Pain relief in labor
By dr. ishraq mohammedThe method of pain relief is to some extent dependent on the previous obstetric record of the woman, the course of labor & also the estimated length of labor.
History:
History• The modern era of childbirth analgesia began in
1847 when Dr J Y Simpson administered ether
to a woman in childbirth, and later in the same
year, chloroform
• Queen Victoria was given chloroform by John
Snow (1853) for the birth of her eight child
Prince Leopold and this did much to
popularize the use of pain relief in labour
Non-pharmacological methods:
One-to-one care.Relaxation & breathing exercises.
Acupuncture & hypnosis.
Relaxation in a warm water during the first of labor.
Transcutaneous electrical nerve stimulation.

Acupuncture
• Techniques havebeen used in China
• Both for surgery as
well as for pain relief

Transcutaneous electrical nerve
stimulation• Electrical impulses are applied to
skin via electrodes
• For 1st stage electrodes are
placed over T 10 - 11 on either
side of spinous process
• For second stage analgesia
electrodes are placed over s2-s4
• Diminishes the need of analgesia
• Variable success rate
SYSTEMIC ANALGESIA FOR
LABOR ANALGESIA
Inhalational Agents
• Entonox (N2O:O2 50:50):
• Isoflurane (0.2-0.25%)
• Desflurane (1-4.5% in O2 or Entonox)
• Sevoflurane (0.5 -3%)
May cause light-headedness & nausea.
It is not suitable for prolonged use.

Pharmacological agents:
SYSTEMIC ANALGESIAIV Opioids-
• Most commonly used class of drugs
Primary mechanism of action:
-Analgesia and/or heavy sedation.
Drugs can be given in intermittent doses or via Patient
controlled analgesia
Inexpensive & can be administered by midwives.
provide only limited pain relief during labor & have significant side effects.

Side effects of opioids
• Nausea, vomiting,• maternal drowsiness & depression.
• delayed gastric emptying.
• All opioids cross the placenta. In utero opioid
exposure results in short term respiratory depression of the fetus.
Possible interference with breastfeeding.
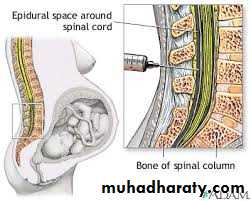
Epidural analgesia:
Epidural analgesia is a commonly employed technique of providing pain relief during labor. Induction of epidural analgesia in early labor remains controversial. However, many physicians induce analgesia as soon as the diagnosis of active labor has been established and the patient has requested pain relief. Retrospective studies have demonstrated an association between epidural analgesia and increases in duration of labor, instrumental vaginal delivery and cesarean section for labor. However, several recent prospective studies have concluded that epidural analgesia does not adversely affect the progress of labor or increase the rate of cesarean section. These remain controversial issues among practicing physicians.Advantage of epidural:
Provides superior pain relief during first and second stages of laborFacilitates patient cooperation during labor and delivery
Provides anesthesia for episiotomy or forceps delivery
Allows extension of anesthesia for cesarean delivery
Avoids opioid-induced maternal and neonatal respiratory depression
Indications of epidural:
Prolonged labor.
Maternal hypertensive disorders
Multiple gestation
Certain maternal medical condition
A high risk of operative intervention.
Patient refusal
Active maternal hemorrhageMaternal septicemia or untreated febrile illness
Infection at or near needle insertion site
Maternal coagulopathy (inherited or acquired)
Hypovolaemia
Insufficient numbers of trained staff.
• Contraindications to Epidural Analgesia
Complication of epidural :
ImmediateHypotension (systolic blood pressure <100 mm Hg or a decrease of 25 percent below preblock average)
Urinary retention
Local anesthetic–induced convulsions*drug toxicity
Local anesthetic–induced cardiac arrest*drug toxicity
Delayed
Postdural puncture headache
Transient backache
Epidural abscess or meningitis*
Permanent neurologic deficit*
• .
Accidental total spinal anasthesia(injection of epidural doses of local anasthetic into the subarachnoid space)causes sever hypotension, respiratory failure, unconsciousness & death. The mother requires intubation, ventilation& circulatory support.
Spinal haematoma & neurological complications are rare.
Short term respiratory depression of the baby due to opioids.
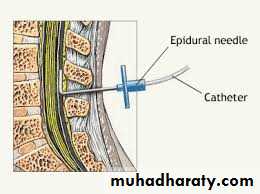
Technique:
The epidural catheter is inserted at the L2-L3,L3-L4 or L4-L5.The catheter is aspirated to check for position & if on blood or CSF is obtained. A small dose of diluted local anasthetic agent is given, if no loss of sensation of lower limb , the catheter is correctly inserted. If loss of sensation in the lower limb, then spinal anasthesia.
Combining the opioids with the local anasthetics reduces the local anasthesia required & this reduce the motor block & peripheral autonomic effects of the epidural.
Loading dose is given & then intermittent bolus or continuous infusions . Blood pressure should be monitored every 5 minutes for 15 minutes.
Spinal anesthesia:
More effective & faster onset.A spinal needle is passed through the epidural space, through the dura & into the subarachnoid space, which contain the CSF .
A small volume of local anesthetic is injected, after which the spinal needle is withdrawn. This may be used as the anesthesia for CS, trial of instrumental deliveries, manual removal of placenta & the repair of difficult perineal & vaginal tear.
Spinals are not used for routine analgesia in labor.
Combined spinal- epidural (CSE) analgesia :
This has the advantage of rapid onset of pain relief & the provision of prolonged analgesia. This is an option for pain relief in labor.