Nutritional Aspects of Dental Caries:
Causes, Prevention, and Treatment
Dr. Hakan Ç olak
DDS, PhD

Learning Outcomes
• Explain the role each of the following play in the
caries process: tooth, saliva, food, and plaque biofilm.
• Identify foods that stimulate salivary flow
• Suggest food and beverage choices and their timing
to reduce the cariogenicity of a patient’
s diet
• Describe characteristics of foods having
noncariogenic or cariostatic properties

Introduction
• Diet and nutrients play a role in dental caries. Some
foods exert a cariogenic effect, whereas others are
cariostatic or anticariogenic and offer protection to
reduce caries.
Nutrient
s
Topical effect
Primary
Secondary
Systemic
effect
Primary
Secondary

• The primary oral health goals of Healthy People 2020 are to
- reduce the number of caries in children and adolescents by 10%,
- reduce untreated decay in this population group and adults by
10%.
• Thirty-three percent of preschool-age children and more
than 50% of children and adolescents have experienced
decay.
• Regarding untreated decay, 24% of preschool-age children,
29% of children, 17% of adolescents, and 28% of adults up
to age 44 years have at least one untreated area

Major Factors in the Dental
Caries Process
Major actors that interact in the dental caries
process
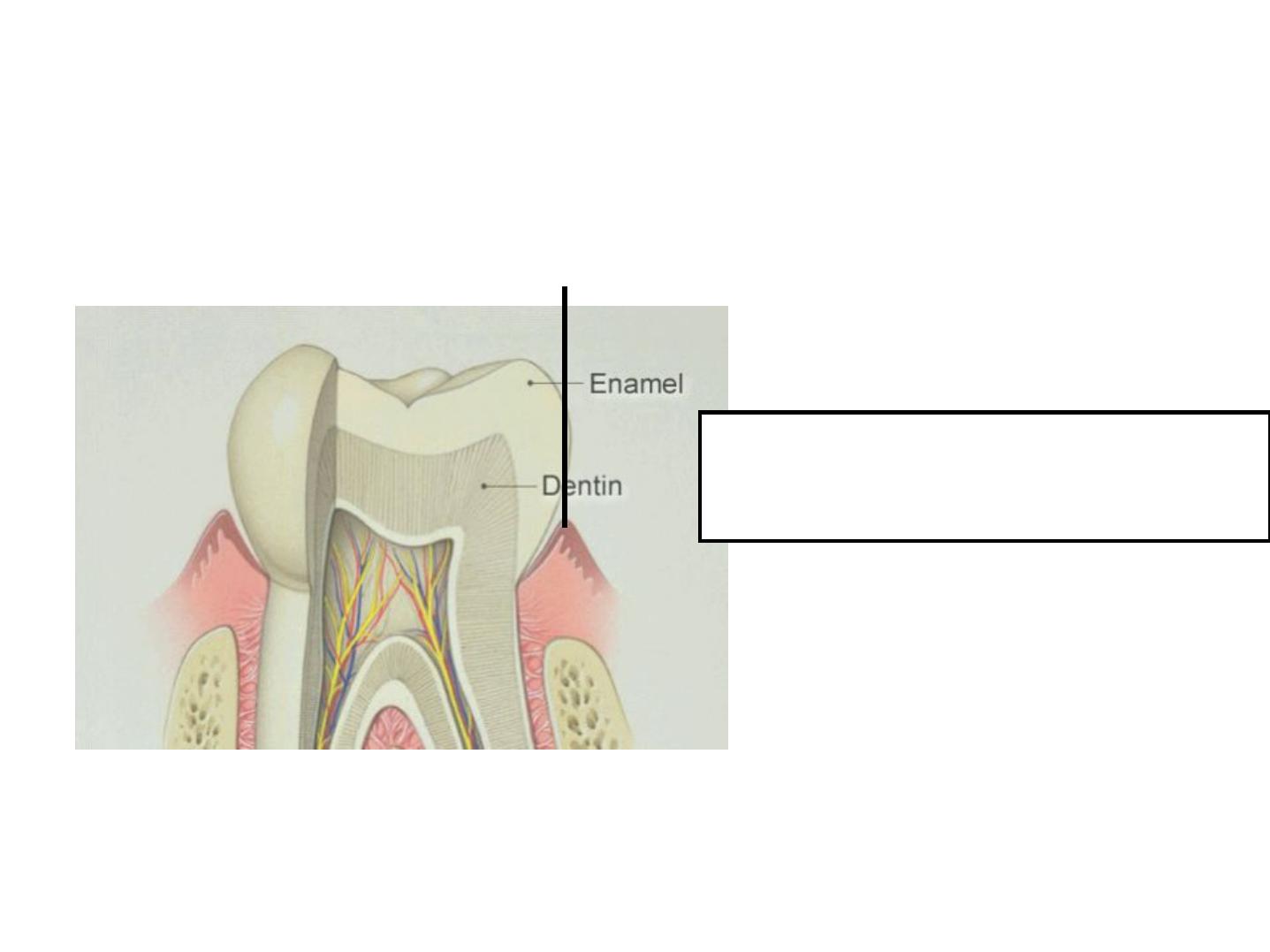
Tooth Structure
• Increasing resistance of the tooth against
demineralization begins in the preeruptive phase.
• It is essential to maintain an
adequate intake of
nutrients
during growth and development of enamel
and dentin.

Tooth Structure
• The most influential nutrients include
- calcium;
- phosphorus;
- vitamins A, C, and D;
- fluoride;
- protein.
• Indirectly, some fermentable carbohydrates play a
role in the formation of caries before tooth eruption.

• Consider a child who snacks on cookies, candy, or ice
cream throughout the day and is not hungry or meat,
vegetables, fruit, and milk offered at mealtime.
• A child’
s diet high
in low-nutrient
(or calorie-dense)
carbohydrates may be deficient in required nutrients
for optimal growth and development of the dentition.

Deep pits and
fissures increase
susceptibility of dental
caries
•Overlapping
and crowding
of teeth
The potential of plaque
bioflm and food
entrapment
Increase susceptibility
of dental caries


Host Factors
• Food selection
• Dietary patterns
• Oral hygiene habits
• Genetics
• Race or ethnicity
• Age
• Income
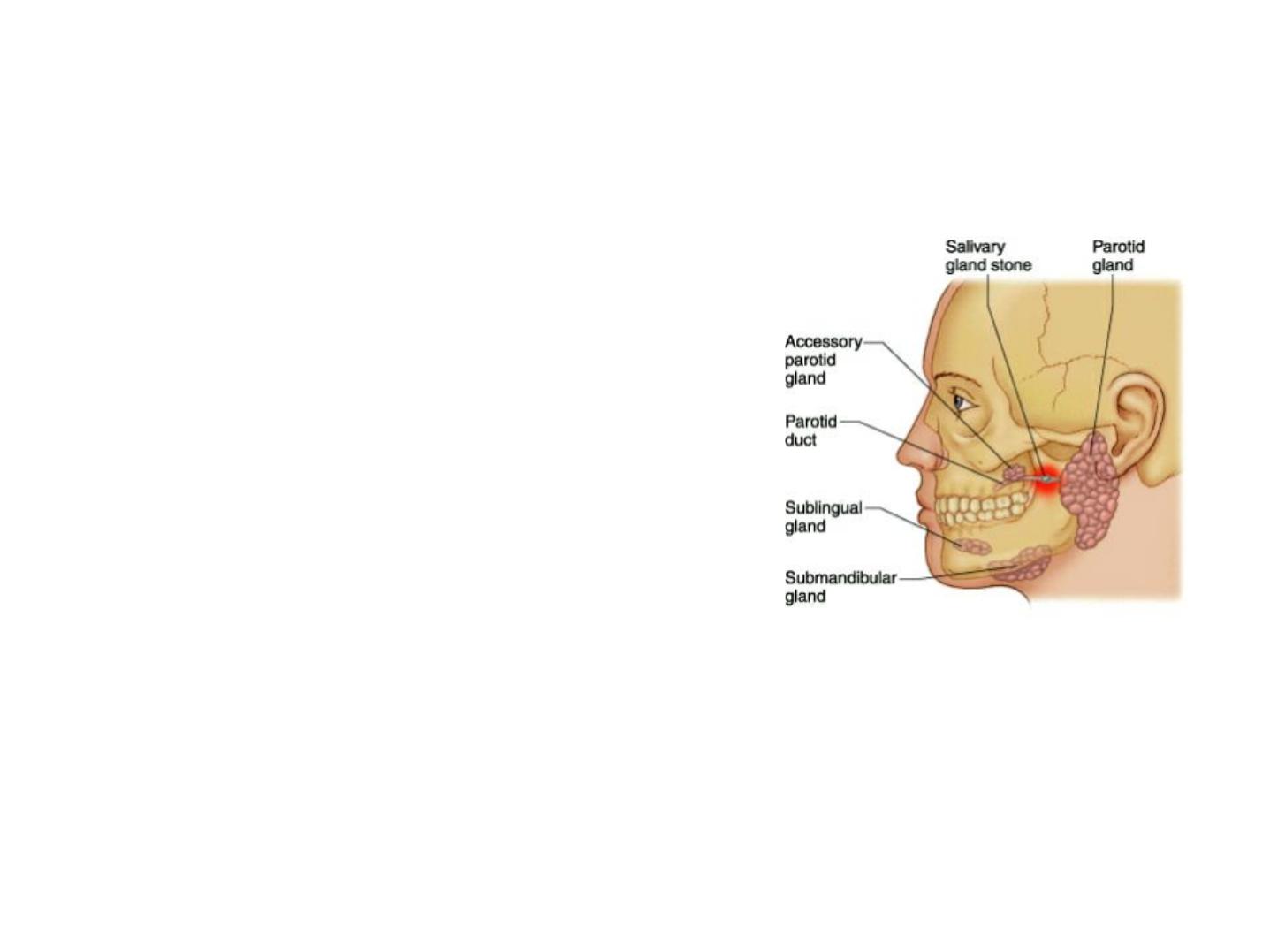
Saliva
• Availability of essential nutrients
during the development of
salivary glands, which begins
during
the fourth week in utero
,
has a significant impact on the
amount of saliva and its
composition.

Saliva
• Saliva provides protection against caries
- Saliva acts as a buffer by neutralizing much of the acid
produced by plaque biofilm as a result of carbohydrate
metabolism

Saliva
• Saliva provides protection against caries
- Normal saliva contains bicarbonate, phosphate, and
protein, which dilute and neutralize acids to maintain a
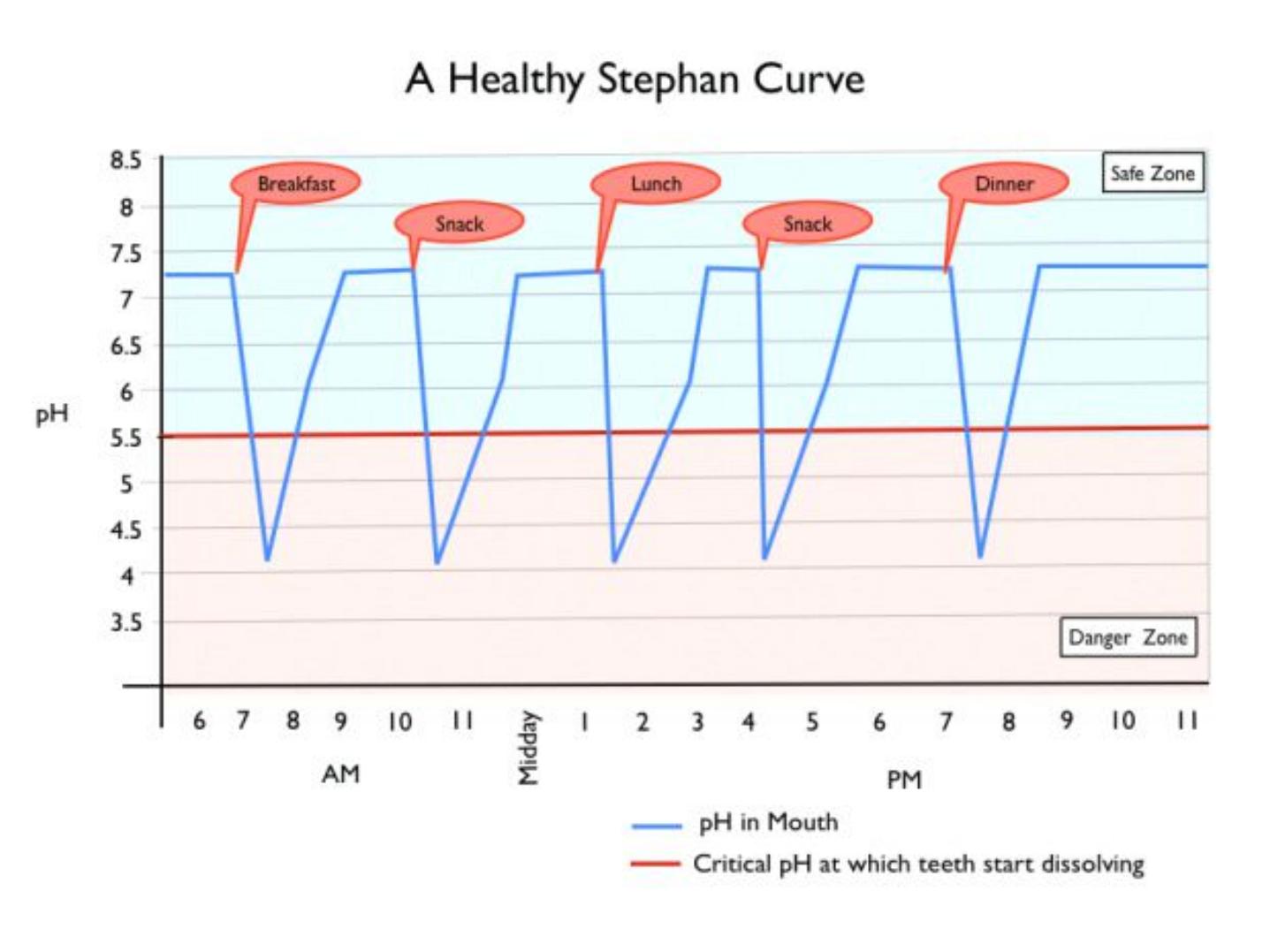
neutral oral pH, which is around 7.
• After an acidic drink is consumed, the pH of the oral cavity is
rapidly normalized by the components of saliva.
• Because saliva is saturated with calcium, phosphate, and fluoride
ions, the potential for remineralization (restoration of damaged
enamel) and resistance to enamel dissolution exists.

Saliva
• An adequate salivary flow
- enables rapid transport of foods from the mouth
• decreasing the length of time harmful bacteria and food particles
are able to attach to teeth and cause caries to develop
• Antimicrobial elements in saliva
- immunoglobulin A
• either interfere with adherence of bacteria or compete with
bacteria to attach to the tooth surface.
- An alkaline saliva offers protection, whereas an acidic
saliva increases susceptibility to caries.

Plaque Biofilm and Its Bacterial
Components
B
ac
t
e
ri
a
Polysaccharide
s
Pro
te
in
s
Lip
id
s
Plaque
Plaque Biofilm and Its Bacterial
Components
Plaque biofilm forms a local barrier on
enamel and may interfere with
demineralization

by-product of the metabolism of
sucrose and glucose
bacteria produce acids that lower
the pH
a more favorable environment for development of
certain bacteria, such as Streptococcus mutans. S.
mutans, a gram-positive, anaerobic, spherical
bacterium
Composition of plaque biofilm is
altered
Carbonhydrates
Ingestion metabolism
by salivary amylase begins within 2 to
3 minutes and can
persist for hours
acetic, butyric,
ormic, lactic, and propionic acids
its metabolism bysalivary amylase begins within 2 to 3 minutes and can
persist or hours
acetic, butyric, formic, lactic, and propionic acids
Concentration of the
acids escalates as carbohydrate intake continues, whereas the pH o fthe
plaque decreases
Demineralization of enamel occurs when the “
critical pH”of 5.5 is reached
metabolic product
In
g
e
st
io
n
st
a
rs
ts
Carbonhydrates

Demineralization is faster on root surfaces than
on enamel because dentin contains less mineral
content
In interproximal areas for in deep pits and fissures,
the pH can decrease to 4 and remain at that pH or
an hour
The pH of acids produced by bacteria in plaque
biofilm is eventually neutralized after elimination
of cariogenic foods as saliva exerts its protective
action
Keynotes

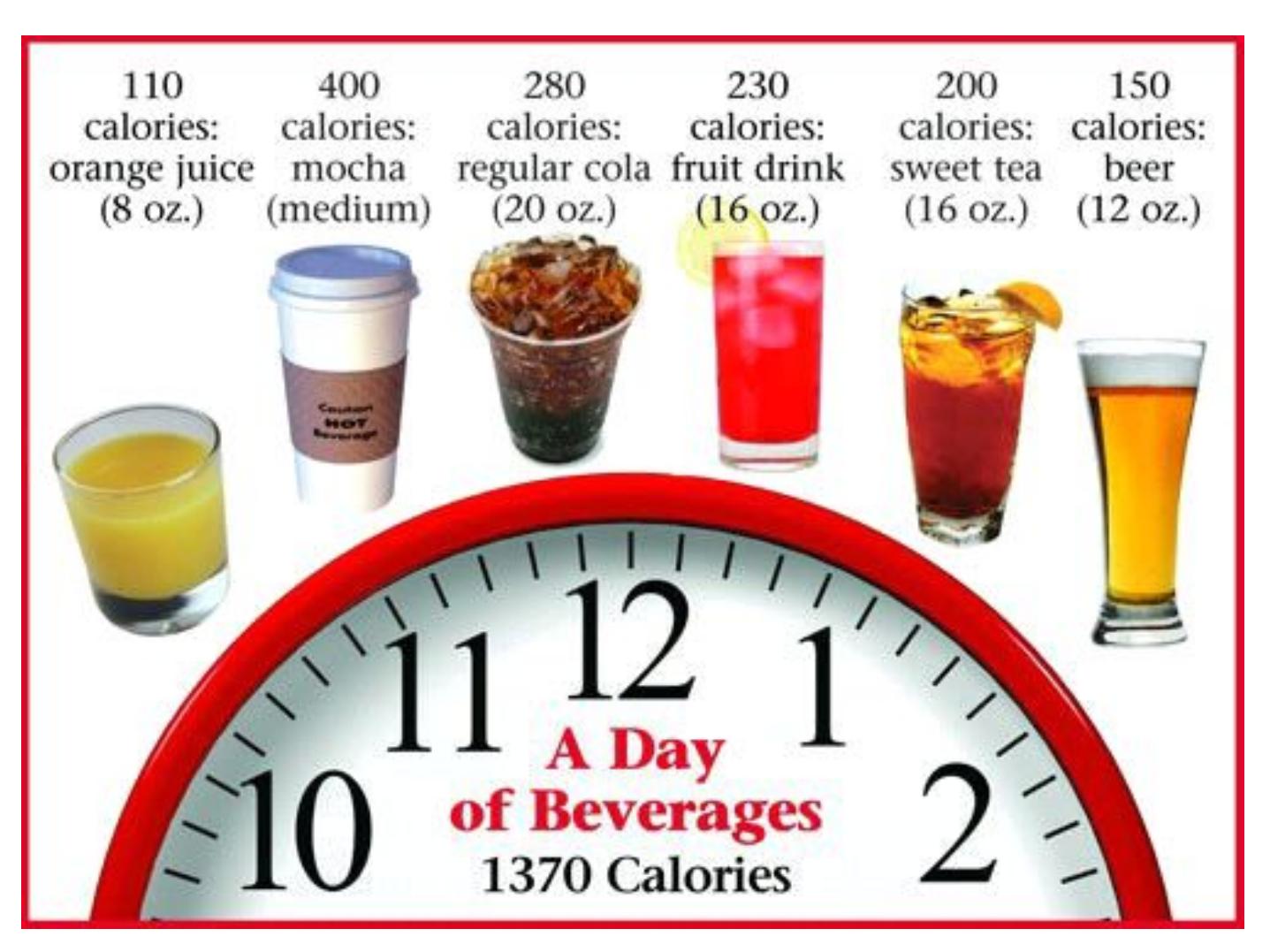
Cariogenic Foods
• The average daily consumption from added sugars
among 2- to 18-year olds is 365 kcals (over 90 g, or
approximately 23 tsp*)
• The major sources of added sugars, in descending
order, are
- sugar-sweetened beverages (e.g., sodas or ruit drinks),
- grain desserts (e.g., cookies or cakes),
- dairy desserts (e.g., ice cream),
- candy, and cold cereals
*Tea spoon, 1 tsp=16 kcals


Cariogenic Foods
• Nondiet sports and energy drinks
- fast growing sugar-sweetened
beverage choices.
- Almost 1 in 4 U.S. adults consumes
sports and energy drinks at least one
time per week.
- A 20-oz
* bottle of a
regular sports
drink contains
32 g
of added sugars, a
12-oz
can of
energy drink
contains
37
g
, and
12 oz sugar-sweetened soda
may contain as much as
40 g sugar
*1 0z = 29,5735296875 ml

*1 0z = 29,5735296875 ml
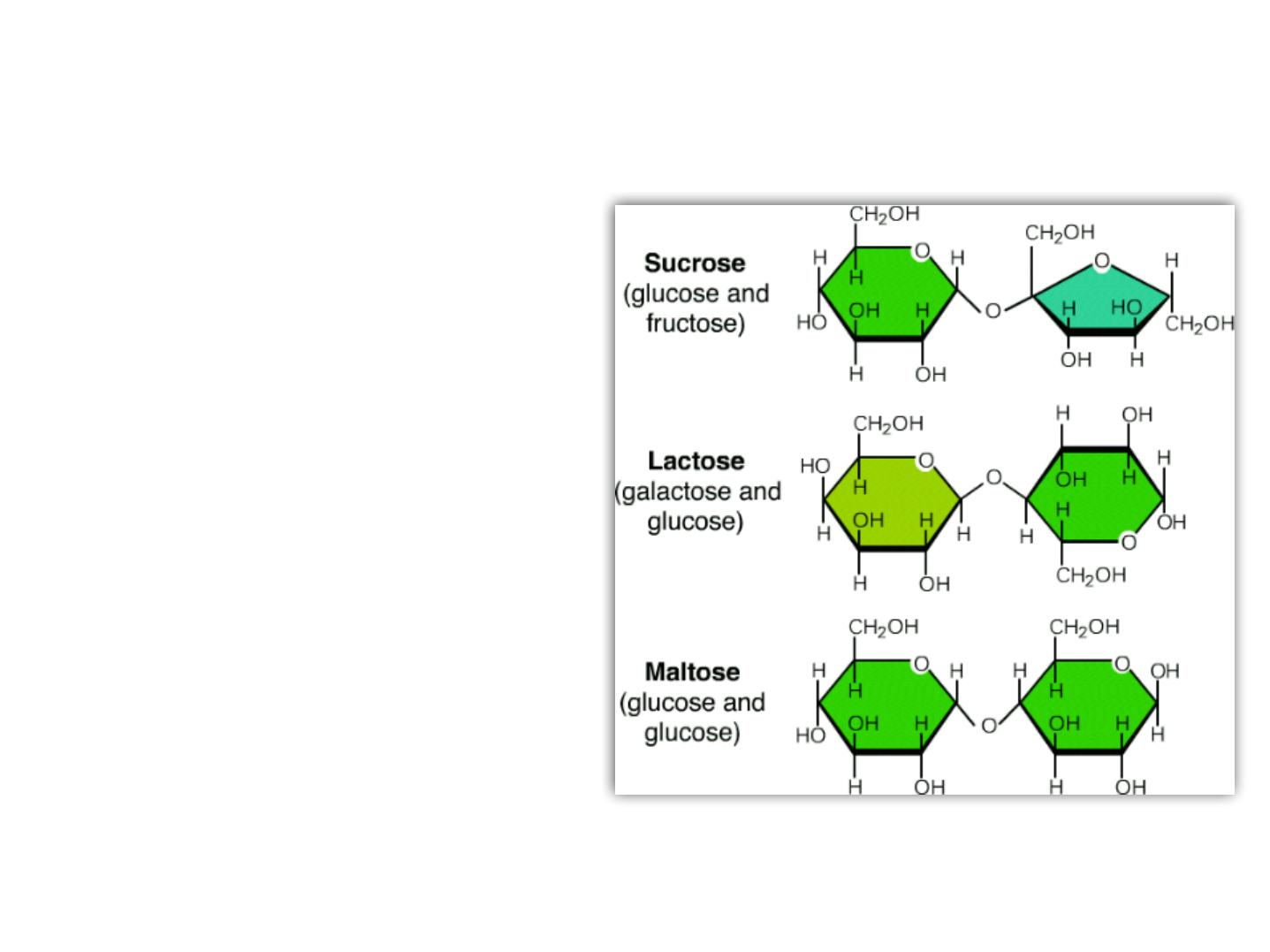
Cariogenic Foods
• Monosaccharides and
Disaccharides
- Sucrose, fructose,
glucose, and maltose
- Small sized sugar
molecules
- Allows salivary amylase
to split the molecules
into components that
can be easily
metabolized by plaque
bacteria.
Cariogenic Foods
• Sucrose
- used to produce glucans
- facilitating the adherence of bacteria,
such as S. mutans, to the dental
pellicle.
• Glucose and other carbohydrates
- used to produce extracellular
polysaccharides.
Diets containing sucrose,
glucose, and other
disaccharides can increase
plaque biofilm mass and
facilitate its retention and
colonization
Polysaccaharides
(Starches)
less damaging to enamel
make it almost insoluble
the time a starch is in the mouth is usually not
long enough or it to be completely
metabolized if oral self-care is promptly
completed
Several unique properties prevent starch from providing a readily available
energy source for cariogenic microflora, and it is less likely to produce caries
than mono- or disaccharides

Cariogenic Foods
• Fresh fruit
- low cariogenicity
• its low percentage of carbohydrate and high percentage of water
- Firm fruits such as apples
• play a protective role by stimulating saliva flow
- The high concentration of fructose found in juices
• potentially a source of substrate or plaque bacteria that may
influence caries risk
- Dried fruit (e.g., raisins)
• Sticky nature
• increases risk o decay.
Foods That Can Cause the pH of Human Interproximal Plaque to
Fall Below 5.5
Alcohol
•Bananas
•Beans, baked
•Bread
•Candy
•Cereals, non–presweetened,
ready-to-eat
•Cereals, presweetened, ready-
to-eat
•Chips
•Cookies
•Crackers
•Doughnuts, plain
•Energy drinks
•Flavored cofees and teas
•Fruit, dried
•Fruit drinks
•Fruit smoothies
•Honey
•Ice cream
•Jams and jellies
•Marshmallows
•Oatmeal, instant cooked
•Pasta
•Peanut butter
•Pretzels
•Rice, cooked
•Snack cakes
•So t drinks
•Sports drinks
Anticariogenic Properties of Food
• Some food components can protect teeth by
decreasing demineralization, enhancing
remineralization, or increasing salivary flow, even in
the presence o a fermentable carbohydrate

Anticariogenic Properties of Food
• Sugar Alcohols
- mannitol and sorbitol
• substitute sweeteners
• viable alternatives to sugar because of their sweet taste but have
the added benefit of being noncariogenic
• fermented more slowly in the mouth than monosaccharides and
disaccharides; buffering effects of saliva competently neutralize
destructive acids produced by plaque bacteria.

Anticariogenic Properties of Food
• Sugar Alcohols
- xylitol
• found naturally in plants
• equal to or sweeter than sucrose.
• classifed as anticariogenic
• oral flora do not contain enzymes to ferment it, and metabolizing
microorganisms, such as S. mutans, are inhibited
• Chewing gums, mints, and candies containing xylitol
• inhibit enamel demineralization.
• inhibitory effect is enhanced by
- increased salivary flow,
- increased oral clearance
- greater buffering capabilities.

Anticariogenic Properties of Food
• Nonnutritive Sweeteners
- Aspartame, saccharin, sucralose, neotame, and
acesulfame
- are not metabolized by microorganisms
- do not promote dental caries.
- Foods made from these sweeteners are generally higher in
cost
• not be feasible or low-income patients.
Products containing aspartame
ü The following are well-known products that use aspartame
:
ü Diet sodas
ü Yogurts
ü Chewing gum
ü Cooking sauces
ü Crisps
ü Tabletop sweeteners
ü Drink powders
ü Flavored water
ü Sugar-free products
ü Cereals
• Learnmore:
http://www.naturalnews.com/035141_aspartame_worst_sources_produc
ts.html#ixzz44SatbYMX

Anticariogenic Properties of Food
• Protein and Fat
- they do not lower plaque pH.
- Generally, protein may
contribute to buffering
effects of saliva.
- Consuming foods with fat and
protein following a
fermentable carbohydrate
may increase plaque pH.
- Meat, sea food, poultry, eggs,
nuts, seeds, margarine, and
oils are example

Other Factors Influencing
Cariogenıcıty
• Retentiveness of the carbohydrate
• How often or how long teeth are exposed
• Sequence in which a carbohydrate is consumed
• Whether food is eaten with a meal or as a snack.
• Some foods thought to have low cariogenic potential
(e.g., corn flakes, crackers, or potato chips) may be
more acidogenic than simple carbohydrate foods
because of their retentiveness in embrasures, pits,
and fissures.

Physical Form
• How quickly a cariogenic food is cleared from the
mouth is a factor related to caries development.
• Ingestion of hard candy results in prolonged
exposure.
• A sticky and retentive carbohydrate (e.g., chewy fruit
snacks) remains in contact with the enamel surface
or a longer period than sweetened fluids.
• Slow oral clearance of fermentable carbohydrate
means longer exposure of the tooth to acid attack.

Frequency of Intake
Longer periods of oral
exposure to a
fermentable
carbohydrate
greater risk of
demineralization
less opportunity for
teeth to remineralize

Frequency of Intake
• Two individuals can eat equal amounts of
fermentable carbohydrates, but the one who eats
more frequently throughout the day has the
greatest
potential
for decay
• With each exposure, a decrease in pH begins within
2 to 3 minutes; at a pH of
5.5
or less (the critical pH),
enamel
decalcifcation
occurs. Within 40 minutes, the
pH has increased to its initial value.

Frequency of Intake
• If a person eats a candy bar within a
5-minute
period,
the teeth would be exposed to a critical pH that lasts
or approximately
40 minutes
before the pH returns
to the original level.
• If another person eats the same candy bar in five
bites, but only takes a bite every hour until it is gone,
the total acid exposure would be approximately
200
minutes
- (5 bites × 40 minutes = 200 minutes of acid exposure).

Frequency of Intake
• Soft drinks, sports drinks, energy drinks, and favored
coffees and teas
- The pH of diet and regular soft drinks, bottled iced teas,
and sports drinks ranges rom 2.5 to 3.5
- Fruit juice should be limited to
• 4 to 6 oz per day for children 1 to 6 years old
• 8 to 12 oz per day or children 7 to 18 years old
*1 0z = 29,5735296875 ml
Timing and Sequence in a Meal
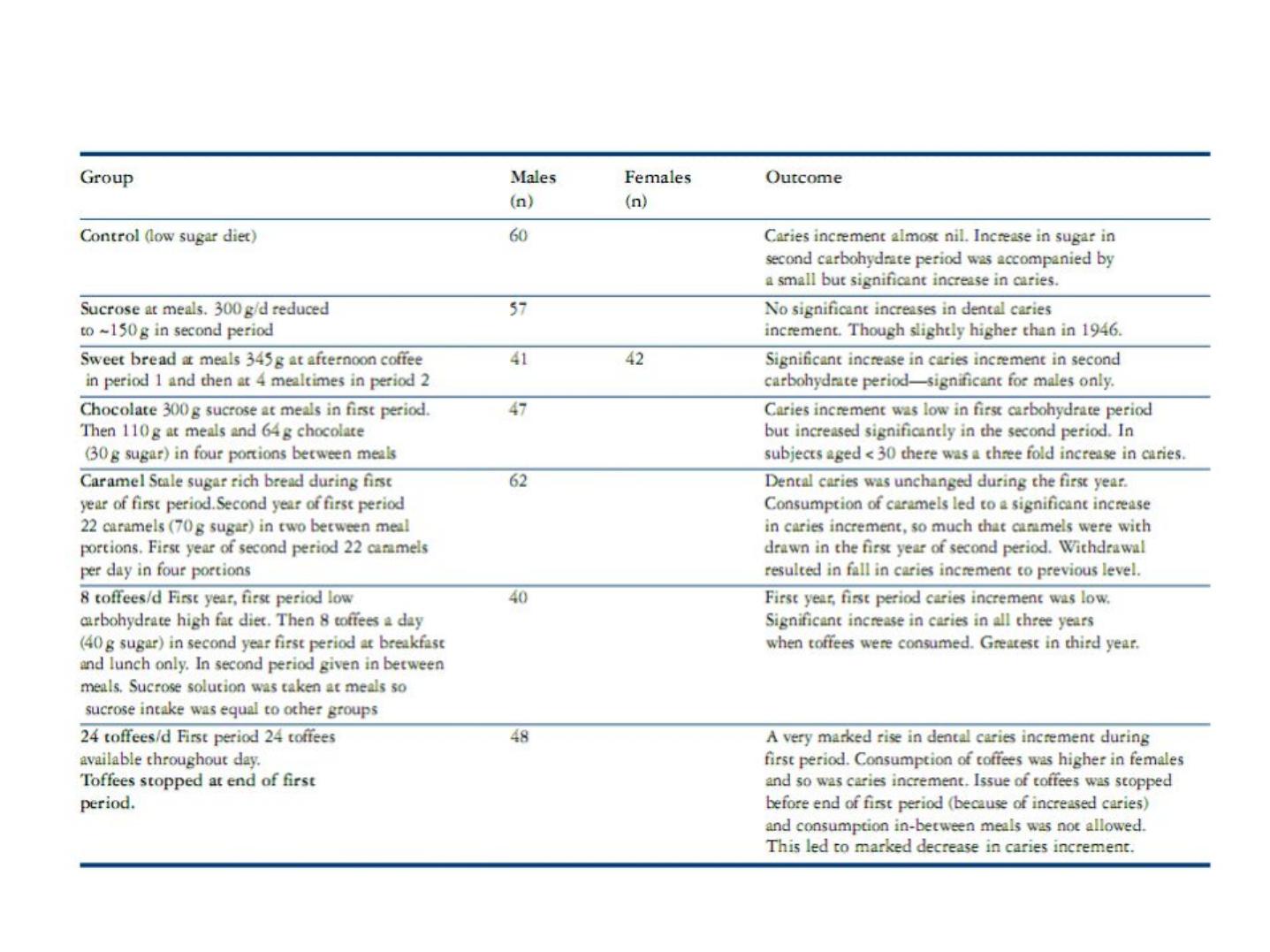
• The Vipeholm study
- conducted shortly after the Second World War in an adult
mental institution in Sweden between 1945 and 1953
The Vipeholm study
• The study investigated the effects of consuming sugary
foods of
varying stickiness
(i.e. different oral retention
times) and
at different times
through-out the day on the
development of caries by measuring caries increment in
subjects who consumed
- (1) refined sugars with a slight tendency to be retained in the
mouth at meal times only (e.g. sucrose solution, chocolate)
- (2) refined sugars with a strong tendency to be retained in the
mouth at meal times only (e.g. sweetened bread)
- (3) refined sugars with a strong tendency to be retained in the
mouth, in between meals (e.g. toffee)
The Vipeholm study

The Vipeholm study
• The first carbohydrate period was between 1947 and
1949 and the second carbohydrate period in which
the regimens were changed slightly ran between
1949 and 1951.

The Vipeholm study
• Main conclusions of the Vipeholm study
- Sugar intake, even when consumed in large amounts, had
little effect on caries increment if it was ingested up to a
maximum of four times a day at mealtimes only
- Consumption of sugar in-between meals was associated
with a marked increase in dental caries
- The increase in dental caries activity disappears on
withdrawal of sugar-rich foods
- Dental caries experience showed wide individual variation

The Turku Sugar Studies
• A controlled longitudinal study carried out in Finland in the
1970s
• Study investigated the effect of almost total substitution of
sucrose in a normal diet with either fructose or xylitol on caries
development
• Three groups of subjects (n = 125 in total)
• Subjects aged 12–53 years, with 65% being in their twenties,
• Consumed a diet sweetened with either sucrose, fructose, or
xylitol for a period of 25 months
• Dental caries increment was monitored blind at six-month
intervals by one person throughout the study and both carious
cavities and precavitation lesions were monitored
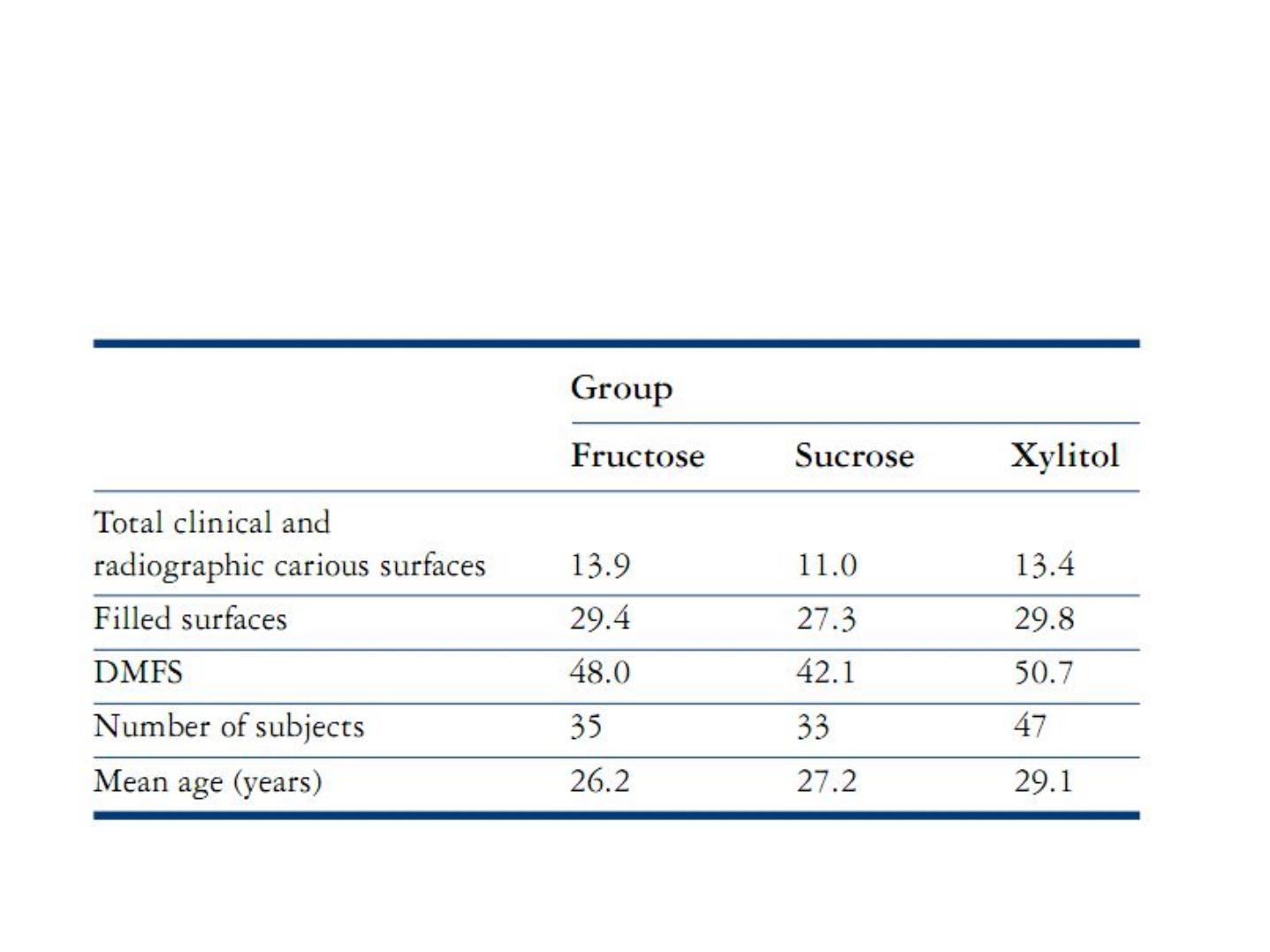
The Turku Sugar Studies
The baseline conditions of the 115 subjects who completed the 2-year Turku
sugar study

The Turku sugar studies
• Foods were specially manufactured for the fructose
and xylitol groups and intake of starch was not
restricted but subjects were asked to avoid sweet
fruits such as dried fruits since sugars in these foods
could not be substituted.

The Turku Sugar Studies
• The xylitol group consumed xylitol-containing foods
significantly less frequently than the sucrose or
fructose groups consumed their sweetened foods
and the overall intake of xylitol in the xylitol group
was lower than that of sucrose or fructose in the
other groups
• An 85% reduction in dental caries was observed in
the xylitol group who had removed sugar from their
diet
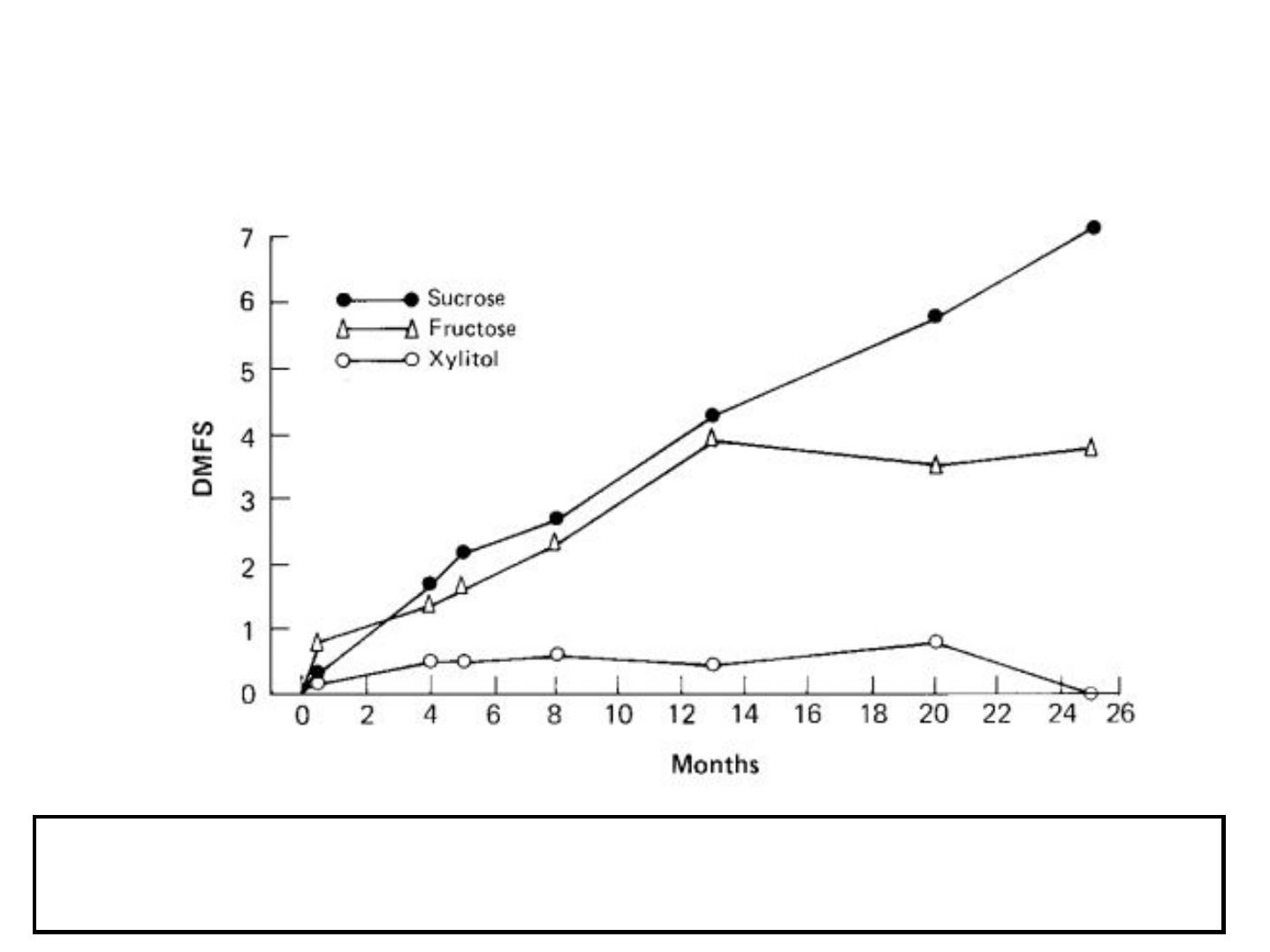
The Turku Sugar Studies
The cumulative development of decayed, missing or filled surfaces including cavitation and pre-
cavitation carious lesions, diagnosed both clinically and radiographically, but not including secondary
caries. At 24 months, differences between all groups were statistically significant (p< 0.01).

The Turku Sugar Studies
• The main conclusions of the
Turku study are that
substitution of sucrose with
xylitol
resulted in a
markedly
lower dental caries increment
in
both cavities and at the pre-
cavitation stage.