Diagnosis of Helicobacter pylori infection
BMJ 24 February 2012د. حسين محمد جمعه
اختصاصي الامراض الباطنة
البورد العربي
كلية طب الموصل
2012
The article explores how to test for Helicobacter pylori infection and when to check whether treatment has worked.
A 32 year old nurse presents with intermittent discomfort in her upper abdomen for more than five months, particularly when fasting. She denies any weight loss, recurrent vomiting, dysphagia, fever, or a change in bowel habits. There is no evidence of gastrointestinal bleeding. She takes no medications,
including over the counter non-steroidal anti-inflammatory drugs. She does not smoke and drinks about 4 units of alcohol a week. Abdominal examination shows mild epigastric tenderness.
What is the next investigation?
Dyspepsia in patients younger than 55 years presenting without alarm symptoms does not require endoscopic investigation.Empirical treatment with a proton pump inhibitor or the “test and treat” strategy for Helicobacter pylori infection are recommended management strategies in this setting and are equally cost effective in relation to symptom control.
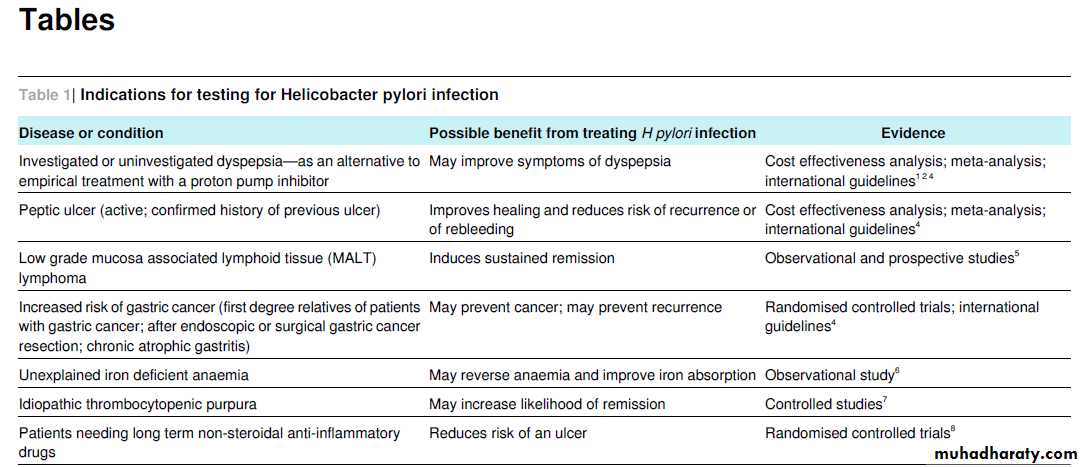
H pylori infection is usually acquired during childhood, and the prevalence is high (70-90%) in Asia, Africa, South America, and eastern Europe and low in western Europe and North America (30%). Testing for the infection is recommended if the treatment is indicated to improve the clinical condition or outcome (table 1⇓).
Non-invasive tests
Non-invasive tests include the 13C urea breath test and the 14C urea breath test, stool antigen tests, and antibody tests in serum, blood, urine, and saliva.Urea breath tests
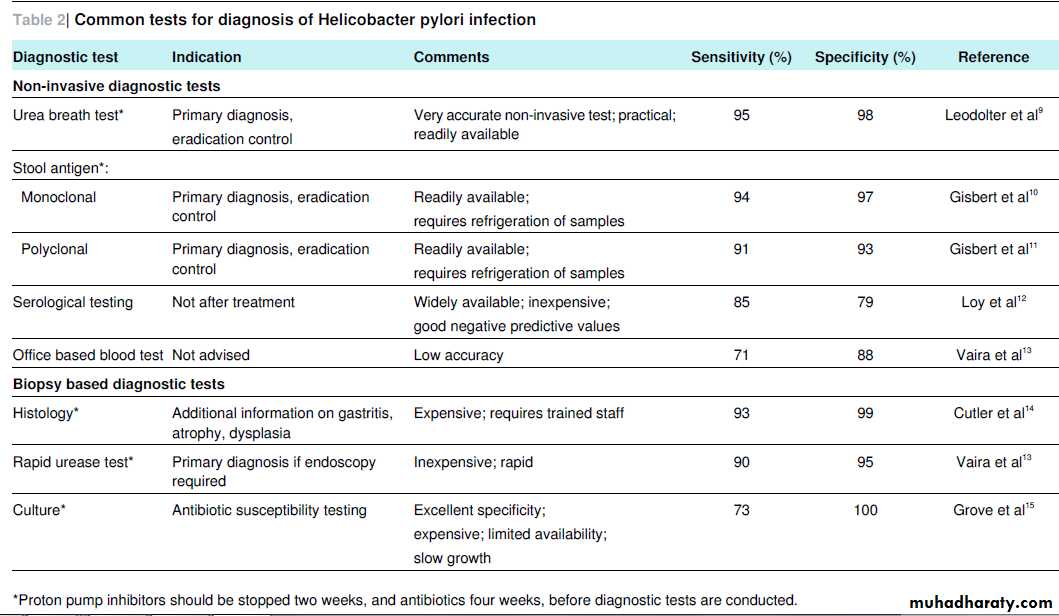
A urea breath test is the most accurate non-invasive test (table
2⇓). The 13C test is preferable to the radioactive (14C) test as it avoids any exposure to radiation. After the patient has drunk acitric acid solution containing 13C urea, the bacterial urease will hydrolyse the labelled urea to 13C carbon dioxide and ammonium.
The increase in 13C labelled carbon dioxide in breath samples (taken before and 15-30 minutes after drinking the test solution) reflects the bacterial urease activity present on the gastric mucosa, and the intensity of the 13C signal in breath correlates with the density of the bacterial colonisation.
The test should be done under fasting conditions, to optimise the contact of the test solution with the gastric mucosa. The 13C urea breath
test is widely available in primary care as breath samples are easy to collect and can be sent by mail for analysis (if not directly measured using non-dispersive, isotope selective, infrared analysers that are simple to operate).
Stool antigen test
Testing for H pylori antigen in a random stool sample using an immunoassay is also suitable for primary diagnosis (table 2⇓).In a meta-analysis, monoclonal stool antigen tests proved superior to polyclonal tests. Stool samples need refrigeration when stored before analysis.
A new, rapid, office based, one step monoclonal immunoassay for detection of H pylori antigen
in stool has shown promising results in pretreatment and
post-treatment settings and provides results within 10
minutes. Further data and cost effectiveness analysis is
needed before the one step test can be recommended for use in primary care. Disadvantages of faecal antigen tests include the aversion of patients and doctors to stool samples and the difficult logistics and the precautions needed in handling, storing, and
disposing of faecal samples.
Serological testing
Serological testing is the cheapest and most widely available method of testing. However, avoid using it for primary diagnosis when the more accurate breath or stool tests are available because it indicates only previous exposure, not current H pylori infection.
Generally, serological testing has a high negative
predictive value, but its positive predictive value depends on the pretest probability of H pylori infection, which in turn depends on the patient’s age, the prevalence of infection in his or her country of origin, and his or her socioeconomic status.Office based blood tests12 or antibody detection in urine or saliva are even less accurate and should not have a role in patient management.
Biopsy based tests
Refer for endoscopy any patients with new onset dyspepsia who are older than 55 years and patients of any age with alarm symptoms such as weight loss, dysphagia, persistent vomiting, iron deficient anaemia, or signs of gastrointestinal bleeding.Rapid urease test
If an endoscopy is indicated, the rapid urease test from antral biopsies is the test of first choice as it provides a reliable and cheap method for identifying H pylori infection.
The biopsy specimen is placed into a solution or gel containing urea and apH indicator. If H pylori is present, the urease will convert the
urea to ammonia, leading to an increase in the pH and a colour change on the pH indicator.
A recent large study comprising 1000 patients reported excellent (>90%) sensitivity and specificity for a new generation, ultrafast rapid urease test, which allows reading after only one minute.
Histology
Histology is more expensive but is also slightly more sensitive and specific than the rapid urease test and gives additional information on the type of gastritis, atrophy, intestinal metaplasia, and malignancy. If proton pump inhibitors have been taken, biopsies from the gastric body can improve the diagnostic yield. The organisms can be identified onconventional histological stains, such as Giemsa or haematoxylin and eosin; immunostaining increases sensitivity and specificity further, but its extra costs might be justified only in cases of assumed low colonisation density; it is not necessary for routine diagnostics.
Culture
Culturing of the organism from gastric biopsies is an insensitive but highly specific method, which is available only in specialised microbiology centres. Gastric biopsies for antimicrobial susceptibility testing are recommended when treatment hasfailed repeatedly.
Limiting factors
When the patient has acute bleeding or is taking proton pump inhibitors, H2 antagonists, or antibiotics, most diagnostic tests for H pylori infection (such as histology, the rapid urease test, the urea breath test, and the stool antigen test) can yield false
negative results, as shown in systematic reviews and several studies. Proton pump inhibitors should therefore be stopped two weeks before, and antibiotics four weeks before, testing for H pylori infection.
The pH buffering effect of blood in the gastric lumen might impair the tests. In cases of upper gastrointestinal bleeding or in low colonisation density of H pylori (as in MALT lymphoma
(mucosa associated lymphoid tissue lymphoma) and extensive mucosal atrophy) serological testing can be helpful as it indicates previous exposure to H pylori, although it does not confirm current infection. This diagnostic strategy is recommended by a consensus of the European Helicobacter Study Group.
Alternatively, if tests were negative at the time of gastroduodenal haemorrhage, non-invasive tests conducted four to eight weeks after the bleeding event will avoid missing an H pylori infection.
Therapy control (testing whether the treatment has worked)
Treatment for H pylori fails in about 20% of cases. Therefore, testing for eradication after treatment is advised in patients at risk of treatment failure but not generally in other patients. Do eradication testing, therefore, in those with an associated ulceror MALT lymphoma; after resection of early gastric cancer; or in those with persistent dyspeptic symptoms.
These recommendations are based largely on expert consensus agreement.
For testing whether the treatment has worked, the non-invasive 13C urea breath test or the stool antigen test is recommended, unless repeat endoscopy is needed. Serological testing isunhelpful after treatment, as antibodies persist for months or even years. The urea breath test is simple to perform and also suitable in children. The current European consensus, based on recent comparative studies, regards it as more accurate than the
faecal antigen test as a test for therapy control.
Treatment failure usually results from non-compliance or antibiotic resistance, which varies with the country of origin of the patient and previous antibiotic treatment for other conditions.
If treatment with the locally recommended second line rescue regimen fails repeatedly, referral for endoscopy is recommended so that biopsies can be obtained for susceptibility testing and culture guided treatment.
It is still not known whether molecular based methods using polymerase chain reaction in material from biopsies, stool, saliva, or string tests (in which a thread is swallowed, with one end kept outside the mouth, and pulled out again) or the direct
visualisation of the organism on the gastric mucosa using endomicroscopy will ever have a role in diagnosing H pylori infection in clinical practice.
Outcome
On the basis of her positive 13C urea breath test result, the patient received treatment for H pylori infection (omeprazole 20 mg twice daily, amoxicillin 1000 mg twice daily, and clarithromycin500 mg twice daily for 10 days). Although her dyspepsia temporarily improved after treatment, the symptoms recurred three months later.
A repeated 13C urea breath test indicated
persistent H pylori infection. Second line treatment with omeprazole 20 mg twice daily, amoxicillin 1000 mg twice daily, and levofloxacin 500 mg twice daily for 10 days resulted in lasting symptom relief.Learning points
The 13C urea breath test or the stool antigen test can be used for non-invasive screening for Helicobacter pylori in a “test and treat strategy” in younger patients presenting with dyspepsia without alarm symptoms .As proton pump inhibitors, antibiotics, and acute bleeding might cause false negative results (except in serological testing), stop proton pump inhibitors at least two weeks, and antibiotics four weeks, before testing;if gastrointestinal haemorrhage is present and tests are negative, consider serological testing or waiting four to eight weeks after the bleeding event and doing a non-invasive test (breath test or stool antigen test) then The 13C urea breath test and the stool antigen test are reliable and accurate for testing whether the treatment has worked.