition between pharmaceutical companies become intense, to produce "The drug of choice" in the treatment of a particular type of disease.

Additional causes for the development of
clinical pharmacy and pharmaceutical care
• * Discussions of quality surrounding drug use usually do not refer to the quality of the drug product, but to the quality of decisions as whether and how a drug should be used, i.e. drug therapy decisions.
• Up to 20% of hospitalization in U.S.A. are related to drug therapy problems, and
• 50% of the drug -related morbidity and mortality is preventable.
• * The cost of drug-related morbidity and mortality in USA of 76 billions dollar.
• Cont.-----
• The pharmaceutical industry has traditionally influenced physicians and the drug product they prescribe through direct advertising and promotion.• Recently this industry has reached the patient through direct advertising of drug products to the customer.
• But Patients seldom have a single disease, and treating the disease instead of the patient is associated with much limitation.
• Therefore, it is necessary to find drug of choice for the individual patient rather than drug of choice for the disease
• Hospitals as well as managed care organization have attempted to manage the use of drug therapy, through:
• * Pharmacy and therapeutics committees ( P& T committees).
• * Formulary system.
• * More recently, protocol for drug therapy; Protocol development is based on the "Best practice" standards available in the literature.
• But this protocol makes it difficult to manage patient-specific variation.
Several activities have been developed as a part of the clinical pharmacy movement, which influenced drug use in hospitals through the development of specialty clinics.
* Warfarin dosing.
* Diabetes education.
* Pharmacokinetic dosing services.
* Total Parenteral nutrition
ADVERSE DRUG EVENT (ADE)
Definition:Any injury that results from the use of a drug
CLASSIFICATIONS OF ADE
1. Adverse Drug Reaction (ADR) :Any response to a drug that is noxious and unintended and that occurs at doses normally used in humans for prophylaxis, diagnosis, or therapy of disease
2. Medication Error:
Any preventable drug event that may cause or lead to inappropriate medication use or patient harm3. Accidental/Intentional Overdose:
Accidental (childhood poisoning) or intentional (suicide attempt)Some epidemiological studies show the prevalence of ADE:
a. 18% of patients experience an ADE
b. 1/3 of drug related hospitalizations involve patient noncompliance issues
c. 10-30% of hospitalized patients experience an ADE, 1-3% significant
d. Each ADE costs approximately $5000
e. 30-50% of ADEs in hospitalized patients are preventable
f. in log term therapy more than 50% of ADEs are preventable
g. Polypharmacy: average number of medications taken by elderly 5-8 per day
h. The ADE rate among patients receiving
1-3 drugs: 6%
More than 6 drugs the rate is 52%
ADEs STATISTICS
Warfarin 95%Antidiabetic agents 94%
NSAIDs 89%
Digoxin 82%
Antiepileptic drugs 69%
Inadequate monitoring of drug therapy 67%
Inappropriate dose 51%
Patient compliance 33%
Drug-drug interaction 26%
Contraindication 3%
Allergy 1%
CONCLUSION
THE ANNUAL COST OF DRUG- RELATED MORBIDITY AND MORTALITY EXCEEDS : $ 136 BILLION
• Drug therapy problems
• All DTPs can be classified into seven main categories.• Drug therapy problems are the ‘heart’ & ‘soul’ of the practice of pharmaceutical care.
• Drug therapy problems have been divided into seven major categories.
• Each pharmacist need to become familiar with these categories and their common caused.
• The seven categories of DIPs are:
1. The patient has a medical condition that requires the initiation of new or additional drug therapy.
2. The patient is taking drug therapy that is unnecessary given his a her
present condition.
3. The patient has a medical condition for which the wrong drug is
given.
4. The patient has a medical condition for which too little of the
correct drug is being taken.
5. The patient has a medical condition resulting from an ADRs.
6. The patient has a medical condition for which too much of the correct drug
is being taken.
7. The patient has a medical condition resulting from not taking the drug
appropriately.
Clinical pharmacy
The overall goal of clinical pharmacy activities is to promote the correct and appropriate use of medicinal products and devices.
These activities aim at:
1. Maximizing the clinical effect of medicines,i.e., using the most effective treatment for each type of patient
2. Minimizing the risk of treatment-induced adverse events,
i.e., monitoring the therapy course and the patient's compliance.3. Minimizing the expenditures for pharmacological treatments born by the national health systems and by the patients,
i.e., trying to provide the best treatment alternative for the greatest number of patients.
One of the most important factor which may lead to drug therapy problems and related subjects is the inter-individual variation in drug response.
This subject has been studied under new sciences named as pharmacogenetics and pharmacogenomics( both are important issues in clinical pharmacy activities)
Inter-individual Variability in Drug Response
Disease Drug Class Rate of Poor ResponseAsthma Beta-agonists 40-75%
Hypertension Various 30%
Solid Cancers Various 70%
Depression SSRIs, tricyclics 20-40%
Diabetes Sulfonylureas, others 50%
Arthritis NSAIDs, COX-2 inhibitors 30-60%
Schizophrenia Various 25-75%
Genetics or Genomics?
PharmacogeneticsStudy of how genetic differences in a SINGLE gene influence variability in drug response (i.e., efficacy and toxicity)
Pharmacogenomics
Study of how genetic (genome) differences in MULTIPLE genes influence variability in drug response (i.e., efficacy and toxicity)
Factors Contributing to Interindividual Variability in Drug Disposition and Action
AgeRace/ethnicity
Weight
Gender
Concomitant Diseases
Concomitant Drugs
Social factors
GENETICS
PERSONALIZED
MEDICINEPotential of Pharmacogenomics
All patients with same diagnosis
1
2
Responders and patients
not predisposed to toxicityNon-responders
and toxic
responders
Treat with alternative
drug or dose
Treat with
conventional
drug or dose
Genetic variability is the main factor but not the only factor determine such inter-individual variation in drug therapy.
Whatever the receptors of drug is, it is usually protein in nature and it is gene product.
Therefore any variation in the sequence, absence or abnormal present of amino acids may lead to non-typical receptors or enzymes and finally may cause unusual or unexpected action with corresponding drug.
DNA is Information
DNAA, T, G, C
CodonGene
ChromosomeGenome
ENGLISHAbcdefg….xyz
WordSentence
Chapter
Book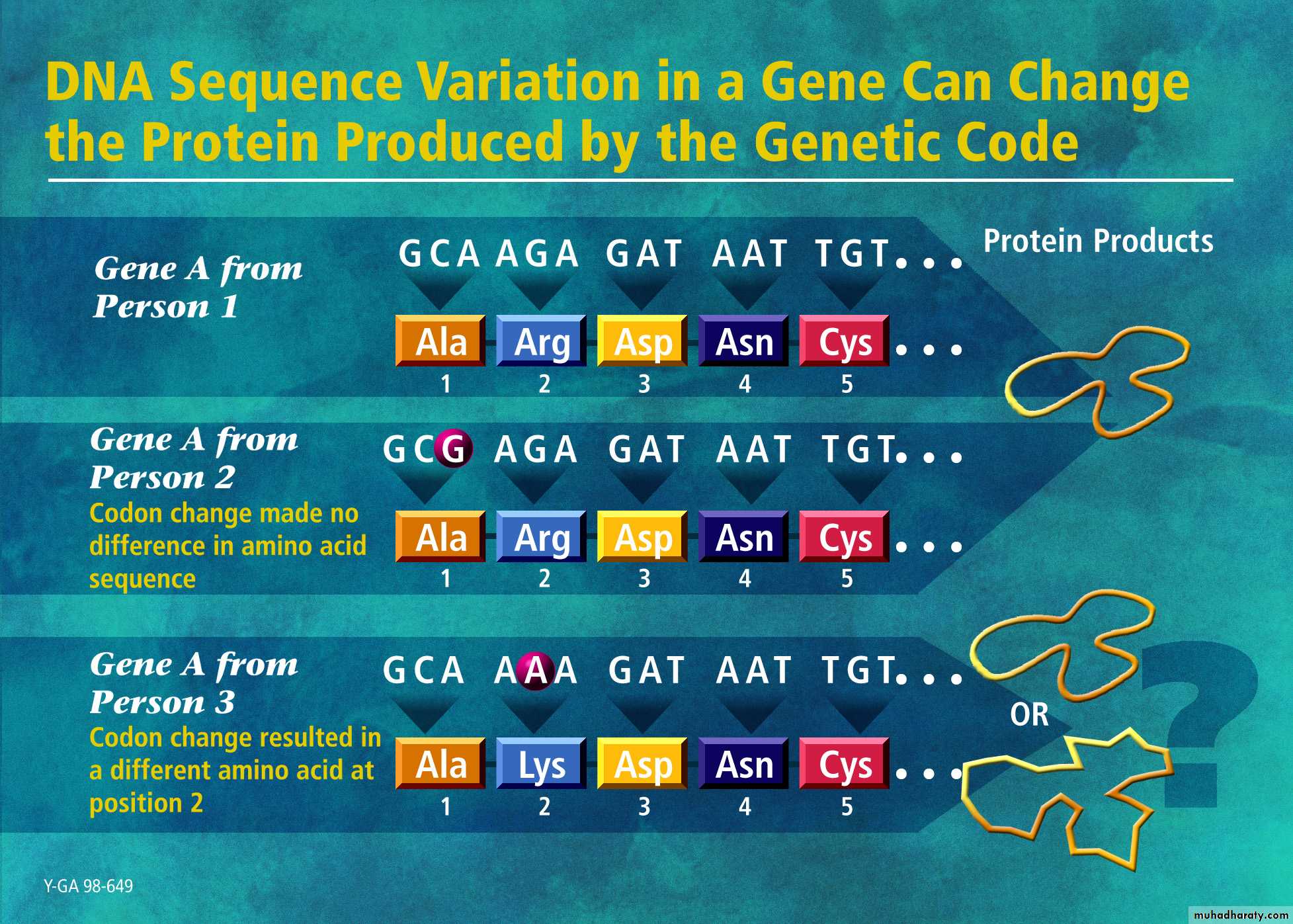
Pharmacogenomics
DRUGTARGETS
DRUG
METABOLIZING
ENZYMES
DRUG
TRANSPORTERS
PHARMACOKINETICS
PHARMACODYNAMICS
Variability in
Efficacy/Toxicity
Johnson JA. Trends in Genetics 2003: 660-666

"Here's my
sequence..."The New Yorker