د. حسين محمد جمعه
اختصاصي الامراض الباطنةالبورد العربي
كلية طب الموصل
2012

Interpreting the Coronary-Artery Calcium Score
NEJM january 26, 2012A 55-year-old white man presented with an abnormal
coronary-artery calcium (CAC) score. He exercised regularly and was asymptomatic. There was nofamily history of premature coronary artery disease (CAD). He was not overweight, had never
smoked, and did not have diabetes.
His blood pressure was 122/78 mm Hg.
In 2006, he had undergone an electron-beam computed tomographic (CT) scan in response to
a newspaper ad. His CAC score was 39.
He underwent a repeat scan in 2011 and had a
CAC score of 119. The radiologist at the imaging facility told him that he was “in danger of heart
attack and might not make it to 60.” His only medication was rosuvastatin, which he had been
taking at a 5-mg dose daily for 3 years. His high-density lipoprotein (HDL) cholesterol level was
43 mg per deciliter, and his lowdensity lipoprotein (LDL) cholesterol level was 86 mg per deciliter.
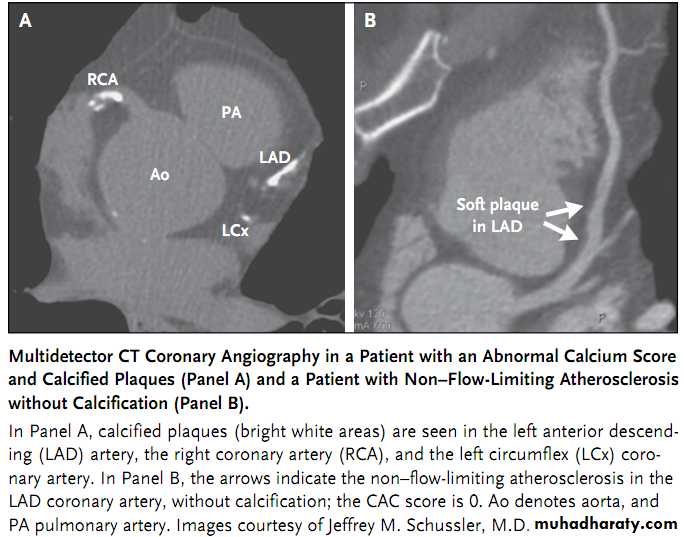
More than half of Americans will die of cardiovascular disease, and many of those will have sudden cardiac death or acute myocardial infarction as its first manifestation. Therefore, the ability to screen for early CAD is appealing from a preventive heath perspective. CAC scoring is a sensitive and quantitative method of detecting calcium in the coronary arteries (see images).
Because CAC is almost always found within atherosclerotic plaque, a positive CAC score directly identifies the presence of CAD.
Recent studies of CAC scoring have focused primarily on risk stratification.
There is unanimous agreement among the guidelines thatCAC scoring is not helpful in screening patients at either very low risk or high risk for CAD.
Guidelines vary on the question of whether it’s indicated for screening asymptomatic patients at intermediate risk for CAD, usually defined as those with aFramingham risk score of 10 to 20% over 10 years (1 to 2% per year).
Screening of symptomatic patients with known CAD is not
helpful.
A recent study of 10,037 symptomatic patients undergoing CT coronary angiography showed that the absence of CAC did not rule out the presence of obstructive CAD, nor did CAC scoring add incremental prognostic information to that provided by clinical risk factors and the severity of CAD.
So far, there have been no prospective randomized, controlled trials demonstrating that an abnormal CAC score influences treatment decisions or outcomes.
The limitations of applying CAC scoring to screening broad populations are numerous and have
been extensively reviewed. Nevertheless, CAC scoring is offered to the public by direct advertising.
Such ads typically suggest paying with a flexible spending account, health insurance, or cash. Physician referral is not needed. Patients who undergo self-referred CAC scoring and have a positive
score are told to go to their physician for advice. How does aphysician interpret a CAC score and counsel a patient such as the one described above?
A number of obvious clinical questions arise. Is a CAC score of 119 considered high? What is the significance of the increase in CAC score from 39 to 119 over a
5-year period? This patient was told that he was in danger of aheart attack and might not make
it to the age of 60. Was that true? Did he need stress testing or coronary angiography? The website
of the facility that performed his scan states that “the higher the calcium score, the greater the likelihood of a future coronary event such as a heart attack or the
need for angioplasty, stents or bypass surgery.”
The patient therefore believed that the areas of
CAC would require treatment with stents or bypass surgery. Was that true? If not, what therapyshould have been prescribed? In considering these questions, it’s important to evaluate the
CAC score within the clinical context.
As a rule, data from the Multi-Ethnic Study of Atherosclerosis (MESA) and other trials suggest that a CAC score below 100 indicates low risk, and a score above 300 indicates high risk.
The Framingham risk calculator yields a 10-year risk of cardiac death or myocardial infarction of 4.5% (<0.5% per year) in the patient described above. According to the guidelines, CAC scoring was not needed, because this man’s predicted coronary event rate was low.
Nevertheless, recent evidence from MESA indicates that CAC scoring can significantly reclassify risk.
The MESA website contains a useful tool that incorporates the CAC score as well as clinical risk factors. According to the MESA arterial age calculator
(www.mesa-nhlbi.org), this patient’s 10-year risk of death or myocardial infarction would be
reclassified from 4.5% according to the Framingham scale to 10% with a CAC score of 39 and 12%
with a CAC score of 119. Yet although the relative risk is more than doubled, the absolute risk is
roughly 1% per year, so the statement that he was “in danger of aheart attack and may not make it
to 60” was misleading and unduly alarming.
Although the change in CAC score from 39 to 119 seems to suggest progression of CAD, it only slightly increased this man’s risk of myocardial infarction or death due to cardiac causes. Interestingly, had this patient’s total cholesterol level been only 10 mg per deciliter higher, his MESA risk score would have increased from 12% to 20% with a CAC
score of 119 — a disparity that highlights the need to consider CAC scores only in the context of other clinical risk factors, particularly cholesterol levels and blood pressure.
A stress test can be very helpful in patients with abnormal CAC scores to evaluate functional
capacity and the presence or absence of ischemia. It can also help to reassure an anxious patient. An abnormal CAC score in an asymptomatic patient is not an indication for coronary angiography, nor are stents or bypass surgery indicated to treat CAC.
The abnormal CAC score should simply be viewed as documentation of coronary atherosclerosis,
the appropriate treatment for which is lifestyle modification, reduction of blood pressure and
LDL cholesterol levels, and antiplatelet agents. Were the patient to develop a clinical indication
for coronary revascularization, such as an acute coronary syndrome, the “culprit” lesion might
turn out to be a noncalcified plaque.
In an intravascular ultrasound study of the natural history of CAD, the plaque characteristics most predictive of subsequent coronary events were plaque burden, thin fibrous cap, and small luminal area (<4 mm2), not coronary calcium.
Therefore, the areas of coronary calcium visualized by
CT are not necessarily the same lesions that cause subsequent coronary events.
It should also be remembered that a CAC score of 0 does not mean that CAD is absent,particularly in younger patients who may have soft fatty atheromas.
Although the CAC score has not been shown to affect outcomes or change the appropriate therapy, it can be useful in encouraging medical compliance.
A recent randomized trial demonstrated that subjects who underwent CAC scoring before counseling about risk-factor modification had greater improvements in systolic blood pressure, LDL cholesterol levels, and waist circumference than subjects who did not undergo CAC scoring.
Thus, an abnormal CAC score may motivate some patients to take their prescribed medications and follow recommended lifestyle changes.
The patient described above was very anxious about his abnormal CAC score and the finding that it had increased between 2006 and 2011.
A stress echocardiogram was ordered. He exercised for 13.5 minutes, in accordance with the Bruce protocol, and had no symptoms, electrocardiographic changes, or wall-motion abnormalities.
He was given dietary instruction and prescribed 325 mg of aspirin daily, and his rosuvastatin dose was increased to 20 mg daily. There are no plans to obtain a follow-up CAC score.