Control of Acute Respiratory Tract Infections(ARI)
Dr. Nadia AzizC.A.B.C.M.
Department of Community Medicine
Baghdad Medical College
Objectives
1- Determine the causative agents that cause the ARI.2- Identify the burden of ARI on the community.
3- Identify the causative agent of viral influenza, its occurrence.
4- The ways to prevent and control the occurrence of an epidemic.
Introduction
ARI responsible for 20% of childhood (< 5 years) deathsARI mortality highest
– HIV-infected
– in children under 2 year of age
– Malnourished
– Weaned early
– Poorly educated parents
– Difficult access to healthcare
Introduction
- Most young children worldwide have 4 to 8 episodes of respiratory infections per year.
- Incidence of acute lower respiratory infections (pneumonia) is very high in developing countries
- Four millions child die each year due to ARI.
Anatomical classification
Upper respiratory tract infection1- Pharangitis
2- Tonsillitis
3- Sinusitis
4- Otitis media
5- Laryngotracheobronchitis
6- Epiglositis
Anatomical classification
Acute lower respiratory tract infection1- Bronchiolitis
2- pneumonia

Risk factors
MalnutritionLow birth weight
Absence of breast feeding
Vitamine A defficency
Indoor air pollution
Low socioeconomic status
Poor hygiene
Missing EPI vaccination
Etiological agents
VirusesPara influanzae virus
Respiratory syncytial virus
Influenza virus
Bacteria
Streptococcus pneumoniaHaemophilus influanzae
INFLUENZA ICD-10 J10, J11
Identification
An acute viral disease of the respiratory tract characterized by:
fever, headache, myalgia, prostration, coryza, sore throat and cough.
Cough is often severe and protracted.
other manifestations are self-limited in most patients, with recovery in 2–7 days.
INFLUENZA
Differential DiagnosisInfluenza may be clinically indistinguishable from disease caused by other respiratory viruses and undifferentiated acute respiratory disease.
INFLUENZA
Influenza derives its importance from:- The rapidity with which epidemics evolve
- The widespread morbidity
- The seriousness of complications(viral and bacterial pneumonias).
- Emergence among humans of influenza viruses with new surface proteins can cause pandemics
INFLUENZA
High risk groupSevere illness and death occur among:
- The elderly
- Debilitated by chronic cardiac, pulmonary, renal or metabolic disease.
- Anemia or immunosuppression.
Complication
Reye syndrome
- Involving the CNS and liver, is a rare but serious complication following virus infections in children who have ingested salicylates.
- Children and teenagers recovering from chickenpox or flu-like symptoms should never take aspirin.
Diagnosis
Isolation of influenza viruses from pharyngeal or nasal secretions or washings on cell culture or in embryonated eggs.Direct identification of viral antigens in nasopharyngeal cells and fluids (FA test or ELISA).
Rapid diagnostic tests
Viral RNA amplification (used to identify small amounts of RNA in test samples)
Infectious agents
Three types of influenza virus are recognized:A, B and C.
Type A includes 15 subtypes of which only 2 (H1and H3) are associated with widespread epidemics.
Type B is infrequently associated with regional or widespread epidemics.
Type C with sporadic cases and minor localized outbreaks.
Infectious agents
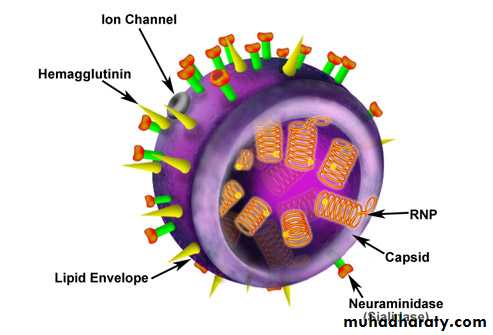
The antigenic properties of the 2 relativelystable internal structural proteins, the nucleoprotein and the matrix
protein, determine virus type.
Infectious agents
Influenza A subtypes are classified by the antigenic properties of surface glycoproteins: Hemagglutinin (H)
Neuraminidase (N).
Frequent mutation of the
glycoproteins of influenza A and influenza B viruses results in emergence of new variants.
Infectious agents
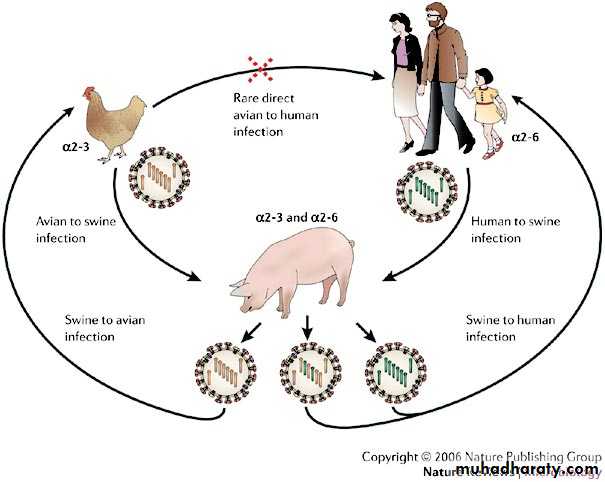
Pandemics results from:1- Emergence of completely new subtypes at irregular intervals (only for type A) results from antigenic shift in HA gene
Minor antigenic changes (antigenic drift) of A and B viruses responsible for frequent epidemics and regional outbreaks and require annual reformulation of influenza vaccine.
Infectious agents
Pandemics2- Unpredictable recombination of human and mammalian or
avian antigens.
INFLUENZA
OccurrenceAs pandemics (rare), epidemics (almost annual),
localized outbreaks and sporadic cases.
Ranking as global health emergencies (pandemic e.g. 1918, 1957, 1968) with millions of deaths (40 million in 1918).
INFLUENZA
Influenza viral infections with different antigenic subtypes also occur naturally in swine, horses, mink and seals, and in many other domesticspecies in many parts of the world.
Aquatic birds are a natural reservoir and carrier for all influenza virus subtypes.
INFLUENZA
ReservoirHumans are the primary reservoir
for human infections.
Birds and mammalian
reservoirs such as swine

INFLUENZA
Mode of transmission
Airborne spread
INFLUENZA
Incubation periodShort, usually 1–3 days.
INFLUENZA
Susceptibilityimpact of epidemics and pandemics depend upon: level of protective immunity in the population, strain
virulence, extent of antigenic variation of new viruses and number of previous infections.
Pandemics (emergence of a new subtype): Total population immunologically naive
Methods of control
A. Preventive measures:1) Educate the public and health care personnel in basic personal hygiene, especially transmission via unprotected coughs and sneezes, and from hand to mucous membrane.
Vaccine
2) Immunization withInactivated and live virus vaccines may provide 70%–80% protection against infection in healthy young adults.
Live vaccines, used in the Russian Federation for many years, registered for intranasal application
in healthy individuals aged 5–49.
Vaccine
In the elderly
Inactivated vaccines may reduce severity of disease and incidence of complications and deaths.
Vaccine
Two doses more than 1 month apart are essential for children under 9.Routine immunization programs directed towards:
- Those at risk of serious complications or death
- Those who might spread infection (health care personnel and household contacts of high-risk persons).
- Immunization of children on aspirin treatment to prevent development of Reye syndrome.
Vaccine
Contraindications:Allergic hypersensitivity to egg protein
or other vaccine components is a contraindication.
Chemoprophylaxis
3) Effective chemoprophylaxis of influenza A: Amantadine hydrochloride (CNS side-effects)Rimantadine hydrochloride
Chemoprophylaxis
Oseltamivir have been shown to be safe and effective for both prophylaxis and treatment of influenza A and B.B. Control of patient, contacts and the immediate environment
1) Report to local health authority:
Reporting outbreaks or laboratory-confirmed cases Class 1.
Control of patient, contacts and the immediate environment
In epidemicsisolate patients (especially infants and young
children)
Control of patient, contacts and the immediate environment
Protection of contacts:A specific role has been shown for antiviral chemoprophylaxis with amantadine or rimantadine against type A strains
Control of patient, contacts and the immediate environment
Specific treatment: Amantadine or Rimantadine started within 48 hours of onset of influenza A illness and given forapproximately 3–5 days in 2 divided doses
Control of patient, contacts and the immediate environment
During treatment with either drugs, drug-resistant viruses may emerge late in the course of treatment and be transmitted to others.Epidemic Measures
- health care personnel should be immunized annually.- Maintaining adequate supplies of antiviral drugs would be desirable to treat high-risk patients and essential personnel in the event of the emergence of a new pandemic strain for which no suitable vaccine is available in time for the initial wave.
Thank You
&
Good Luck