1
Learning outcomes
1. Define injury
2. Value the preventable aspect of injury
3. Describe the public health burden of injury
4. Identify codes in ICD-10 for recording and classifying injuries
5. Identify classification systems for injury
6. Definition of surveillance
7. Describe the possible uses of injury surveillance
8. List the steps required for building injury surveillance system
9. List two data sources for Iraq Injury Surveillance System
10. Describe the 3 phases in the history of Iraq Injury Surveillance System
Definition of Injury
“Injury”
is used to describe the physical damage that result when a human
body is suddenly or briefly subjected to
intolerable levels of energy
. It can be a bodily
lesion resulting from acute exposure to energy in amounts that exceed the threshold of
physiological tolerance, or it can be an impairment of function resulting from a
lack of
one or more vital elements
i.e. water, air, warmth, as in drowning, strangulation or
freezing
.
Injuries have traditionally been regarded as
random, unavoidable “accidents”.
Within the last few decades, however, a better understanding of the nature of injuries
has changed these old attitudes, and today both unintentional and intentional injuries
are viewed as largely
preventable events
.
As a result of this shift in perception, injuries
and their health implications have demanded the attention of decision-makers
worldwide and injury policy has been firmly placed in the public health arena.
Furthermore, the growing acceptance of injuries as a preventable public health
problem over the past decade or so has led to the
development of preventative
strategies
and, consequently, a decrease in the human death toll due to injuries in some
countries.
2
Public health burden
Globally
, more than nine people die every minute from injuries or violence
.
About 15 million being injured each year
.
Injuries are the third most
important
cause of
health loss in children and young people, and the fifth most important cause of health
loss across all age groups
.
Higher rate of injuries are in the developing countries
(like our country Iraq)
and lower rate are in the rich countries.
The Human Rights Ministry of the Iraqi government recorded
250,000
Iraqi
injuries between 2003 and 2012. Death from injuries in >5 years old age group makes
Iraq in the third, second and first stage in the world during the years 2004, 2005 and
2006 ,consequently
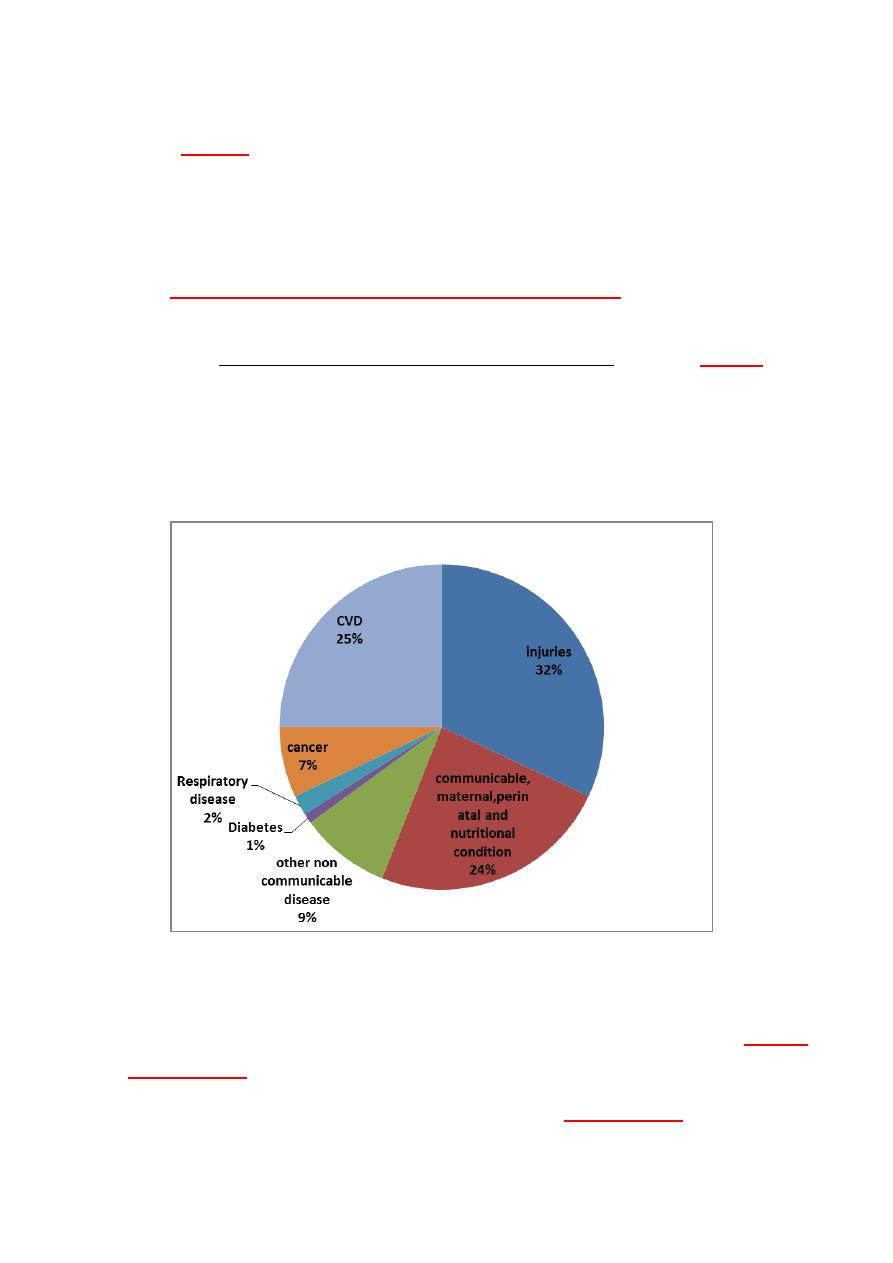
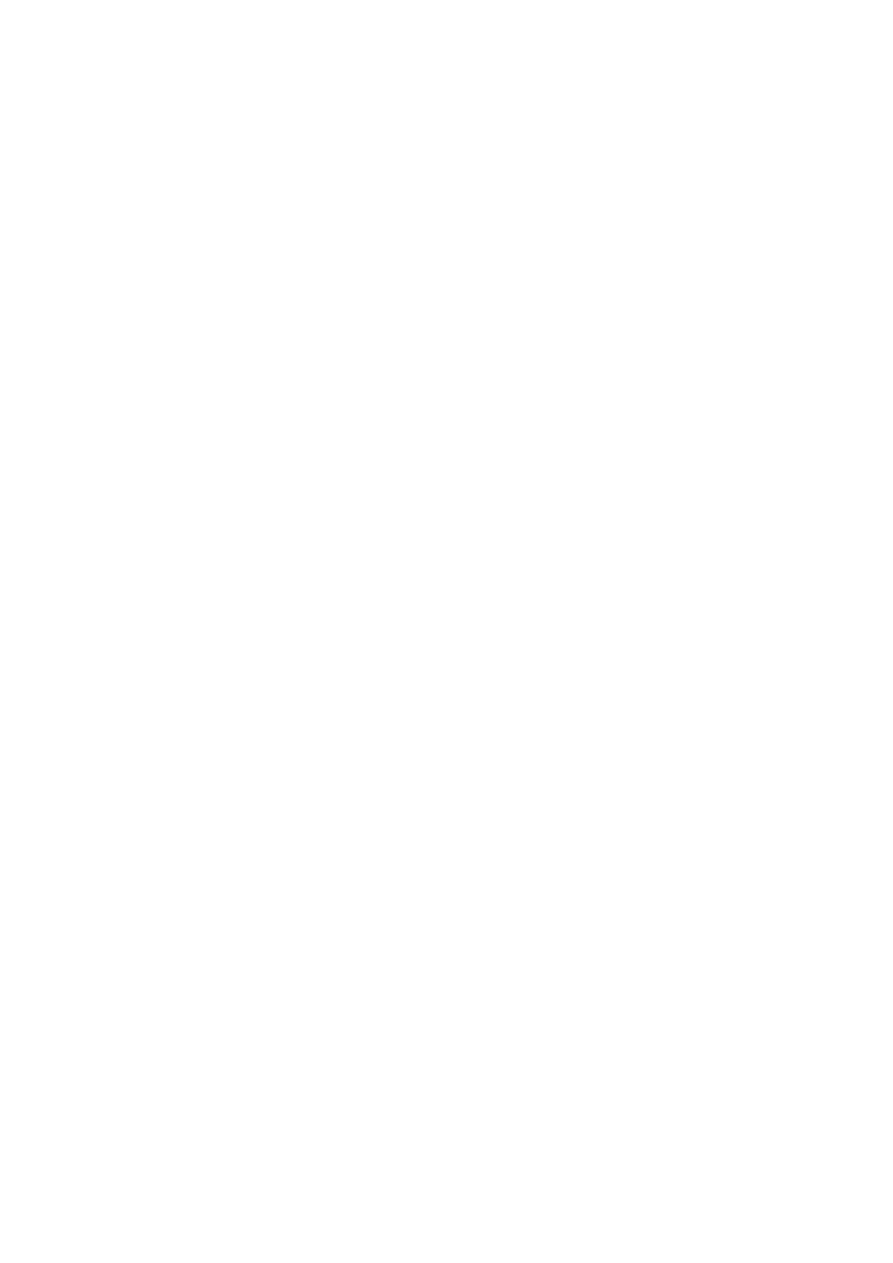
Figure 1: Proportional mortality-(percentages of total deaths, all ages in Iraq
2011).
According to World Health Organization - NCD Country Profiles, 2011,
Injuries
estimates 32 %
of all deaths in Iraq 2010 as shown above
.
Injuries have physical, emotional, and financial
consequences
that can impact
the lives of individuals, families, and society.

3
The ICD-IO Classifications of Injuries
The "S" series of codes (S00-S99) was used to classify injuries related to single
"body region". The 10 body regions are the following:
The "T" series of codes (T00-T98) Injuries involving multiple body regions are
assigned to T00-T07.
The letter V is used for transport accidents.
Specific codes Injury Classifications
Injuries are classified according to specific codes in the International
Classification of Diseases (ICD) Manual. These codes provide information on
Intent of the injury (e.g., assault-related, intentionally self-inflicted,
unintentional or "accidental").
Cause of injury, such as fall or motor vehicle crash.
Nature and anatomic location of the injury (e.g., multiple fractures involving
skull or face, dislocation of hip).
Natural classifications
Physical: 1-mechanical a-trauma (I-blunt II- sharp) b-road traffic c-fall. 2-thermal-Fire
and burns, freezing. 3-radiation 4-vibratory 5-lightning 6-sound 7-air
suffocations, drowning 8-pressure 9-electrica.
Chemical: 1-acidic 2-alkaline 3- poisons
4
Definition of Surveillance
Surveillance has been defined as Systematic and
continuous
collection
,
analysis
, and
interpretation
of data, closely integrated with the timely and
coherent dissemination of the results and assessment to those who have the right
to know so that action can be taken.
It implies a
proactive mechanism
for identifying problems and
implementing appropriate preventive strategies on a routine basis.
Injury surveillance may be regarded as a specific form of public health
audit
. It can be designed to generate information on both the numbers and
characteristics of injuries, such as the injury location, circumstances, cause, and
mechanism. This information is
crucial for
:
detecting trends in injury incidence.
identifying risk factors.
developing injury control measures and assessing their impact.
This process is thus an epidemiological means to a public health end,
namely prevention.
Another essential role of public health surveillance is
monitoring causes of death
, including premature mortality. In that context,
injuries clearly emerge as a major public health problem.
.
Information about injuries is required at both
national and local levels
.
Nationally, injury data are used by government departments for policy making
and priority setting; by researchers investigating epidemiology, treatment, and
prevention; and by a range of other voluntary and commercial organizations
interested in injury.
5
Locally, injury data are required for planning health services, developing
and implementing safety policies and standards, and for evaluating the
effectiveness of interventions.
Iraq Injury Surveillance System
The Iraqi Sentinel Injury Surveillance System started collecting data since
2010
supported by WHO, UNICEF, CDC Atlanta, UN developmental program. The
experimental phase
of the program started 1/7/2008 in 4 provinces Baghdad Rusafa,
Basrah, Kerbala, Arbil. The
second phase
started in 1/1/2009 to include
further 5
provinces
, Misan, Anbar, Mosel, Suleimania, Baghdad Karch. The
third phase
started
1/1/2013 to include
all Iraqi provinces
.
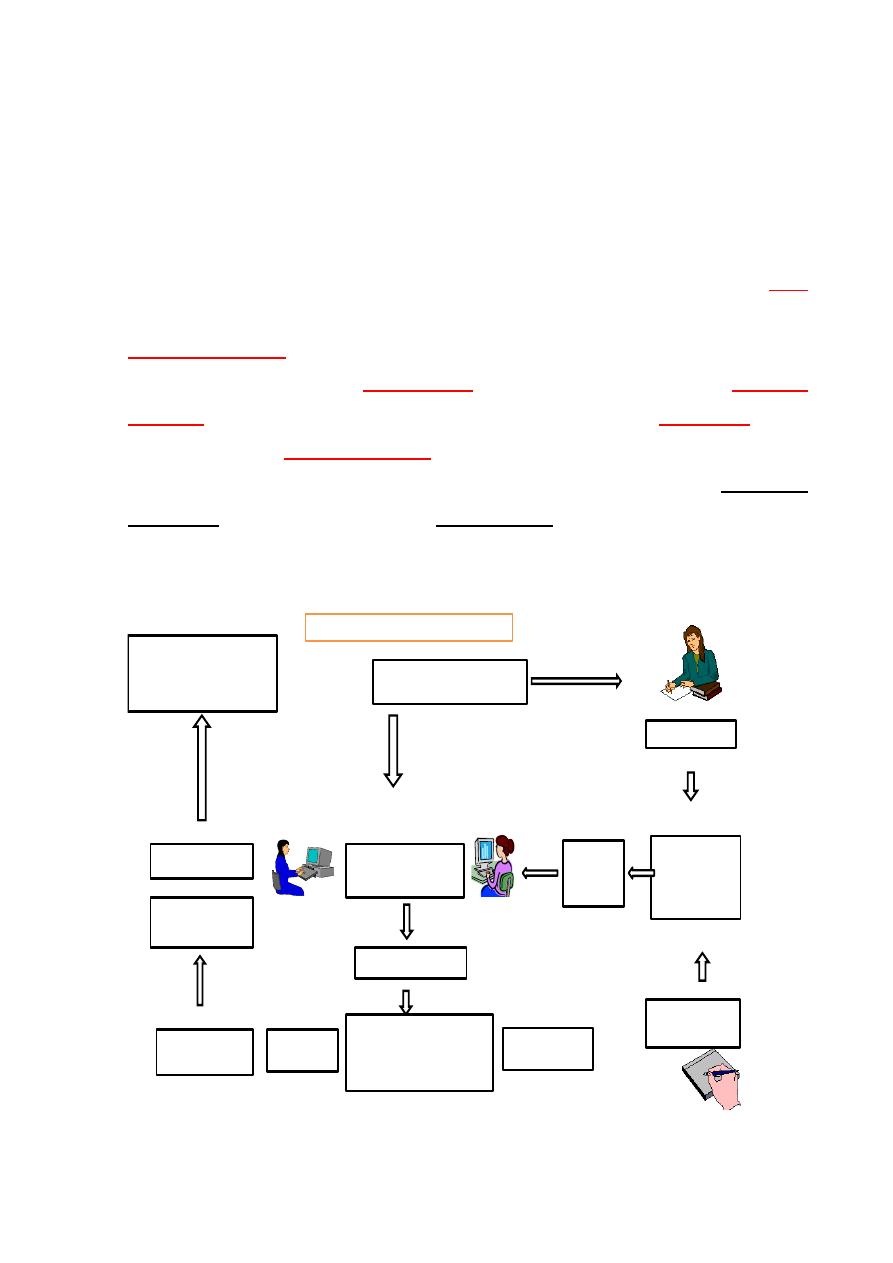
Data are collected from injured patients or witness in the emergency
department of the hospitals and from forensic office by officials are included in the
program by trained staff using special formula, which is fed to the computers by
trained community department staff, using (Epi_info) program.
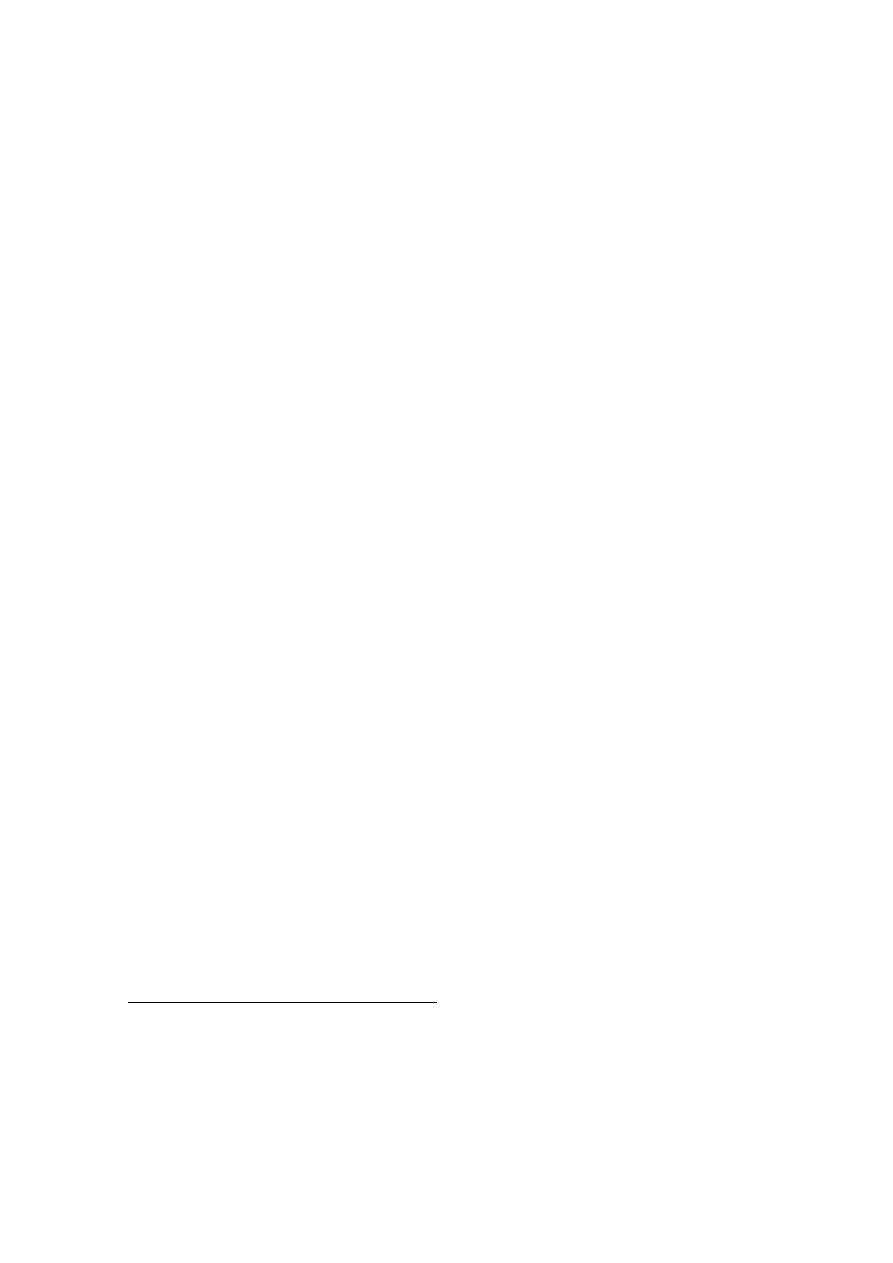
Coroner Office
Emergency
Room
(
daily filling
of form)
Weekly
collection
Data entrance to Epi-Info
In Medical Operations
Department in H.D.
Medical Operations
Department
Ministry of Health
Sending by E-Mail monthly
Merge data
Interpretati
on, analysis
Prepares reports
Related Ministries
WHO
Preventive programs
(
Monitoring, evaluation
Iraqi sentinel injury surveillance system(ISISS
)
5
Figure 2: Showing the stages in collecting of data by Iraqi Sentinel Injury
Surveillance System
6
How to design and build an injury surveillance
system
Next steps can help to build an injury surveillance system:
Step 1: Identify stakeholders.
Any agency or individual who is concerned about injuries and thus may
have an interest in injury surveillance can be considered to be a potential
stakeholder, for example: Health care workers, administrators and policy makers
working for public agencies or for nongovernmental organizations (NGOs) with
interests in health or injury issues. Other agencies that have interest in collecting
data are considered like insurance companies, educational institutions, legal
institutions and social welfare agencies.
Step 2: Define system objectives. Some possible objectives are:
To assess the contribution of injuries in general to the overall burden of
disease in the country or community.
To determine the incidence and other characteristics of a particular type of
injury.
To identify populations at high risk from particular injuries.
Step 3: Define
“a case”.
It depends on the objectives of the surveillance system. For example:
If
the objective is to monitor the burden of care on a given service, then a “case” will be
any visit (first or repeat) to that service by an injured person or by a person who was
not in fact injured but only suspected he/she might be injured. If the objective is to
monitor the incidence of different types of injury, then a case will be an injury
presented by one person for the first time. Repeat visits for the treatment of the same
injury will not count as separate cases.
7
Step 4: Identify data sources.
Examples of potential data sources are: Autopsy/pathology reports, police
reports, hospital in-patient records, trauma registries and ambulance or Emergency
Medical Technician (EMT) records.
Step 5: Assess available resources.
These may include: personnel with sufficient expertise not only to
complete forms and/or extract data from them, but also to process the data and
produce reports, equipment and supplies (e.g. computers, if existing or
affordable), reliable electricity supplies to run computers, manually operated
devices, forms, computer diskettes).
Step 6: Inform and involve stakeholders.
By convincing stakeholders that surveillance is useful, and their
commitment to it should be secured. It will be of enormous benefit in the long
run if it can involve stakeholders in the design and establishment of the system.
They will develop a strong sense of ownership of the completed system; this in
turn will help to make it sustainable.
Step 7: Define data needs.
This depends on the priorities of the system. However, certain minimum
data sets are recommended that is to say there is a least amount of data that we
consider a system needs to collect in order to be useful for injury surveillance
purposes. Extra information can be readily added to these minimum data sets,
according to specific requirements and circumstances.
Using standard classifications and codes
:
It is critical to use standard classifications and codes. By doing this, data
collected by your injury surveillance system can be compared and collated with
data collected by other injury surveillance systems. This will enable community-
by-community and country-by-country comparisons.

8
Ultimately, it will provide more accurate worldwide estimates of the extent
of the injury problem. The WHO has been supporting efforts to establish
international standards for classifying and coding data on injuries. The work is
now complete and the results can be found in two publications:
1. The International Statistical Classification of Diseases and Related Health
Problems 10th Revision (ICD10) contains 21 major classification
categories. Two of the major categories are devoted to injuries and external
causes of morbidity and mortality
(27)
. These are category 19 and 20 as
shown below:
XIX S00–T98 Injury, poisoning and certain other consequences of
external causes.
XX V01–Y98 External causes of morbidity and mortality.
2. International Classification of the External Causes of Injury (ICECI)
.
Step 8: Collect data:
It is better to build on existing systems, whenever possible. If there is a
system in place that already collects and processes most or even some of the
data wanted, it could be used as the basis for the surveillance system. It may be
possible to extend the existing system to gather all of the data needed, with only
minor modifications to the forms already in use and with little or no added
burden on the staff that currently operate the system.
Another possibility is to coordinate several existing systems by persuading
the separate agencies to use the same forms or, at least, revise their forms so that
they are consistent. Of course, seeking advice from a statistician can help with
form design and ensure that the information obtained is as easy as possible to
collate and process.
Step 9: Establish a data processing system.
Data processing systems can be either manual or electronic.

9
Step 10: Design and distribute reports.
If electronic means of data processing are used, the production of basic
reports should be both automatic and prompt.
Step 11: Train staff and activate the system.
Step 12: Monitor and evaluate the system.
Once it is up and running, your surveillance system should be continually
monitored and periodically evaluated, so that problems are detected and
remedied as soon as they emerge.