Parkinson's disease initial assessment and referral
د. حسين محمد جمعةاختصاصي الامراض الباطنة
البورد العربي
كلية طب الموصل
2010
Parkinson's disease is common. Its overall prevalence is 0.2% and this rises with age. Parkinson's disease also causes considerable morbidity and can have a markedly adverse effect on a patient's quality of life and also on the lives of relatives and carers. There is a lower life expectancy in people with Parkinson's disease and this is particularly so for people with younger onset disease. Despite all this the diagnosis is often delayed or incorrect.
Delayed or incorrect diagnosis can result in the patient receiving inappropriate treatment or no treatment. The purpose of this module is to help you to have an appropriate level of suspicion for Parkinson's disease and to know when and how to refer when you do suspect it.
A soft, monotonic voice is a characteristic feature.
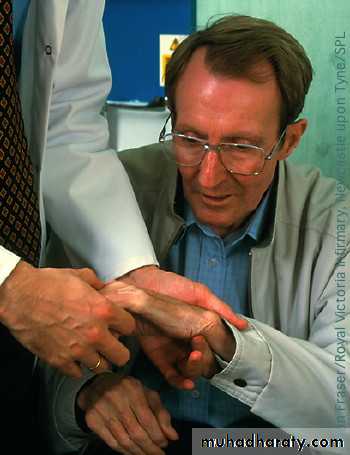
In later stages, patients also may complain of dysphagia.Cogwheel rigidity is characteristic of Parkinson's disease and it combines two of the cardinal features of the condition: tremor and rigidity.
The tremor is most prominent at rest,typically made worse by stress and tiredness and the feeling that other people notice it.
In Parkinson's disease the
symptoms are commonly asymmetric;
indeed, symmetrical symptoms often bring the diagnosis into question.
Poor arm swing on walking is typical of Parkinson's disease, and is often asymmetric.
Balance is often well preserved until later stages, and frequent falls early in the condition suggest another diagnosis. Bradykinesia (slowing of movements) is one of the
three classic features of Parkinson's disease –
bradykinesia, resting tremor, and rigidity.
symptoms are commonly asymmetric;Postural instability is usually the last cardinal symptom to appear -
Learning biteA patient's speech can also be helpful in making a diagnosis. A soft, monotonic voice .Patients commonly complain of hypernasal speech as a result of reduced ability of the soft palate to seal off the nasal cavity. Speech can lack fluency due to a "stuttering" speech pattern, frequent pauses, and repetition of syllables, sounds, or words. Difficulties changing pitch and volume result in "flattened" speech, without natural melody or rhythm.
Learning bite
Parkinson's disease is a clinical diagnosis. The classic features are:Slowing of movement (bradykinesia)
Paucity of movement (hypokinesia)
Resting tremor
Rigidity
Postural instability
The symptoms and signs are typically asymmetric in idiopathic Parkinson's disease.
The following features make idiopathic Parkinson's disease unlikely:
Frequent early falls
Prominent early dementia
Failure to respond to L-dopa therapy
Exposure to drugs that can cause parkinsonism for example metoclopramide
Cerebellar signs
Pyramidal signs
Abnormalities of eye movements
Rapid and relentless progression with early loss of mobility
Postural instability is usually the last cardinal symptom to appear - it can be disabling and result in frequent falls and loss of confidence.
Patients commonly have difficulty turning - they tend to turn “en bloc” which results in an increased risk of falling.
Difficulty turning in bed is another classic sign of Parkinson's disease.
Apathy is a particular symptom of Parkinson's, independent of depression and fatigue and responds minimally to dopaminergic drugs. Hallucinations and other forms of psychosis occur in about 40% of individuals with Parkinson's who are on dopaminergic therapy. Psychotic symptoms can take the form of vivid, complex visual hallucinations of people and animals. Auditory and olfactory hallucinations are less common. Most people with Parkinson's will have problems with sleep. A full sleep history should be taken. The merits of good sleep hygiene should be advised.
Restless legs syndrome will disturb sleep but usually responds to a low dose of dopamine agonists, clonazepam, or levodopa.
Rapid eye movement (REM) sleep behaviour disorder is characterised by loss of the normal skeletal muscle atonia during REM sleep, resulting in people physically acting out their dream (often violently) and can precede the development of the motor symptoms in up to 40% of patients.
Excessive daytime sleepiness and dozing affects up to 50% of patients with Parkinson's. Excessive daytime sleepiness can occur early in the condition and predate the diagnosis.
Bladder dysfunction can affect up to 40% of individuals. The earliest and most commonly reported complaint is nocturia followed by urgency, frequency, and urge incontinence.
Constipation occurs frequently, affecting over 50% of people with Parkinson's disease.
Hypersexuality can occur but the most commonly reported sexual problem for men with Parkinson's is erectile dysfunction.
For women, difficulty with arousal (genital sensitivity or lubrication), orgasmic difficulty, dyspareunia, or vaginismus are the primary problems
Levodopa and dopamine agonists can cause orthostatic hypotension but this can also occur as part of the disease itself. Orthostatic hypotension can occur in up to 48% of people with Parkinson's disease.
Clinical tips
When you suspect that a patient has Parkinson's disease, you should refer them quickly to a specialist. You should not start treatment before referralIf a patient with Parkinson's disease develops atypical clinical features (for example weakness or double vision or falls), you should refer the patient back to their specialist for a review of the diagnosis
Some unintended weight loss is common but severe weight loss doesn't typically occur as part of the early disease process. If it does you should think of other causes (such as malignancy). Excessive saliva or drooling occurs in many people with Parkinson's disease. Excessive sweating is typical and is often associated with dyskinesias. Pain can occur in up to 50% of people with Parkinson's disease. Patients may complain of sensory-type pains or musculoskeletal pain, secondary to parkinsonian rigidity and hypokinesia.
The tremor and shuffling gait both suggest parkinsonism. Dopaminergic antagonists (for example metoclopramide) are well known causes of parkinsonism.
Thus metoclopramide should be withdrawn: the parkinsonian symptoms should resolve. Other examples of drugs that can induce parkinsonism include:
Old antipsychotics (for example haloperidol)
New antipsychotics (for example olanzapine)
Anti-nausea agents (for example prochlorperazine)
Antihistamines (for example cinnarizine).
"Parkinson's disease is a condition that we're seeing more frequently because of the ageing population, because it's a lack of dopamine in the base of the brain and that tends to be a function along with age, with the ageing population there is a gradual increased incidence.
"Before we weren't looking so closely to find Parkinson's disease patients - but now that we're more aware more cases are being found.
Summary
"It varies quite considerably as to how patients present with Parkinson's disease. One of the most common things in my experience is people who have been falling, or they will often have a blank expression on their face, or they've just got slowed up movement, and often someone else in their family has noticed that they've got a problem.
"The classic thing you would expect is bradykinesia, which is slowing up of general movement, and a poverty of movement. They also usually have tremor and rigidity, so the classic cogwheel rigidity that you learn about at medical school is still fairly common. And it's those sort of patients you become suspicious of having Parkinson's disease.
"If someone is severely disabled because of Parkinson's disease they will ideally be seen within a fortnight up at the hospital. Failing that then within six weeks is the guideline. In reality, with the modern system it's within three months if they aren't urgent because of the choose and book system. Ideally they are seen fairly rapidly and hopefully over the next few years that will happen, because obviously it's a very worrying condition for people to have and the sooner you get a diagnosis the sooner you can start treatment.
Primary care has a really important role with patients with Parkinson's disease. When they are seen by a neurologist they are often only with them for 10-15 minutes, but their problems are daily, so one of the things we need to concentrate on is to make sure the patients have community support. And this is usually provided by Parkinson's disease nurse specialists. They will either visit the patient at home, or see them in a community clinic, and will go through all the symptoms - both motor symptoms and non motor symptoms.
"Classically we assume that the motor symptoms are worse for the patients - bradykinesia, tremor, rigidity - but often patients will be more concerned about the non motor symptoms. They vary between psychiatric and non psychiatric. Most common are anxiety and depression, which most Parkinson's disease patients will have. Occasionally some of them are psychotic, and sadly a lot of them develop dementia eventually, with what we call Lewy body dementia. Then there's the non psychiatric symptoms such as constipation, weight loss, urinary incontinence, sexual dysfunction - a whole legion of things. Often these are more distressing to them than the actual Parkinson's disease.
"So, if we as primary care workers can spot these and treat them, then we will bring the patient a lot more benefit rather than just manipulating the medication for the tremor, and they will be really, really grateful to you."