MALIGNANT MELANOMA
OutlineIntroduction
Aetiology
Types
Invasion and Metastasis
Risk Factors
Diagnosis and Staging
Treatment and Prevention
Skin:Epidermis – Melanocytes
Melanocytes:
In stratum basale
Pale “halo” of cytoplasm
Neural crest
Produce melanin and pass it on to nearby keratinocytes
Melanin covers nuclei of nearby keratinocytes
Skin colour depends on melanocytes activity, rather than the number present
MALIGNANT MELANOMA
A tumour arising from melanocytes of the basal layer of the epidermis
Less commonly – uveal tract (eye) and meningeal membranes
AETIOLOGY
The cause is unknown.
Excessive exposure to sunlight
Genetic predisposition
RISK FACTORS FOR MELANOMA
Large numbers of benign naevi
Clinically atypical naevi
Severe sunburn
Early years in a tropical climate
Family history of MM
Clinical features
Occur anywhere on the skin
Females (commonest is lower leg)
Males ( back).
Early melanoma is pain free. The only symptom if present is mild irritation or itch.
AIDS IN CLINICAL DIAGNOSIS
GLASGOW SYSTEM
Major:
Change in size
Irregular pigment
Irregular outline
Minor:
Diameter >6mm
Inflammation
Oozing/bleeding
Itch/altered sensation
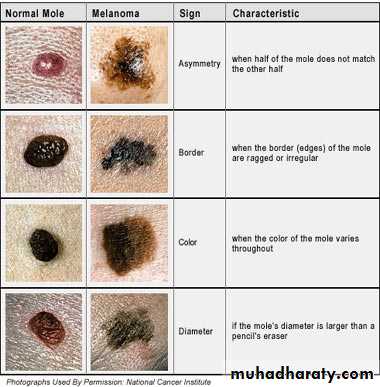
AMERICAN ‘ABCDE’
SYSTEM
Asymmetry
Border
Colour
Diameter
Evolution
TYPES OF MELANOMA
Superficial spreading Malignant melanomaNodular melanoma
Letingo maligna melanoma
Acral melanoma
SUPERFICIAL SPREADING
The most common type of MM in the white-skinned population – 70% of cases
Commonest sites – lower leg in females and back in males
In early stages may be small, then growth becomes irregular
NODULAR
Commoner in males
Trunk is a common site
Rapidly growing
Usually thick with a poor prognosis
Black/brown nodule
Ulceration and bleeding are common
ACRAL LENTIGINOUS MELANOMA
In white-skinned population this accounts for 10% of MMs, but is the commonest MM in nonwhite-skinned nations
Found on palms and soles
Usually comprises a flat lentiginous area with an invasive nodular component
SUBUNGAL MELANOMA
Rare
Often diagnosed late – confusion with benign subungal naevus, paronychial infections, trauma
Hutchinson’s sign – spillage of pigment onto the surrounding nailfold
LENTIGO MALIGNA MELANOMA
Occurs as a late development in a lentigo maligna
Mainly on the face in elderly patients
May be many years before an invasive nodule develops
DDx
Superficial spreading melanomas
Benign melanocytic naevi.
Nodular melanomas
Vascular tumor
Histiocytoma
Latingo maligna melanoma
Seborrhic keratoses
PROGNOSTIC VARIABLES
The Breslow thickness is the single most important prognostic variable (distance in mm of the furthest tumour cell from the basal layer of the epidermis)
Scalp lesions worse prognosis, then palms and soles, then trunk, then extremeties
Younger women appear to do better than either men at any stage or women over 50
Ulceration of the tumour surface is a high risk factor
MANAGEMENT
Surgical resection of tumour
MOHS technique
Lymph node dissection
Chemotherapy
Radiotherapy
Immunotherapy
Prevention
Reduce risk factor exposure:
Covering up (sunscreen, sunglasses, clothes)
Avoidance (less time in sun)
Screening (possibly feasible)