ACUTE KIDNEY INJURY
Hussien Mohammed JumaahCABM
Lecturer in internal medicine
Mosul College of Medicine
Thursday, 24 march, 2016

Acute kidney injury (AKI), also referred to as acute renal failure, is a sudden and often reversible loss of renal function, which develops over days or weeks and is usually accompanied by a reduction in urine volume.
In uncomplicated AKI, such as that due to haemorrhage or drugs, mortality is low, even when renal replacement therapy (RRT) is required.
In AKI associated with serious infection and multiple organ failure, mortality is 50–70%.
AKI: Pathophysiology
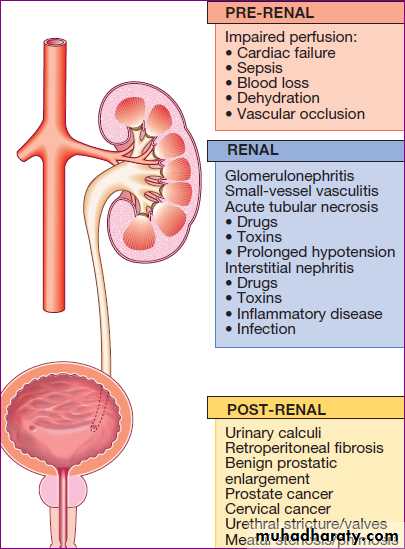
classified into three subtypes:a. ‘prerenal’, perfusion to the kidney is reduced , leading to acute tubular necrosis (ATN) .
b. ‘renal’, the primary insult affects the kidney as in GN or by nephrotoxic drugs ,which can cause ATN .
c. ‘post-renal’, when there is obstruction to urine flow at any point from the tubule to the urethra , with kidney damage arising as the result of back pressure.
Causes of acute kidney injury
AKI: Clinical features
Early recognition and intervention is important in AKI; all emergency admissions to hospital should have renal function, blood pressure, temperature and pulse checked. Coexisting diseases such as diabetes, vascular and liver diseases, which make AKI more likely, drug treatments such as ACE inhibitors and NSAIDs, which may be associated with renal dysfunction should be checked .If a high serum creatinine is found, it is important to establish whether this is an acute or acute-on-chronic, or a sign of chronic kidney disease (CKD).
Pre-renal AKI
Tachycardia and postural hypotension (a fall in blood pressure of > 20/10 mmHg from lying to standing) , signs of poor peripheral perfusion, such as delayed capillary return are valuable signs of early hypovolaemia.The cause of the hypotension is usually obvious, but concealed blood loss can occur into the GIT , following trauma (fractures of the pelvis or femur crush injuries or burns ) and into the pregnant uterus. Severe inflammatory skin diseases or sepsis.
Biochemical assessment usually reveals metabolic acidosis and hyperkalaemia.
Renal AKI
GN : Haematuria, proteinuria and clinical manifestations of an underlying disease, such as SLE. Blood tests, including an immunological screen, should be performed to clarify the diagnosis, renal biopsy is usually required. Drug-induced acute interstitial nephritis (AIN) should be suspected in a previously well patient if there is an acute deterioration of renal function coinciding with introduction of a new drug treatment.Drugs that are commonly implicated in deterioration of renal function include gentamicin, omeprazole, cisplatin and amphotericin B.Post-renal AKI
Patients should be examined clinically to look for evidence of bladder enlargement and should also undergo imaging with ultrasound to detect evidence of obstruction above the level of the bladder.Post-renal AKI is usually accompanied by hydronephrosis, but this can be absent if
the ureters are affected by fibrosis or malignancy,
or if obstruction occurs incombination with a renal disorder such as ATN that causes oliguria.
AKI : Investigations
That are required in all cases are shown in Box .Additional investigations that are required in some cases, depending on the clinical picture are shown in Box .
Various criteria have been proposed to classify AKI and to help identify high-risk patients, guide treatment and provide information regarding prognosis.
The most commonly used are the KDIGO and RIFLE criteria which use serum creatinine and urine output as biomarkers of kidney function.
• Criteria for acute kidney injury
• KDIGO (Kidney disease: improving global outcomes)• RIFLE(Risk, Injury, failure,
• loss, end-stage)
• Stage 1:
• serum creatinine increase > 1.5-1.9-fold, urine production of < 0.5 mL/kg/ hr for 6-12 hrs
• = Risk
• Stage 2:
• serum creatinine increase > 2.0-2.9-fold, urine production of < 0.5 mL/kg/ hr for ≥12 hrs
• = Injury
• Stage 3:
• serum creatinine increase> 3.0-fold, urine
• production of < 0.3 mL/kg/hr for≥24 hrs or
• absolute anuria for ≥12 hrs, or absolute serum
• creatinine > 354 µ mol /L with an acute rise of
• > 44 µ mol /L
• = Failure
• Loss: persistent AKI, or complete
• loss of kidney function for > 4 wks
• End-stage renal disease: need for RRT
• for > 3 mths
• Investigation of patients with established acute kidney injury
• Urea , creatinine• Compare to previous results. Chronically abnormal in CKD
• Electrolytes
• If potassium > 6 mmol/L, treat urgently
• Calcium and
• phosphate
• Low calcium and high phosphate may indicate CKD , Calcium low in
• rhabdomyolysis: measure CK, Hypercalcaemia in myeloma
• Albumin
• Low albumin in nephrotic syndrome
• Full blood count
• Clotting screen
• Anaemia may indicate CKD or myeloma , Anaemia and fragmented
• RBC on blood film with raised LDH in thrombotic microangiopathy
• Low platelets and abnormal coagulation in DIC, including in sepsis:
• take blood cultures
• C-reactive protein
• ESR is misleading in renal failure , High CRP may indicate sepsis or inflammatory disease
• Urinalysis
• Marked haematuria suggests GN , tumour of renal tract or
• bleeding disorder . Heavy proteinuria suggests glomerular disease:
• measure PCR or ACR
• Urine microscopy
• Casts or dysmorphic RBC suggest GN .WBC suggest infection
• /interstitial nephritis, Crystals in drug-induced or uric acid
• nephropathy
• Renal ultrasound
• Hydronephrosis ± enlarged bladder in UT obstruction: consider PSA.
• Small kidneys (CKD). Asymmetric kidneys in renovascular or
• developmental disease: consider renal artery imaging
Cultures , blood, urine, sputum.
Chest X-ray Pulmonary oedema .
Globular heart in pericardial (uraemic) effusion: perform echocardiogram.
Fibrotic change in systemic inflammatory disease with lung and kidney involvement: request pulmonary function and high-resolution CT
Serology HIV and hepatitis serology is urgent if dialysis is needed
ECG If patient is > 40 yrs or has electrolyte abnormalities or risk of cardiac disease
Investigation of patients with established acute kidney injury - cont'd
• Clinical features and investigations of specific causes of acute kidney injury - cont'd
Possibility
• considerVascular occlusion
Aorta, or renal artery to single kidney;
Pointers include missing pulses, anuria
Urgent arteriography
Doppler ultrasound
Malignant hypertension
BP very high; RBC fragments on blood
film and haemolysis
Examine optic fundi
Check previous BP readings
Scleroderma
Sclerodactyly, other features.
Autoantibodies to extractable nuclear antigens. Imaging
Systemic inflammatory disease
Multi-organ involvement, rash and
evidence of glomerular disease
Differential diagnosis includes infection,
especially endocarditis or TB.
Complement, ANCA, ANF, anti-GBM antibodies,
cryoglobulins and biopsy
Cultures, echocardiogram
• Clinical features and investigations of specific causes of acute kidney injury - cont'd
• Glomerular disease
• Heavy proteinuria and/or haematuria• Screen for systemic inflammatory disease Plus urgent renal biopsy, unless cause already known
• Interstitial nephritis
• Consider if urinary abnormalities minor but leucocytes present. Usually non- oliguric in early stages.
• Eosinophilia and urinary eosinophils
• Renal biopsy
• Uric acid if tumour lysis possible
• Myeloma
• Extra renal features may be present, including bone pain and hypercalcaemia. Renal disease can occur without overt myeloma. Often presents with interstitial nephritis but cast formation can be acute, so patients frequently oliguric
• FBC, calcium, skeletal survey, bone marrow aspirate
• Serum immunoglobulins and protein electrophoresis
• Check urinary light chains
• Consider renal biopsy
• Infections
• Leptospirosis, hantavirus, syphilis, poststreptococcal glomerulonephritis
• ASO titre and other serological tests for infection
• (ANCA = antineutrophil cytoplasmic antibodies; ANF = antinuclear factor; ASO = anti- streptolysin)
• FBC = full blood count; GBM =glomerular basement membrane
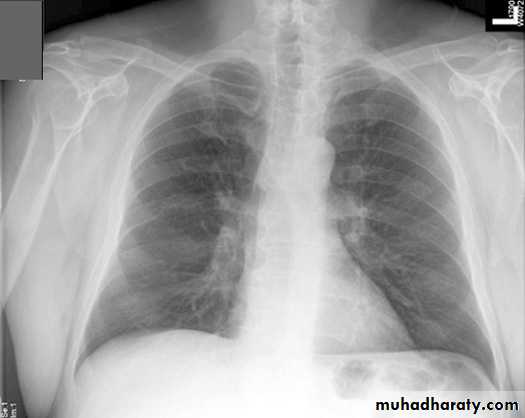
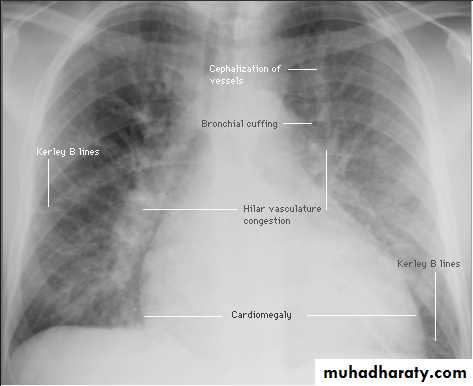
Pulmonary oedema in acute kidney injury. The appearances are indistinguishable from left ventricular failure but the heart size is usually normal.
Normal
LVF
AKI :Management
Haemodynamic statusIf hypovolaemia is present, it should be corrected by replacement of IV fluid or blood; excessive
administration of fluid should be avoided, since this
can cause pulmonary oedema.
Monitoring of the central venous Pressure(CVP) may be of value in determining the rate of administration of fluid.
Hartmann’s or Ringer’s lactate, may be preferable to isotonic (0.9%) saline when large volumes of fluid resuscitation are required, in order to avoid hyperchloraemic acidosis.
AKI :Management cont'd
Low-dose dopamine in acute kidney injuryCritically ill patients may require inotropic drugs to restore an effective blood pressure 'Dopamine at low, "renal" doses has been used in the belief that it may increase renal blood flow in critically ill patients and prevent AKI.
However, meta-analysis of clinical trials does not support its use in patients with, or at risk of, acute kidney injury.'
AKI :Management cont'd
Administration of hydroxyethyl starch solutions should be avoided in the resuscitation of critically ill patients, since they have been associated with a greater requirement for RRT and mortality .Hyperkalaemia and acidosis
Common, particularly in patients with sepsis, burns, haemolysis or metabolic acidosis . If serum K+ > 6.5 mmol/L, should be treated immediately to prevent life-threatening cardiac arrhythmias.
Restoration of blood volume will correct acidosis.
Infusions of sodium bicarbonate (50 mL of 8.4%) may also be used, if acidosis is severe.
AKI :Management cont'd
Cardiopulmonary complications
Pulmonary oedema may result from the administration of excessive amounts of fluids relative to urine output and increased pulmonary capillary permeability.
Dialysis may be required to remove excess fluid.
Temporary respiratory support may be necessary with continuous positive airways pressure (CPAP) or intermittent positive pressure ventilation (IPPV),
fluid intake should be matched to urine output plus 500 mL (insensible losses) unless diarrhoea is present, in which case additional fluids might be required.
AKI :Management cont'd
Electrolyte disturbancesSuch as dilutional hyponatraemia, may occur if the patient has continued to drink freely despite oliguria or has received inappropriate amounts of IV dextrose. They can be avoided by paying careful attention to fluid balance.
Modest hypocalcaemia is common but rarely requires treatment.
Phosphate levels are usually high but may fall to low levels in patients on dialysis or haemofiltration, necessitating phosphate replacement.
AKI :Management cont'd
Dietary measures
Adequate nutritional support should be ensured with sufficient amounts of energy and adequate amounts of protein; high protein intake should be avoided, particularly in patients with sepsis and burns who are hypercatabolic. Enteral or parenteral nutrition may be required .
Infection
Patients at substantial risk of infection because humoral and cellular immune mechanisms are depressed. Regular examination, microbiological investigation, is required, if infection is discovered, it should be treated promptly .
AKI :Management cont'd
MedicationsPatients with drug-induced ATN or drug-induced AIN should have the offending drug withdrawn.
NSAIDs and ACEI , should be discontinued.
H2-receptor antagonists should be given to prevent gastrointestinal bleeding. Other drug treatments doses adjusted if necessary, to take account of renal function. Nonessential drug treatments should be stopped.
Immunosuppression
Patients with GN may require immunosuppressive drugs , plasma infusion and plasma exchange .
AKI :Management cont'd
Renal tract obstructionThe obstruction should be relieved as soon as possible. Catheterisation in urethral obstruction, or correction of ureteric obstruction with stent or percutaneous nephrostomy.
Renal replacement therapy (RRT)
Conservative management can be successful with attention to fluid balance, electrolyte and nutrition,
but RRT may be required in patients who are not showing recovery.
RRT cont'd
Typically, the decision to start RRT is driven by hyperkalaemia, fluid overload or acidosis.Severe uraemia with pericarditis and neurological signs (uraemic encephalopathy) is uncommon in AKI but, when present, is a strong indication for RRT.
No specific cut-off values for serum urea or creatinine have been identified at which RRT should be commenced, and clinical trials of earlier versus later RRT in unselected patients with AKI have not shown differences in outcome.
RRT can be a risky intervention in patients with comorbidity, since it requires the placement of large IV catheters that may become infected and can also represent a major haemodynamic challenge in unstable patients.
Accordingly, the decision to institute RRT should be made on an individual basis, taking account of the potential risks and benefits, comorbidity.
The two main options for RRT in AKI are haemodialysis (HD) and haemofiltration.
Peritoneal dialysis (PD) is also an option if HD is not available .
Recovery from AKI
Heralded by a gradual return of urine output and a steady improvement in plasma biochemistry.During recovery, there is often a diuretic phase in
which urine output increases rapidly for several days before returning to normal. This may be due to tubular damage and to temporary loss of the medullary concentration gradient and it may be necessary to provide supplements of sodium chloride, sodium bicarbonate, potassium chloride and sometimes phosphate temporarily, to compensate for increased urinary losses.
After a few days, urine volume falls to normal as the concentrating mechanism and tubular reabsorption are restored.
Management of acute kidney injury
• Correct hypovolaemia and optimise systemic haemodynamic status with inotropic drugs if necessary• Administer glucose and insulin to correct hyperkalemia if K+ > 6.5 mmol/L
• Consider administering sodium bicarbonate (100 mmol) to correct acidosis if pH < 7.0 (> 100 nmol/L)
• Discontinue potentially nephrotoxic drugs and reduce doses of therapeutic drugs according to level of renal function
• Match fluid intake to urine output plus an additional 500 mL to cover insensible losses once patient is euvolaemic
• Measure body weight on a regular basis as a guide to fluid requirements
• Ensure adequate nutritional support
• Administer proton pump antagonists to reduce the risk of upper gastrointestinal bleeding
• Screen for intercurrent infections and treat promptly if present
Acute kidney injury in old age
Physiological change: nephrons decline in number with age and average GFR falls progressively.Creatinine: as muscle mass falls with age, less creatinine is produced each day. Serum creatinine can be misleading as a guide to renal function.
Renal tubular function: declines with age, leading to loss of urinary concentrating ability.
Drugs: increased drug prescription in older people (diuretics, ACEI and NSAIDs) may contribute to risk of AKI.
Causes: infection, renal vascular disease, prostatic obstruction, hypovolaemia and severe cardiac dysfunction .
Mortality: rises with age, primarily because of comorbid conditions.