Respiratory
د. حسين محمد جمعةاختصاصي الامراض الباطنة
البورد العربي
كلية طب الموصل
2011
Noninvasive ventilation refers to mechanical ventilation without the need for an invasive interface (ie, an invasive airway) between the ventilator and the patient. Noninvasive positive pressure ventilation (NPPV) is currently the preferred mode of noninvasive ventilation. Other modes that long antedated NPPV are used occasionally, including negative pressure ventilators and abdominal displacement ventilators.
Diaphragm pacers and glossopharyngeal breathing are still used for special applications.
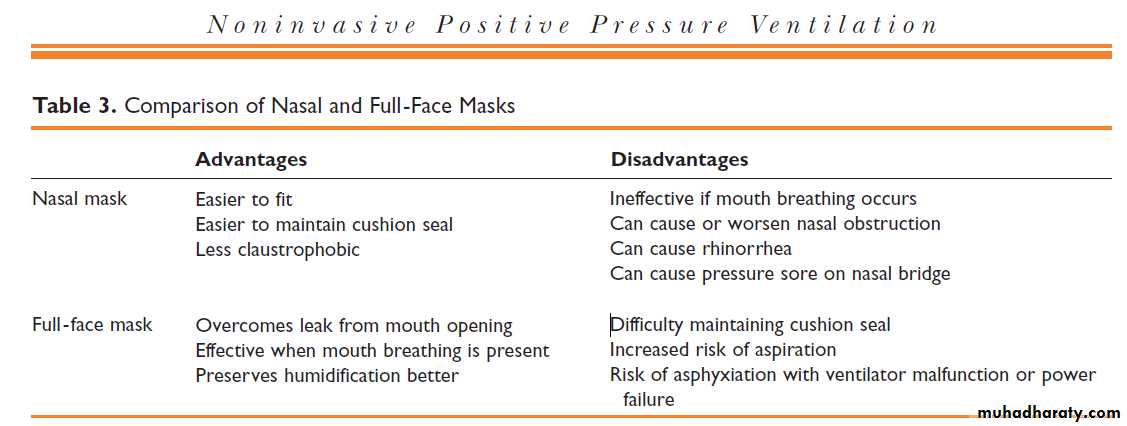
Noninvasive positive pressure ventilation (NPPV) refers to positive pressure ventilation delivered through a noninvasive interface (nasal mask, facemask, or nasal plugs), rather than an invasive interface (endotracheal tube, tracheostomy). Its use has become more common as its benefits are increasingly recognized .
There are four principal modes in which noninvasive ventilation can be used:Controlled mechanical ventilationThere is no patient effort required and the ventilator provides full ventilatory support. On NIV machines this is referred to as 'timed' mode (T). Assist control ventilationThe machine provides ventilatory support in response to the patient's breathing effort but provides back-up safety rate, should the patient not trigger the machine. This mode is referred to 'spontaneous / timed' mode on NIV machines (S/T).'
Assist modeThe machine provides ventilatory support in response to the patient's breathing effort but provides no back-up safety rate, should the patient not trigger the machine. This mode is referred to 'Spontaneous' mode on NIV machines (S).
CPAPA constant pressure is applied to the airway throughout the respiratory cycle. In acute respiratory failure, it is used primarily to correct hypoxemia. It is not a ventilatory mode and is used to correct hypoxemia in acute respiratory failure. Cardiogenic pulmonary edema is the main indication for CPAP.
Proportional assist ventilation (PAV)The ventilator assists the patient by generating volume and pressure in proportion to patient's effort creating a ventilatory pattern that matches metabolic demands on a breath-by-breath basis. Till date, there is no data to show any advantage of PAV.
Cardiogenic Pulmonary Edema. The use of NIV or CPAP in patients with cardiogenic pulmonary edema is supported by multiple randomized trials. The main physiologic benefit from NIV or CPAP in these patients is likely due to an increase in functional residual capacity that reopens collapsed alveoli and improves oxygenation. This also increases lung compliance and reduces work of breathing. The increased intrathoracic pressure also can improve cardiac performance by decreasing ventricular preload and afterload.
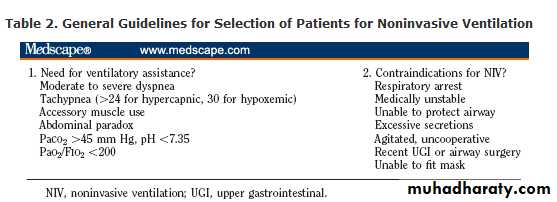
Strong evidence from randomized trials supports the use of NIV in the management of ARF to prevent endotracheal intubation in patients with COPD exacerbations or acute cardiogenic pulmonary edema, and in immunocompromised patients, as well as to facilitate extubation in patients with COPD. NIV should be contemplated in patients with postoperative respiratory failure or at high risk for postextubation respiratory failure who are otherwise good candidates for NIV, and as a means of preoxygenating critically ill patients with hypoxemia before intubation.
NIV can be considered in patients with asthma exacerbations, pneumonia, and ALI/ARDS, although the supporting evidence is fairly weak; these and other acutely ill patients should be monitored closely for signs of NIV failure until stabilized. If there are signs of NIV failure, patients should be intubated promptly before a crisis develops. The application of NIV by a trained and experienced ICU team, with careful patient selection, should optimize patient outcomes.
Mechanical ventilation is also called positive pressure ventilation. Following an inspiratory trigger, a predetermined mixture of air (ie, oxygen and other gases) is forced into the central airways and then flows into the alveoli. As the lungs inflate, the intraalveolar pressure increases. A termination signal eventually causes the ventilator to stop forcing air into the central airways and the central airway pressure decreases. Expiration follows passively, with air flowing from the higher pressure alveoli to the lower pressure central airways.
The Shrinking Heart in Chronic Obstructive Pulmonary Disease
in patients with emphysema, the cardiac silhouette on the radiograph is typically long and narrow. The common explanation for this finding is the altered, more vertical position of the heart in the thoracic cavity. The study by Barr et al. in this issue of the Journal provides an alternative explanation for this radiographic finding: a decreased left ventricular volume.1NEJM January 21, 2010
The question of whether left ventricular volume is normal in chronic obstructive pulmonary disease (COPD) has been discussed for many years.2 In the 1980s and 1990s, several techniquesbecame available to accurately measure ventricular volumes and cardiac function in patients with COPD. It was observed that in selected patients (those with the emphysematous form of thedisease), left ventricular volume and stroke volume were lower than normal.3,4
Most of these patients had leftward bowing of the interventricular septum in the early diastolic phase as a manifestation of underlying right ventricular pressure overload. Therefore, impaired left ventricular filling was thought to be the most likely cause of decreased left ventricular volume and stroke volume.
One of the most vital purposes of the combined actions of the heart and the lungs is to deliver oxygen to the tissues. Since oxygen delivery is directly related to cardiac output, a lower cardiac output in patients with COPD leads to impaired oxygen delivery. The question is whether the striking clinical resemblance between COPD and chronic heart failure can be explained in part by a factor both diseases have in common: decreased cardiac output.
NEJM January 21, 2010