Carcinoma of the breast: is the most common cause of death in middle aged women in western countries. In 2004 approximately one and half million new cases were diagnosed worldwide. In England and Wales one in 12 women will develop the disease during their life time.


(1) Geographical: it occurs most commonly in western world, accounting 3-5% of all death in women. In developing countries it accounts for 1-3% of death.
(2) Age: it is extremely rare below the age of 20 years but thereafter the incidence steadily rise that by the age of 90 years nearly 20% of women are affected.
(3) Gender: it is less than 0.5% of patients with breast cancer are male.
(4) Genetics: it occurs more commonly in women with a family history of breast cancer than in general population. Breast cancer related to specific mutation account for about 5% of breast cancer.
(5) Diet: there is some evidence that there is a link with diets low in phytoestreogen, a high intake of alcohol is associated with increase risk. Diets are recommended are walnut, broccoli, peach and curcuma.




(6) Endocrine: it is more common in nulliparous women and breast feeding in particular approved to be protective. Also protective in having a first child at an early age, especially if associated with late menarche and early menopause. It is known that in postmenopausal, breast cancer is more in obese. This is thought to be because of increased conversion of steroid hormone to oestrodiol in the body fat.
(7) previous radiation; this was considered to be historical interest, with the majority of women exposed to the atomic bombs at Hiroshima and Nagasaki having dead, again using of utilized uranium in Iraq war play a role in this disease. It is, however a real problem in women who have been treated with mantle radiotherapy as a part of the management of Hodgkin lymphoma disease, in which significant dose of radiation is received. The risk appears about decade after treatment and is higher if radiotherapy occurred during breast development.

Pathology: breast cancer may arise from the epithelium of the duct system anywhere from the nipple end of major lactiferous ducts to the terminal duct unit, which is in breast lobule. The disease may be entirely in situ, an increasingly common finding with the advent of breast cancer screening or may be invasive cancer. The degree of differentiation of the tumor is usually described using three grades as well differentiation, moderately differentiation or poorly differentiation. Commonly numerical grading system based on the scoring of the three individual factors (nuclear pleomorphism, tubular formation, and mitotic rate) is used in grade 111 cancers roughly equating the poorly differentiated group.

Previously, descriptive terms were used to classify breast cancer scirrhous meaning woody or medullary meaning brain like. More recently histological descriptions have been used. however with the increasing application of molecular markers there will be a change in the way that the breast cancers are classified, and it is likely that much more information about individual tumor will be routinely reported, such as its likelihood of metastases, and to which therapeutic agents it will be susptible. Gene array analysis of breast cancer has identified five subtypes. Some of these correlate with known markers such as estrogen receptor status.
Current nomenclature: ductal carcinoma: is the most variant with lobular carcinoma occurring about 15% of cases, there are subtypes of lobular carcinoma including the classical type which carries a better prognosis than the pleomorphic type, occasionally pictures may be mixed with both ductal and lobular features. There are different pattern of spread depending on histological type.
If there is doubt whether as tumor is predominantly lobular in type, immunohistochemical analysis using the e- cadherin antibody which reacts positively in lobular carcinoma will help in diagnosis. Rare histological variants, usually carrying a better prognosis, include colloid carcinoma whose cells produce a abundant mucin.
. Medullary carcinoma with solid sheets of large cells usually associated with a marked lymphocytic reaction. Invasive lobular carcinoma is commonly multifocal and or bilateral. Cases detected via screening program are often smaller and better differentiation than those presenting to symptomatic and are of a special type.

Cases detected via screening program are often smaller and better differentiation than those presenting to symptomatic and are of a special type. Inflammatory carcinoma is a fortunately rare, highly aggressive that present as painful swollen breast which is warm with cutanous edema; this is result of blockage of the subdermal lymphatics with cancer cells. Inflammatory carcinoma usually involves at least 1l3 of the breast and may mimic breast abscess.
A biopsy will confirm the diagnosis and show undifferentiated cells, it used to be rapidly fatal but with aggressive chemotherapy and radiotherapy and with salvage surgery the prognosis has improved considerably. In situ carcinoma is a preinvasive cancer that has not breached the epithelium basement membrane.
This was previously a rare usually asymptomatic, finding in breast biopsy specimens but is becoming increasingly common because of the advent of mammographic screening. In situ carcinoma may be ductal (DCIS) or lobular (LCIS). The latter is often being multifocal and bilateral. Both are markers for later development of invasive cancers which will develop in at least 20% of patients. Although mastectomy is curative, this constitutes overtreatment in many cases. The best treatment for carcinoma in situ is depend if it is a high grade tumor treated by excision and radiotherapy, whereas those of low grade whose tumor completely excised need no further treatment.
Staining for estrogen and progesterone receptors is now considered routine, as their presence will indicate the use of adjuvant hormone therapy with tamoxifin or the newer aromatase inhibitors as anastrazole. Tumors also stained foe c- erb2( a growth factor receptor)as patients who are positive can be treated with monoclonal antibody as trastuzumab (herciptin) either in the adjuvant or relapse sitting. The pathologist is an important member of breast cancer team (MDT) and will increasingly help decide which adjuvant therapies will be appropriate.
Paget's disease of the nipple: is a superficial manifestation of underlying disease of the breast carcinoma. It presents as eczema- like condition of the nipple and areola which persists despite local treatment. The nipple is eroded slowly and eventually disappears. If it left the underlying carcinoma will sooner or later become clinically evident. Nipple eczema should biopsied if there any doubt of its cause. Microscopically Paget's disease characterized by the presence of a large ovoid cells with abundant, clear, pale staining cytoplasm in malpighian layer of the epithelium.



Spread of the breast cancer:
(1) Local spread: the tumor increases in size and invade other portion of the breast. It tends to involve the skin and to penetrate the pectorals muscles and even the chest wall if diagnosed later.
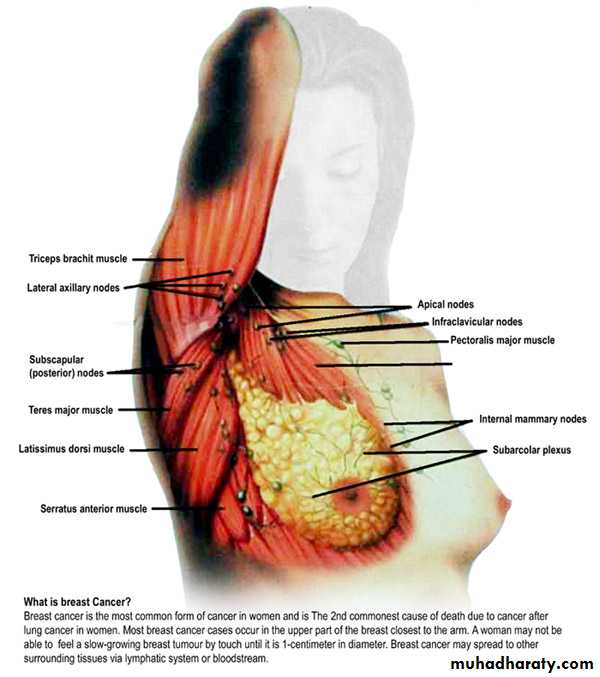
(2) Lymphatic metastasis: it occurs primarily to axillary and internal mammary lymph nodes. A tumor in the posterior one third tends to spread to internal mammary lymph nodes. The involvements of lymph nodes have both biological and chronological event in the spread of carcinoma and it also a marker of metastases potential of that tumor. Involvement of the supraclavicular lymph nodes and of any of the contra lateral breast represents advanced disease.


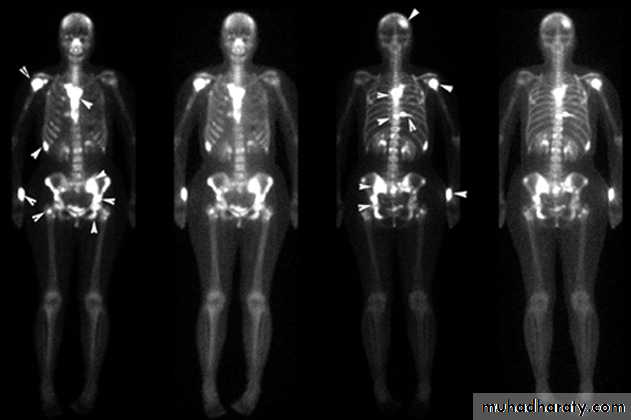
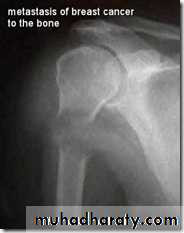
(3) Blood streams: it is by this route skeletal metastases occur. In order of the frequency the lumbar vertebrae, femur, thoracic vertebrae, rib and skull are affected and these deposits are generally osteolytic. Metastases may also commonly occur in the liver, lung, brain, and occasionally adrenal glands and ovaries.

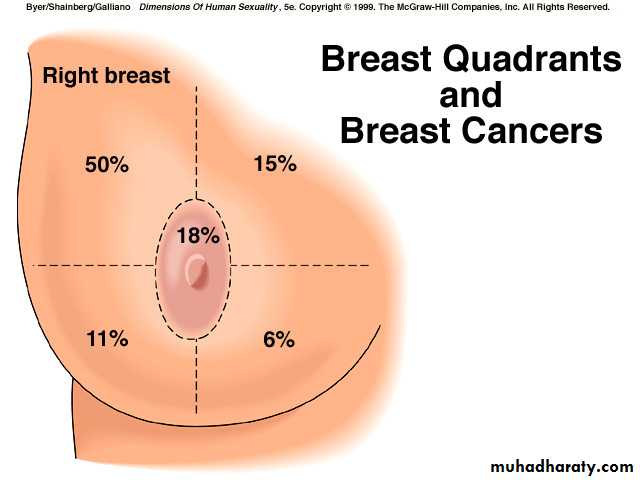
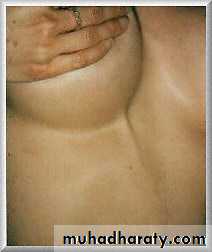
Clinical presentation: although any portion of the breast including axillary tail may be involved breast cancer is found most frequently in the upper outer quadrant most carcinoma will present as a hard lump which may be associated with indrawing of the nipple, as the disease advances locally there may be skin involvement with peau d orange or frank ulceration and fixation to the chest wall.


This is described as cancer en-cuirasses when disease progress around chest wall. About 5% carcinoma in UK presented as locally advanced or symptoms of metastatic disease this figure is much higher in developing countries. These patients under goes staging evaluation so this will include a careful clinical examination, chest x-ray, CT scan chest and abdomen and isotope scan, bone scan.
This will be important for both prognosis and treatment. A patient with wide spread visceral metastases may obtain an increased length and quality of survival from systemic hormone therapy or chemotherapy but is unlikely to benefit from surgery as she will die from her metastases before local disease becomes a problem. In contrast, patients with relatively small tumors less than 5 mm in diameter confined to the breast and ipsilateral lymph nodes, rarely need staging beyond a good clinical examination as puck up rate for distant metastases is so low. Currently, a chest x-ray, full blood count , liver function test are all that recommended for screening of the patient with early breast cancer.
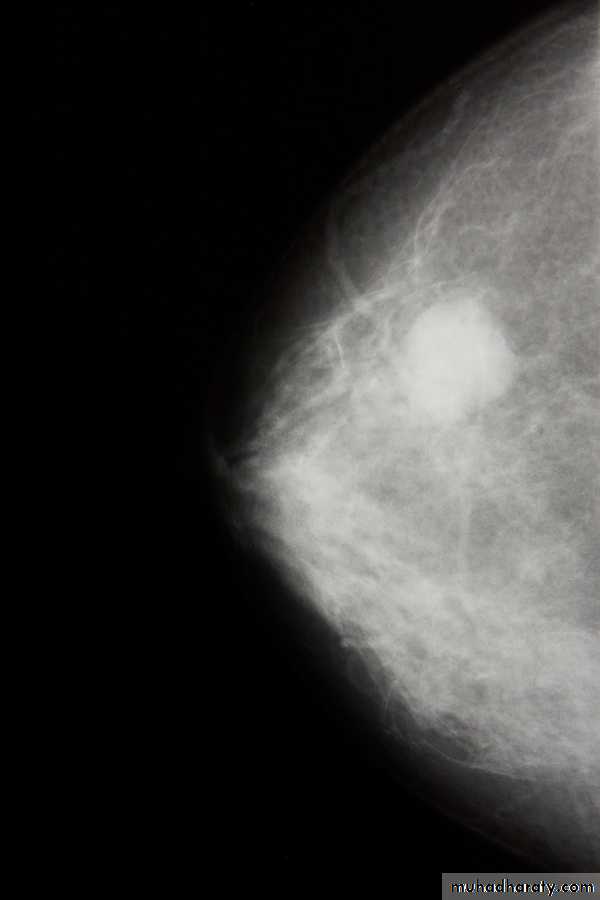
Investigations: ( 1) mammaography: soft tissue radiographs are taken by placing the breast in direct contact with ultrasensitive film and exposing it to low-voltage, high amperage x-rays. The dose of radiation is very low so it is a safe investigation. The sensitivity of this investigation increases with age as the breast becomes less dense. In total, 5% of breast cancers are missed by population –based mammographic screening programme , even in retrospect , such carcinoma are not apparent.
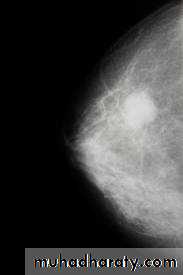

. Thus, a normal mammogram does not exclude the presence of carcinoma. Digital mammography is being introduced, which allow manipulation of the images and computer aided diagnosis. Tomo-mammography is also being assessed as a more sensitive diagnostic modality.
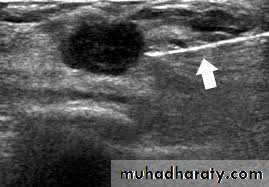
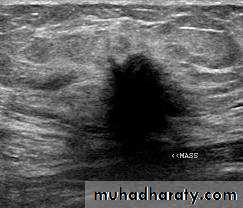
(2)ultrasound: ultrasound is particularly useful in young women with dense breasts in whom mammograms are difficult to interprets, and in distinguishing cysts from solid lesions. It also can be used to localize impalpable areas of breast pathology. It is useful as screening tool and remains operator dependent. Increasingly, ultrasound of the axillary tissue is performed when cancer is diagnosed and guided percutaneous biopsy of any suspicious glands may be performed.
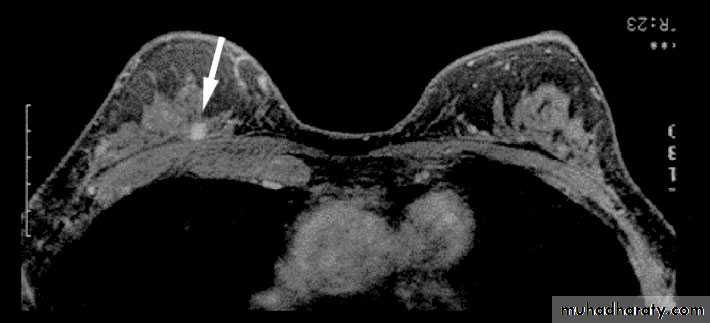
(3)magnetic resonance imaging (MRI); MRI is of increasing interest to breast surgeons in a number of setting: it can distinguish scar from recurrence in women who have had previous breast conservation therapy for cancer. It is the best imaging modality for the breast of women with implants. It has proven to be a useful as screening tool in a high risk women because of a family history. It is less useful than ultrasound in the management of the axilla in both primary breast cancer and recurrent diseases.

(4) needle biopsy/ cytology: histology can be obtained under local anesthesia using a spring loaded core needle biopsy device. Cytology is obtained using a 21 G or 23G needle and 10 ml syringe with multiple passes through the lump with negative pressure in the syringe. The aspirate is then smeared on to a slide which is air dried or fixed. Fine needle aspiration cytology (FNAC) is the least invasive technique of obtaining a cell diagnosis and is a rapid and very accurate if both operator and cytologist are experienced.
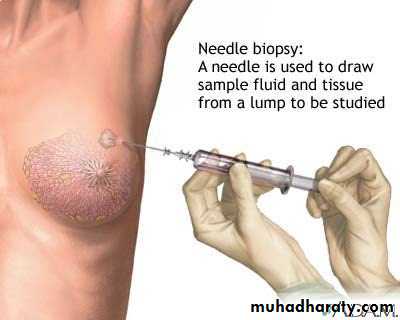
However, false negative do occurs, mainly through sampling error, and invasive cancer cannot distinguished from in situ disease. A histological specimen taken by a core biopsy allows a definitive preoperative diagnosis, differentiates between duct carcinoma in situ and invasive disease and also allows the tumor to be stained for receptor status.
This is important before commencing neoadjuvant therapy. (5)large needle biopsy with vacuum systems: the sampling error decreases as the biopsy volume increases and using 8G or 11G needles allows more extensive biopsies to be taken this is useful in management of micro calcifications or in complete excision of benign lesions such as fibroadenomas.
Triple assessment: the diagnosis should be made by a combination of clinical assessment, radiological imaging and a tissue sample taken for either cytological or histological analysis, the so called triple assessment. The positive predictive value of this combination should exceed 99.9%.
Staging of breast cancer: classical staging of breast cancer by means of TNM ( tumor, nodes, metastasis) criteria is used less often as we gain more knowledge of the biological variable that affect prognosis. It is becoming increasingly clear that it is these factors rather than anatomical mapping that influence the outcome of the disease and treatment. As shown below
group
Approximate 5 year survivalexample
treatment
Very low risk
• 90%
Screen detected DCIS
Local
Low risk prim tumor
70-90%
Node negative with favorite histology
Locoregional with or without systemic
High risk prim tumor
<70%
Node positive or unfavorite histology
Locoregional with systemic
Loca
lly advanced
<30%
Large prim or inflammatory type
Primary systemic
metastatic
------------
-------------------
Primary systemic
Prognosis of breast cancer: the best indicator of likely prognosis in breast cancer remains tumor size and lymph node status. It is realized that some large tumors remain confined to the breast for decades whereas some very small tumors are incurable at time of diagnosis. Hence the prognosis of a cancer depends not on chronological age but on its invasive and metastatic potential.
In attempt to define which tumor will behave aggressively and thus require early systemic treatment, a host of prognostic factors have been described. These include histological grade of tumor, hormone receptors status, measure of tumor proliferation such as S-phase fraction, growth factor analysis and oncogene or oncogene product measurement.
Prognostic indices as Nottingham prognostic index have combined these factors to allow subdivision of patients in to discrete prognostic group. Others put gene profile with other group indicator to give recurrence score but still unproven at moment. Others develop gene signatures said able to detect cancers of good or poor prognosis but still again unproven
Nottingham prognostic index: it depends on pathological size of the tumor in cms and node status as score 1 if no node is involved, score 2 if 1-3 nodes are involved score 3 if four or more nodes are involved. And also depend on grade of the tumor as score 1 if grade 1 and score 2 if grade 2 and score3 if grade 3.
Nottingham prognostic index= (0.2×size cm)+score node+ score grade
Prognostic group value 10 year survival %Excellent <2.4 94
Good 2.4- <3.4 83
Moderate 1 3.4-<4.4 70
Moderate2 4.4-< 5.4 51
Poor >5.4 19
Treatment of breast cancer: the two basic principles of treatment are to reduce the chance of local recurrence and the risk of metastatic spread. The treatment of early breast cancer will usually involve surgery with or without radiotherapy. Systemic therapy such as chemotherapy or hormone therapy is added if there are adverse prognostic factors such as lymph nodes involvement, indicating a high likelihood of metastases relapse. At other end of spectrum locally advanced or metastatic disease is usually treated by systemic therapy to palliate symptoms with surgery playing a much smaller role. Algorithm for management of breast cancer is shown in summary as
(1) Achieve local control
(2) Appropriate surgery include (a) wide local excision (clear margin)+radiotherapy (b) mastectomy+\- radiotherapy immediate or delayed. Combined with axillary procedure.(3) Treat risk of systemic disease by chemotherapy if prognostic factors are poor and hormone therapy if estrogen and progesterone receptor are positive.
Details of local treatment or early breast cancer: local control is achieved through surgery and or radiotherapy. The aim of treatment is to (1) cure: likely in some cases but late recurrence is possible. (2)Control local disease in breast and axilla. (3) Conservation of local form and function. (4)Prevention or delay of occurrence of distant metastases.
Surgery: still has central role to play in the management of breast cancer but have been gradual shifts toward more conservative techniques, that might show equal efficacy between mastectomy and local excision followed by radiotherapy. It was initially hoped that avoiding mastectomy would help to alleviate the considerable psychological morbidity associated with breast cancer but recent studies as has shown that over 30% of women develop significant anxiety and depression following both radical and conservative surgery .
After mastectomy women tend to worry the effect of operation on their appearance and their relationship whereas after conservative surgery they may remain fearful of recurrence. Mastectomy indicated for(1) a large tumor in relation to size of 5he breast (2) central tumor beneath or involving g the nipple(3) multifocal disease(4) local recurrence (5) patient preference.
Types of operation: the radical Halsted mastectomy including excision of breast axillary lymph nodes + pectorals major and minor, this operation is no longer preformed it cause excessive morbidity with no survival benefits. The modified radical (Patey) mastectomy is more commonly performed by preservation of pectorals major and division of pectorals minor. Simple mastectomy, wide local excision. Conservative breast surgery is aimed at removing the tumor plus a rim of at least 1 cm of normal breast tissue this called wide local excision. Lumpectomy is removal of benign lump. Quadrantectony involve removing f entire segment of the breast that contains the tumor.

Radiotherapy: it performs to the chest wall after mastectomy in selected patient in whom the risk of local recurrence is high. This includes patient with large tumor and those with large numbers of nodes or extensive lymph vascular invasion. it improve survival in women with node positive breast cancer. It is conventional to combine conservative surgery with radiotherapy to remaining breast tissue. Recently radiotherapy can be given intraoperatively at one sitting or as accelerated postoperative course.
Adjuvant systemic therapy: it was targeted at these putative micrometastases that might expect to delay relapse and prolong survival for about 30% relapse free. So women with hormone receptors positive tumors will obtain worthwhile benefit from about 5 years of endocrine therapy, either 20mg daily of tamoxifin if she s premenopausal or newer aromatase inhibitors as anastrazole (femara) or letrozole and exemstane if she is postmenopausal. No need to give these drugs in hormone negative receptors tumors.
Hormone therapy: tamoxifin (antiestrogen) is most widely used treatment in breast cancer. It reduces the annual rate of recurrence by 25% with 17% reduction in annual rate of death. It is also useful in reduce the tumor in contralateral breast. Other hormone includes LHRH agonist which induces reversible ovarian suppression and has beneficial effect as surgical or radiation induced ovarian ablation in premenopausal receptor positive tumor. It also used in recurrent tumor as it is superior on tamoxifin. The third drug is aromatase inhibitor has benefit on relapse free and less side effect.
Chemotherapy: first generation regime such as a six monthly cycle as cyclophosamide, methotraxate and 5flurouracil all is called (CMF) it reduces relapse by 25% over 10-15 years period. Modern regime include anthrocycline (doxorubicin) and newer agent such as taxanes suitable for premenopausal with poor prognosis. Recently it also given to postmenopausal patients.
Primary chemotherapy (neoadjuvant): it is being used in many centers for a large tumor but operable that requires mastectomy. The idea is to shrink the tumor before surgery to enable breast conserving surgery to be performed. Newer biological agent used frequently as molecular targets as trastuzumab (herciptin) it is active against tumor containing growth receptor c-erb2. Others as bevacizumab a vascular growth receptor inhibitor, still is not widely used.
Follow up of breast cancer: she is followed for life to detect recurrence and dissemination, so yearly or 2 yearly mammography of treated and contra lateral breast. Ultrasound of breast and abdomen can also be used; tumor marker is not routine checking for the patients.
Multidisciplinary team approach (MDT): this team including surgeon, medical oncologist , radiotherapist, and histopathologist also physiotherapist and psychologist working together for treatment decisions in breast cancer. This has been shown good for the patient to achieve good treatment
Phenomena resulting from lymphatic obstruction in advanced and breast cancer:
peau d'orange :- caused by coetaneous lymphatic edema when the infiltrated skin is tethered by the sweat ducts .it cannot swell leading to appearance like orange skin. it also seen in chronic abscess . late edema of the arm in troublesome complication of breast cancer threats .fortunately seen less often now that radical axillary dissection and radio therapy are rarely combined .

it might appears at any time from months to years after treatment .there is usually no precipitating cause but recurrent tumors should be excluded because infiltratation block both lymphatic and venous .edematous limb is susceptible for bacterial infection following quite minor trauma and this requite vigorous antibiotics .treatment of limb edema is difficult but limb elevation, elastic arm stocking and pneumatic compressive devices can be useful.
cancer-en-cuirasses:- the skin of the chest is infiltrated with carcinoma and has been likened to coat ,it may be associated with grossly swollen arm .it usually occurred with local recurrence of the mastectomy and following irradiation to the chest wall .it has poor prognosis.
lymphangiosarcoma:- is rare complication of lymphadema with an onset many years after the original treatment it take form of multiple subcutaneous nodule in the upper limb and must be distinguish from recurrent tumor .it has poor prognosis.

Familial breast cancer: - recent development in molecular genetics and the identification of number of breast cancer predisposition gene (BRCA, BRCA2, P53) have done much to stimulation interest in this area .yet women whose breast cancer is due to inherited genetic change actually account for less than 5% of all cases of breast cancer . These women have a risk of developing breast cancer that in 2-10 times above baseline .
pregnancy and breast cancers :- breast cancer presenting during pregnancy or lactation tends to be at late stage ,presumably because the symptoms are masked by the pregnancy ,however in other respect it behaves in similar way to the breast cancer in non pregnancy women .treatment is similar with some modification ,radiotherapy should be avoided ,chemotherapy is not used in first trimester but appears safe subsequently ,most tumors are hormone receptor negative and so hormonal treatment .which is potentially teratogenic is not required . For women they have breast cancer, they should wait for 2 years before be pregnant as it is within this time that recurrence most often occurs.
Benign breast disorder:-
fibroadenoma :- this is usually arise in the fully developed breast between the age of 15-25 years although occasionally they occur in much older women .they arise from hyperplasia of single lobule and usually grow up to 2-3 cm in this case ,they surrounded by well marked capsule and can thus be enucleated through cosmetically appropriate incision. fibroadenoma does not require excision unless associated with suspicious cytology ,it becomes very large or the patient expressly desire the lump to be removed .Giant fibroadenoma occasionally occur during puberty they are over 5cm in diameters and are often rapidly growing but in other respects are similar to smaller fibroadenoma and can be enucleated through submammary incision .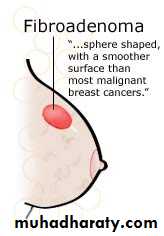
Phyllodes Tumors: these benign Tumors previously sometimes known as serocystic disease of Brodie or cystosacroma phyllodes, usually occur in women over the age of 40 years ,but can appear in younger women. They present as large, sometimes massive, tumor with unevenly bosselated surface, occasionally ulceration of over lying skin occurs because of pressure necrosis, despite their size they remain mobile on the chest wall.


Histologically there is a wide variation in their appearance with some of low malignant potential resembling a fibroadenoma and others having mitotic index which histologically worrying, the latter may recur locally but despite the name of cystosaroma phyllodes, they are rarely cystic and only very rarely develop features of sarcomatous Tumor . These may metastases via blood stream. Treatment for benign type is enucleation in young women or wide local excision. Massive Tumor, recurrent tumors and those of the malignant type will require mastectomy.
Galactocele: is rare, usually present as a solitary, subareolar cyst and always dates from lactation , it contain milk and in longstanding cases its wall tend to calcify .
Aberration of normal development and involution (ANDI)
Nomenclature: - the names are confusing. The name (ANDI) has been applied to this condition including fibrocystic disease, fibroadenosis, chronic mastitis and mastopathy.

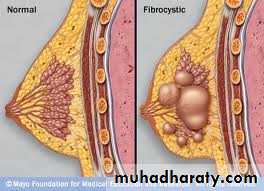
Etiology: - the breast is a dynamic structure that undergoes changes throughout a women's reproductive life and superimposed up on this , cyclical changes throughout the menstrual cycle, the pathogenesis of ANDI involve the disturbance in the breast physiology extending from perturbation of normality to well defined disease process. There is little correlation between the histological appearance of the breast and symptoms. Pathology of the breast consists essentially of four features that may vary in extent and degree in any one breast.
(1)Cyst formation (variable in size), (2) fibrosis: - fat and elastic tissue disappear and replaced with dense white fibrous trabeculae, the interstitial tissue is infiltrated with chronic inflammatory cell. (3) Hyperplasia of epithelium in the lining of the ducts and acini may occur with or without atypia. (4) Papillomatosis: - the epithelium hyperplasia may be so extensive that it results in papillomatous overgrowth within the ducts.
Clinical features:-the symptoms of ANDI are may as the term is used to encompass a wide range of benign conditions, but often include an area of lumpiness (seldom of discrete) and/or breast pain ( mastalgia )A benign discrete lump in the breast is commonly a cyst or fibroadenoma . The true lipoma occurs rarely. Lumpiness may be bilateral commonly in the upper outer quadrant or less commonly confined to one quadrant of the breast.
The changes may be cyclical with an increase in both lumpiness and often tenderness before menstrual period. Non cyclical mastalgia is more common in peri menopausal than post menopausal women. it should be distinguish from referred pain due to musculoskeletal disorder . Breast pain in post menopausal women not taking hormone replacement therapy is usually derived from the chest wall. About 5% of breast cancers exhibit pain at presentation.
Treatment of lumpy breast: - if the clinician is confident that she is not dealing with discrete abnormality and clinical confidence is supported by mammography and or ultrasound scanning if appropriate, then initially the women can be offered firm reassurance. It is worth while reviewing the patient at a different point in menstrual cycle for example 6 weeks after initial visit and often the clinical signs will have resolved by that time.
There is tendency for women with lumpy breasts to be rendered un necessarily anxious and to be submitted to multiple biopsies because the clinician lacks courage of lies or conviction. treatment of mastalgia :- Rx recommended of the pain interfere with women's life ,disturb her sleep and impair sexual activity ,initially firm reassurance that the symptoms are not associated with cancer will help the majority of the women . acknowledgement that this is a real symptom , non dismissive attitude and an explain of etiology are all helpful in managing the conditions .in first instance , an appropriately fitting and supportive bra should be worn throughout the day and a soft bra ( such as sports bra ) worn at night .
Avoiding caffeine drinks is said to be help. A patient symptoms diary helps her to chart the pattern of pain throughout the month and determine whether this is cyclical mastalgia. If these measures are not enough in treatment with evening primrose oil (it is Gammalinolenic acid metabolized to anti inflammatory prostaglandin) adequate dose given over 3 months will help more than half of these women, it appears to achieve higher response rates in those over 40 years of age rather than younger age. For those of intractable pain, antigonadotrophin drug such as danazol cap 200mg, or prolactin inhibitor (parlodel tab promocriptin) may be tried. Very rarely it is necessary to prescribe anti estrogen for example tamoxifin or LHRH agonist to deprive the breast epithelium of estrogenic derives. .
Duct ectasia :-( periductal mastitis): pathology. this is dilatation of the breast ducts which is often associate with periductal inflammation . the pathogenesis is obscure and almost certainly not uniform in all cases. Although the disease in much more common in smokers. it is dilatation in one or more of the larger lactiferous ducts which fill with a stagnant brown or greenish secretion , this may discharge .these fluids then set up an irritant reaction in surrounding tissue leading to periductal mastitis or even abscess and fistula formation.

In some cases a chronic indurations has forms .beneath the areola, which is mimes as carcinoma .fibrosis eventually develops which cause may slit like nipple retraction. Some believes it is anaerobic bacterial infection and smoking causing arteriopathy. Clinical features: nipple discharge of any color, subareolar mass, abscess, mammary duct fistula and nipple retraction are most common symptoms.
Treatment: in case of a mass or nipple retraction carcinoma must be excluded by obtaining mammography and negative cytology or histology. Any suspicion should be excised. Antibiotics should be tried co-amoxiclav or flucloxacillin and metronidazole. Surgery is often the only option likely to bring about cure of this condition; this consists of excision of all major ducts (Hadfield's operation). It is particularly important to shave the back of the nipple to ensure that all terminal ducts are removed, failure to do so will lead to recurrence.
Bacterial mastitis: it is the most common variety of mastitis and is associated with lactation in majority of the cases. Etiology: lactational mastitis is seen less frequently than previously. Most of the cases caused by staph, infective from the hospital or from infants who 50% of them harbor staph in their nasopharynx. Although ascending infection from a sore and cracked nipple may initiate mastitis, in many cases the lactiferous ducts will first become blocked by epithelial debris leading to stasis, this theory is supported by relatively high incidence of mastitis in women with a retracted nipple.

Once within ampulla of the duct, staph. cause clotting of the milk and with clot bacteria multiply. Clinical features: classical signs of acute inflammation (pain, fever, rigor, edema, erythema, tender swelling) and start as general cellulitis end by abscess formation. Treatment: during cellulitis stage patient should be treated by appropriate antibiotics as flucloxacillin or amoxiclav.
Feeding from the affected breast side may continue if the patient can do, local heat and analgesia will help to relieve pain. If an antibiotic is used in presence of undrained pus an antibioma may form. This is large, sterile, brawny edematous swelling that take many weeks to resolve.
It is used to recommended that the breast should be incised and drained if the infection did not resolve within 48 hours or if after being emptied of milk there was an area of tense indurations or other evidence of underlying abscess, this advice has been replaced with recommendation that repeated aspiration under antibiotics cover and ultrasound guide be performed. This often allows resolution without need foe incision scar and also allows carrying on breast feeding.pus should be sending for culture and sensitivity.
Breast abscess: if there is lactational abscess and marked skin thinning drainage can be done under local or general anesthesia. Drainage is done by opening all loculi by removing septi between loculi to make one room or loculi, with this procedure we ensure we draining the entire abscess.
Mondor's disease: it is superficial thrombophlibitis of superficial veins of the breast and anterior chest wall, it appears as subcutaneous cord. It should be distinguish from cancer permeation.

Congenital abnormalities of the breast: amazia: congenital absence of the breast on one or both sides, it might be associated with absence of pectorals major or absence of the nipple. Polymazia: accessory breast has been recorded in axilla most often, buttock and thigh.
Mastitis in infant: equal in boys and girls and usually in 3rd or 4th day of life, if pressed lightly a drop of colorless fluid can be expressed or milky secretion and usually disappear at 3rd week , this called witch's milk. It caused by stimulation of the fetal breast by prolactin in response to drop in maternal estrogen and it essentially physiological, mastitis usually due to staph. aurous.
Diseases of the nipple: absence of the nipple is rare and usually associated with amazia. Supernumerary nipples not un commonly occurs along a line extending from the anterior fold of the axilla to the fold of the groin this is called milk line.
Retraction of the nipple: this may be occurred at puberty or later in life in puberty is called simple nipple inversion and of unknown etiology. It might be bilateral in 25%, usually it cause problems with breast feeding and infection can occur specially during lactation, recent retraction of nipple may be of considerable pathological significance.
Discharge of the nipple; it can occur from one or more lactiferous ducts, management depends on the presence of lump and presence of blood in discharge from single duct. Mammography is done to exclude presence of underlying mass. Cytology is useful to exclude malignancy. a clear serous fluid means physiological in parous women, or it might associated with duct papilloma or mammary dysplasia.## blood stained discharge occurs in duct papilloma, duct carcinoma and in duct ectasia. Black or green secretion usually occurs in duct ectasia. Treatment: carcinoma should be excluded by occult blood and cytology. Surgical treatment of single duct is done by excision of the duct by microdecotomy, or multiple duct excision by core excision of major ducts.

Discharge from the nipple
------------------------------------------------------------------associated with lump no lump present
remove the lump localized to one duct from many ducts
Microdecotomy Hb+ve Hb-ve
over40 year under 40 years observe and repeat
core excision
discharge disappear
Locloised tone duct--microdectomy
Lump appears---lumpectomy
Gynecomastia: hypertrophy of a male breast, may be unilateral or bilateral. The breast enlarges at puberty and sometimes present the characteristic female breast causes
(1) Hormonal cause as in patient with carcinoma of prostate and treated by stilbestrol (now rarely used), in teratoma of the testis, anarchism, after castration, bronchial carcinoma, adrenal and pituitary disease and using of steroids in young body builder.
(2) associated with leprosy due to bilateral testicular atrophy.
(3) associated with liver failure as in cirrhosis due to failure of metabolism of estrogen.
(4) drugs as cemitidine, digoxine and spirenolactone.
(5) Klinefelter, s syndrome: sex chromosome anomaly has 47 XXY trisomy.
Treatment: reassurance, drugs as dostinix (antiprolactin), parlodel, or surgery by mastectomy with preservation of nipple and areola.