Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Objectives:
1.To identify the mechanisms of renal and ureteral injuries.
2. To know staging of renal injury.
3. To outline Management and complications of renal and ureteral injury.
About 10% of all injuries in ER.
Early diagnosis is essential.
Initial resuscitation includes: A,B,C&D, iv line, and catheterization.
History: full description of the trauma,
In gunshots: type, caliber, mass& velocity.
Clinical examination:
Special examination:
1. Catheterization
2. EXU
3. Cystography
4. Urethrography
5. Arteriography
6. CT scan
7. Cystoscopy
8. Abd US

Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Catheterization
Should never be attempted if blood at EUM
If so do retrograde urethrography
If no blood do careful catheterization to recover urine for exam., evacuate
the bladder, and monitor UOP.
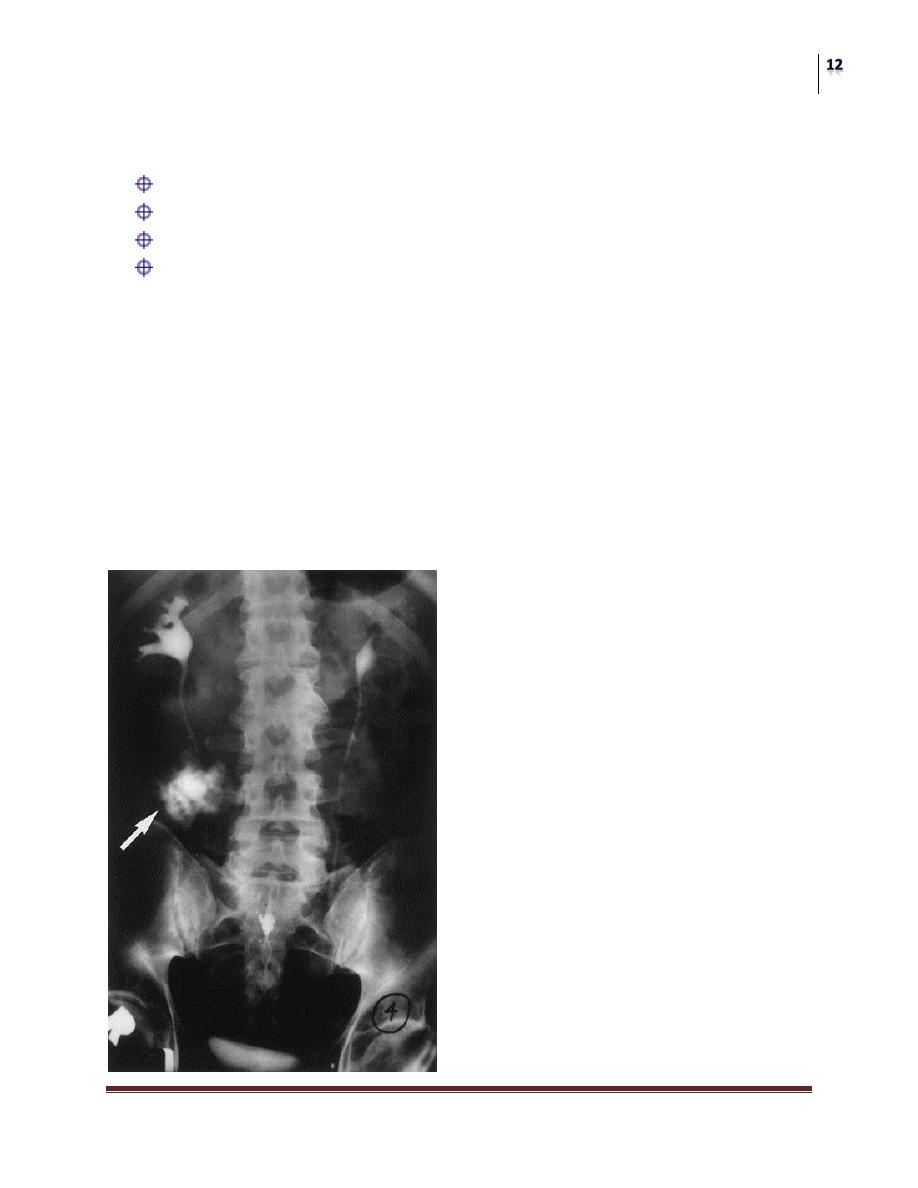
EXU
Done immediately after iv line has been established, and resuscitation has
begun, using 2ml/kg of contrast material injected iv, and multiple x-ray films
are taken
Cystography
Direct/Indirect
Full/evacuation films
Urethrography
12 F cath.
3ml balloon
15-20 ml contrast
Arteriography
define renal vascular and parenchymal injury
Therapeutic : to define and embolize bleeding vessels specially in pelvis
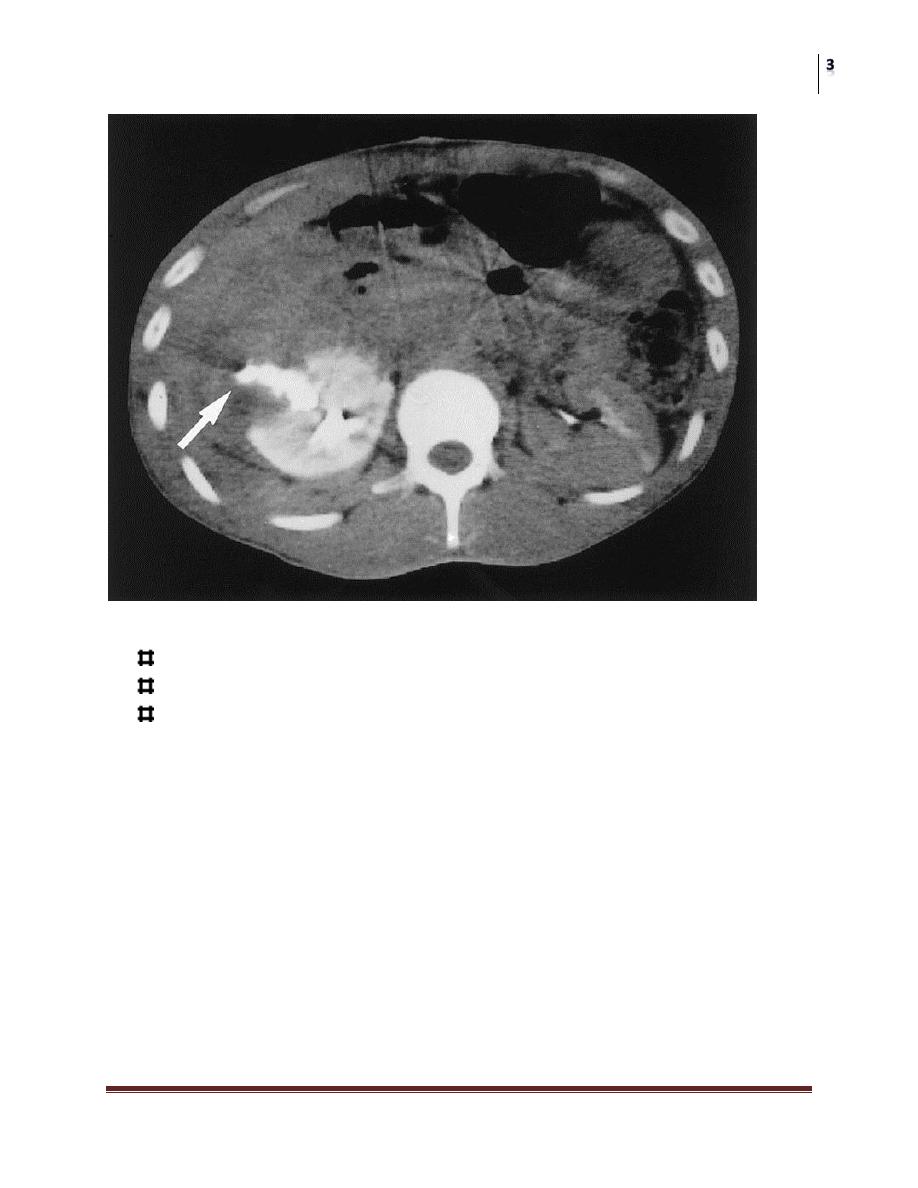
CT scan
Is the definitive study and gold standard in renal injury management
It is helpful in:
Assessing the size and extent of perirenal, and retroperitoneal hematoma
assessing renal parenchymal injury
Identifying non-viable tissues
Defining urine extravasation
Assessing other abd. Organ injuries.
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
INJURIES TO THE KIDNEY
The most common organ injury in GUT.
Fractured ribs and vertebral transverse processes should alert the surgeon.
Usually associated with other organ injury in multiply injured patients.
Etiology
Blunt injury in 85%.
Rapid deceleration injury may avulse the renal vessels.
Other organ injury are present in 80% of cases
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Fructured lower ribs should alert us about kidney injury
Pathology
A) early pathological changes:
1. Minor renal trauma (85%):
contusion or bruising of parenchyma
sub capsular hematoma
superficial cortical laceration
Very rarely needs surgical exploration
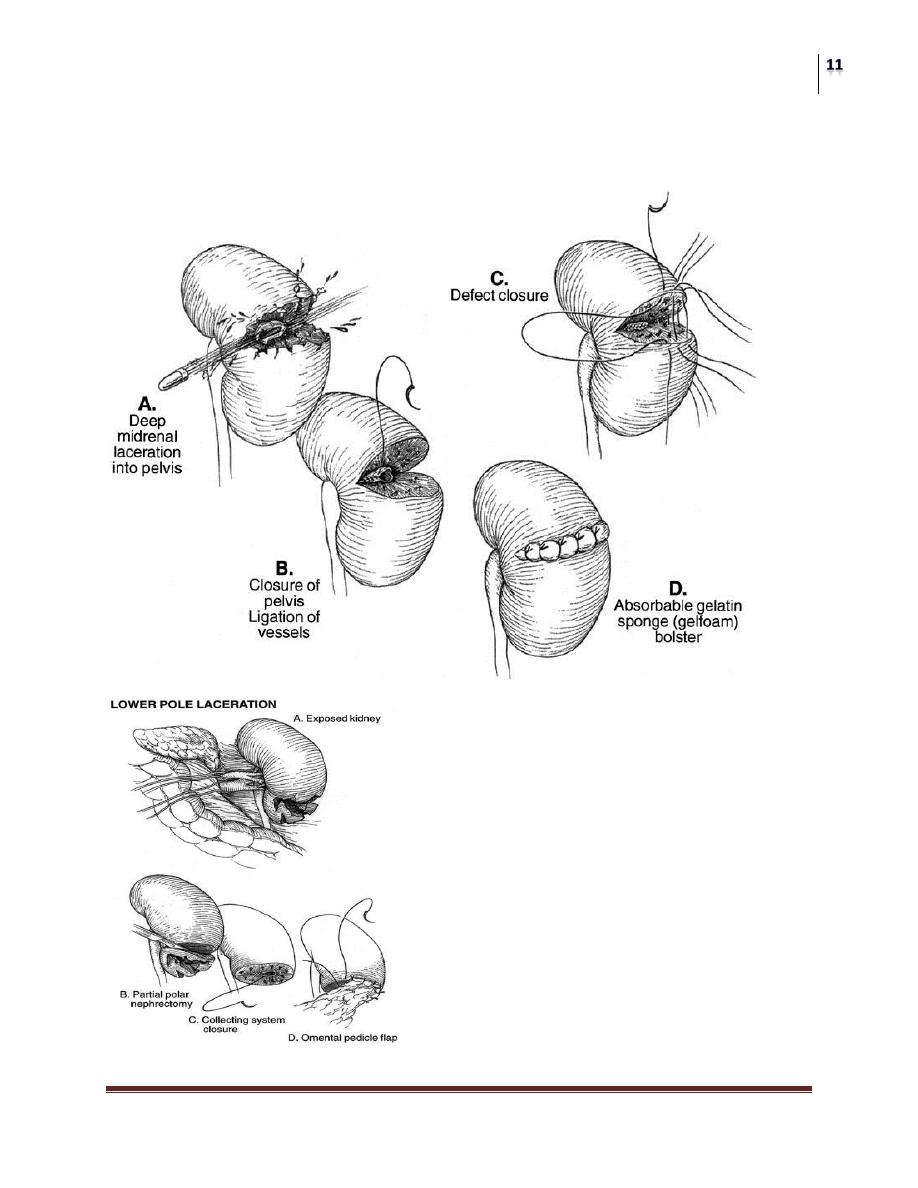
2. Major renal trauma (15%)
Deep corticomedullary laceration which may extend into the collecting system
causing urine extravasation into the perirenal space, in multiple may cause
complete destruction of the kidney
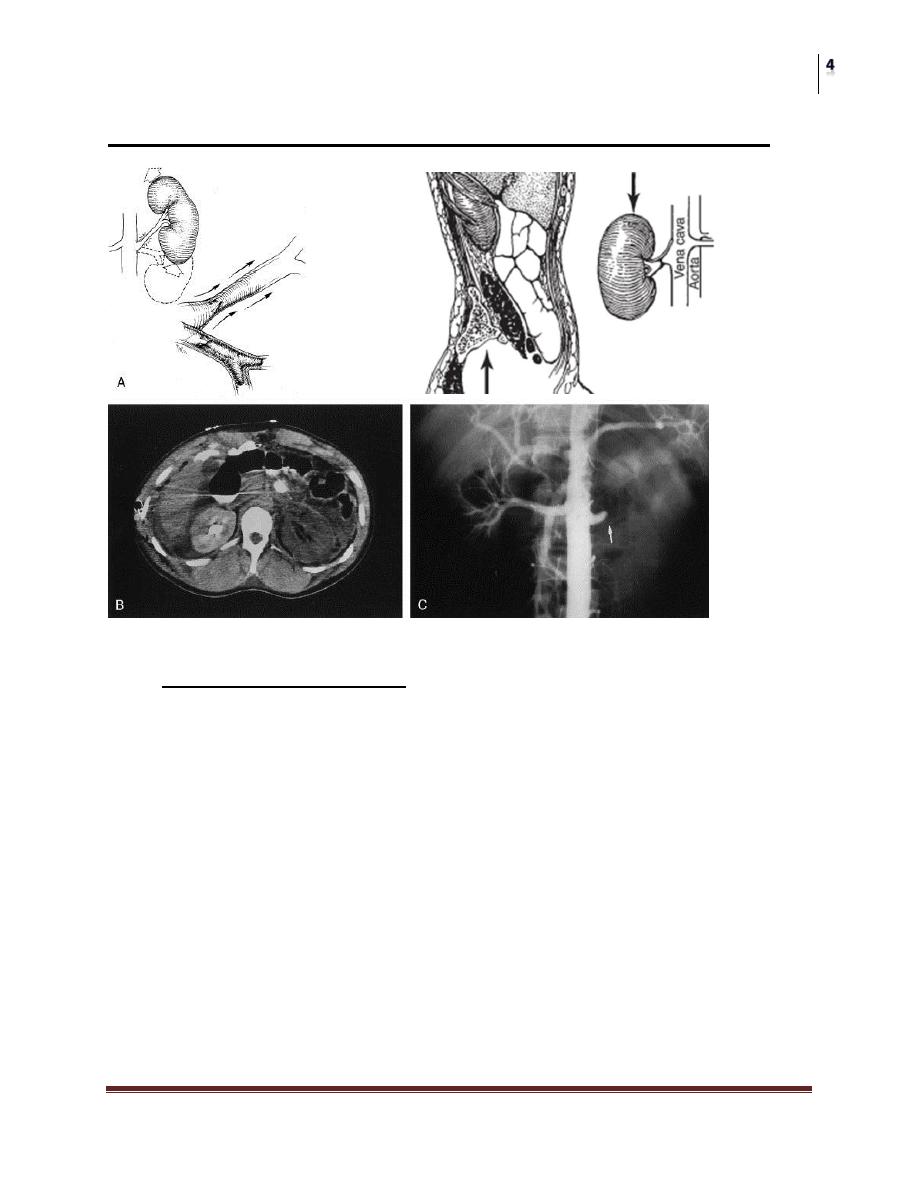
3. Vascular injury (1%)
In rapid deceleration injury the kidney moves up and down causing stretching of
the renal pedicle, avulsion (complete, or partial)
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Intimal tear may occur causing thrombosis
They are usually difficult to diagnose and result in total destruction of the kidney
B) Late pathological changes
1. Urinoma: tear extending into collecting system leading to urinary
extravasation and formation of large perirenal mass, that can lead to HN, and
abscess formation.
2. Hydronephrosis: urinoma compression, or healing by fibrosis can cause
stircture and HN.
3. AV fistulae: specially occurs following penetrating injuries and surgical
intervention.
4. Renal vascular hypertension: occurs in about 1% of cases.
Clinical Features
Symptoms:
Hematuria: microscopic/ gross
degree does not correspond to severity of injury
In some cases of renal vascular injury, hematuria may be absent
specially in deceleration inj.
Pain: over the flank or all over the abd.
Features of other abd org. injury,or shock, or peritoneal irritation.
Degree of Haematuria does not refleclt the severity of renal injury.
signs:
shock and features of blood loss
flank echymosis
lower rib or vertebral fracture
diffuse abd tenderness, and acute abd.
large mass representing hematoma or urinoma
abd distension and absent bowel sounds
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
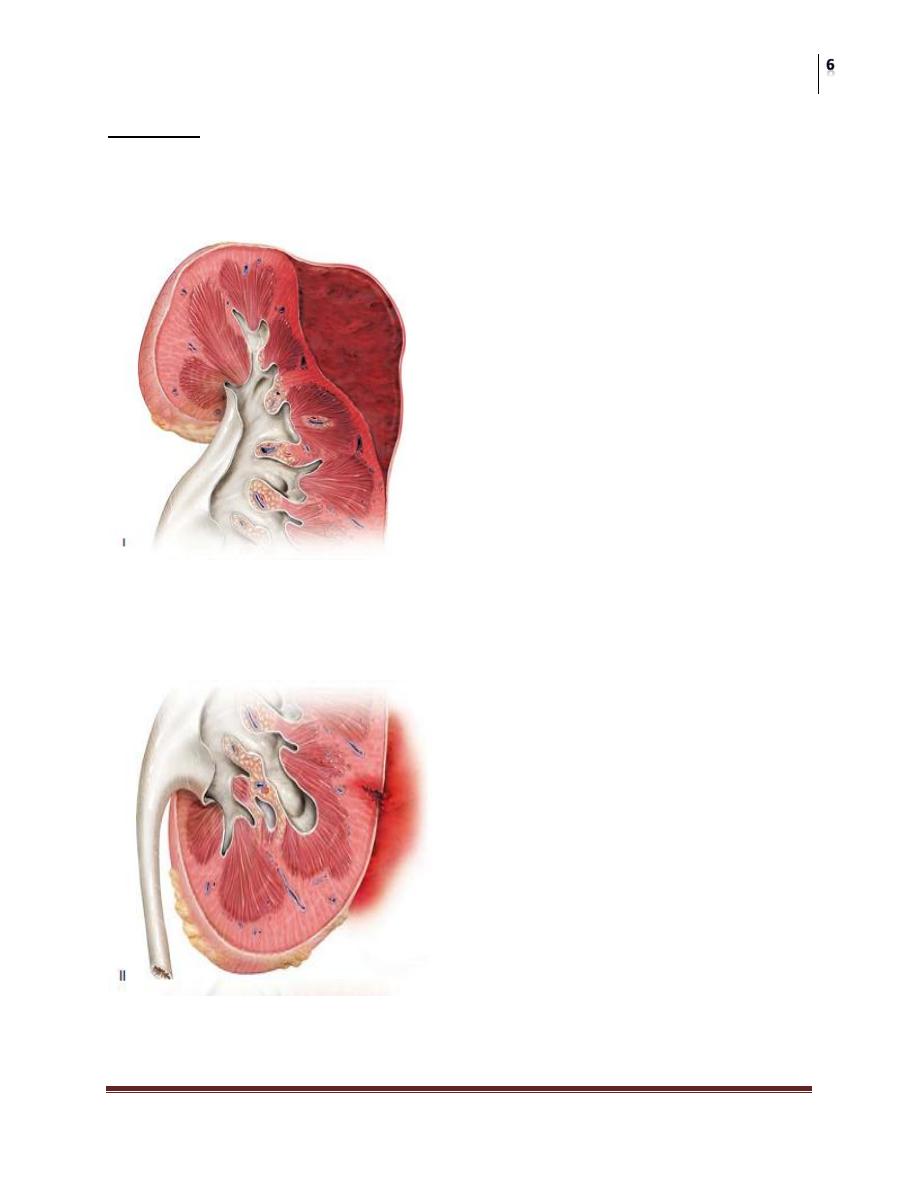
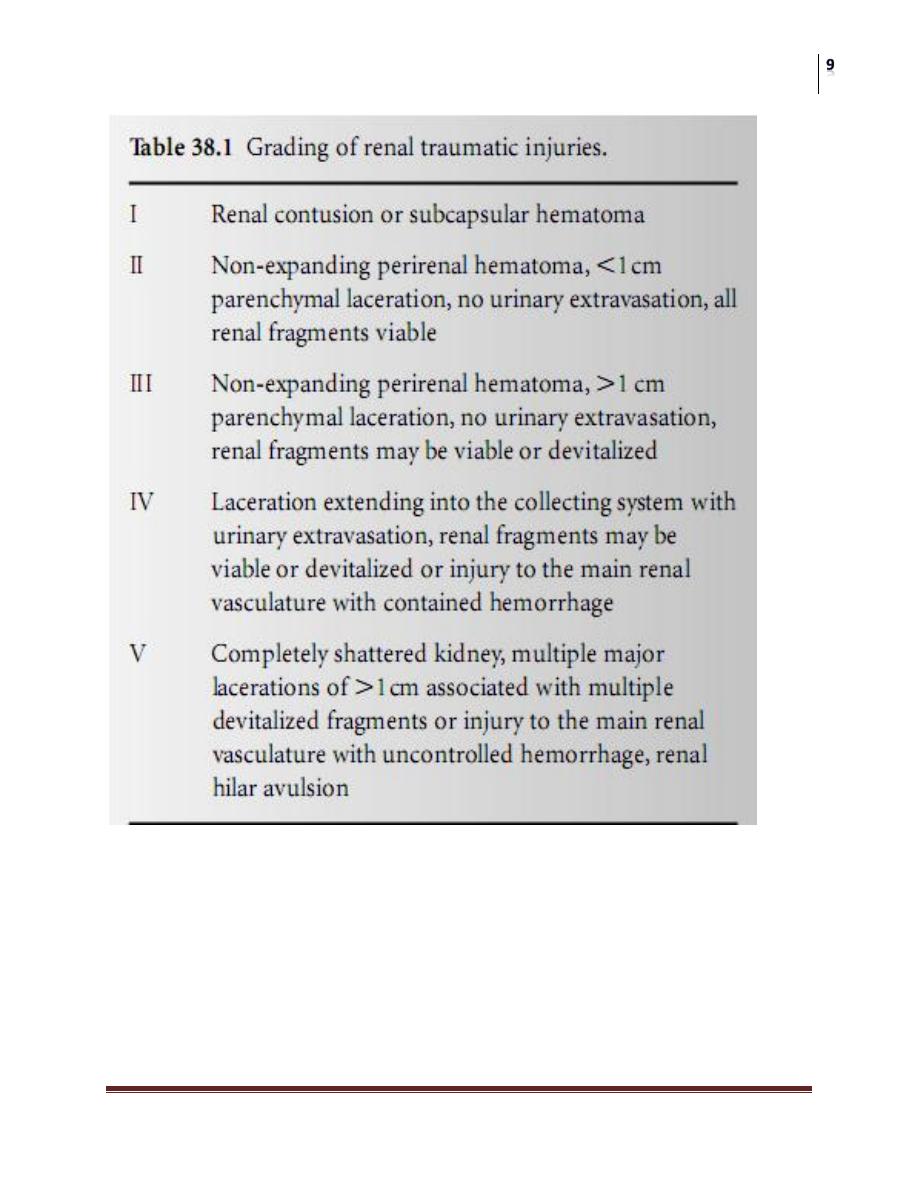
STAGING
staging ideally starts with CT scan, the most effective and accurate method
of diagnosis
us and cystoscopy are of little use in initial assessment
Stage 1
Renal contusion
subcapsular hematoma
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Stage 2
Non-expanding perirenal heamtoma
less than 1 cm parenchymal tear, no urine extravasation
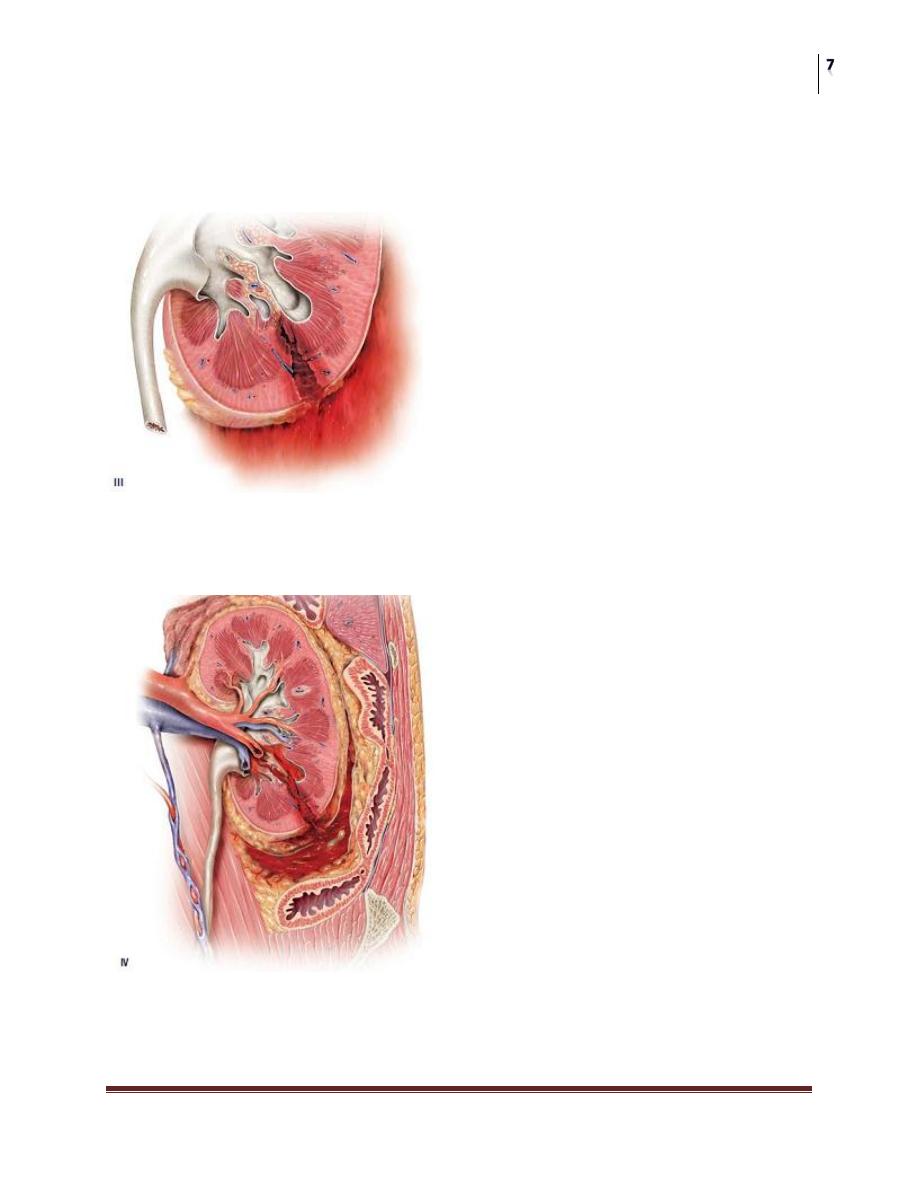
Stage 3
Non-expanding perirenal heamtoma
parenchymal tear more than 1cm but not involving the collecting system
Stage 4
Parenchymal tear extending into the collecting system with urinary
extravasation
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
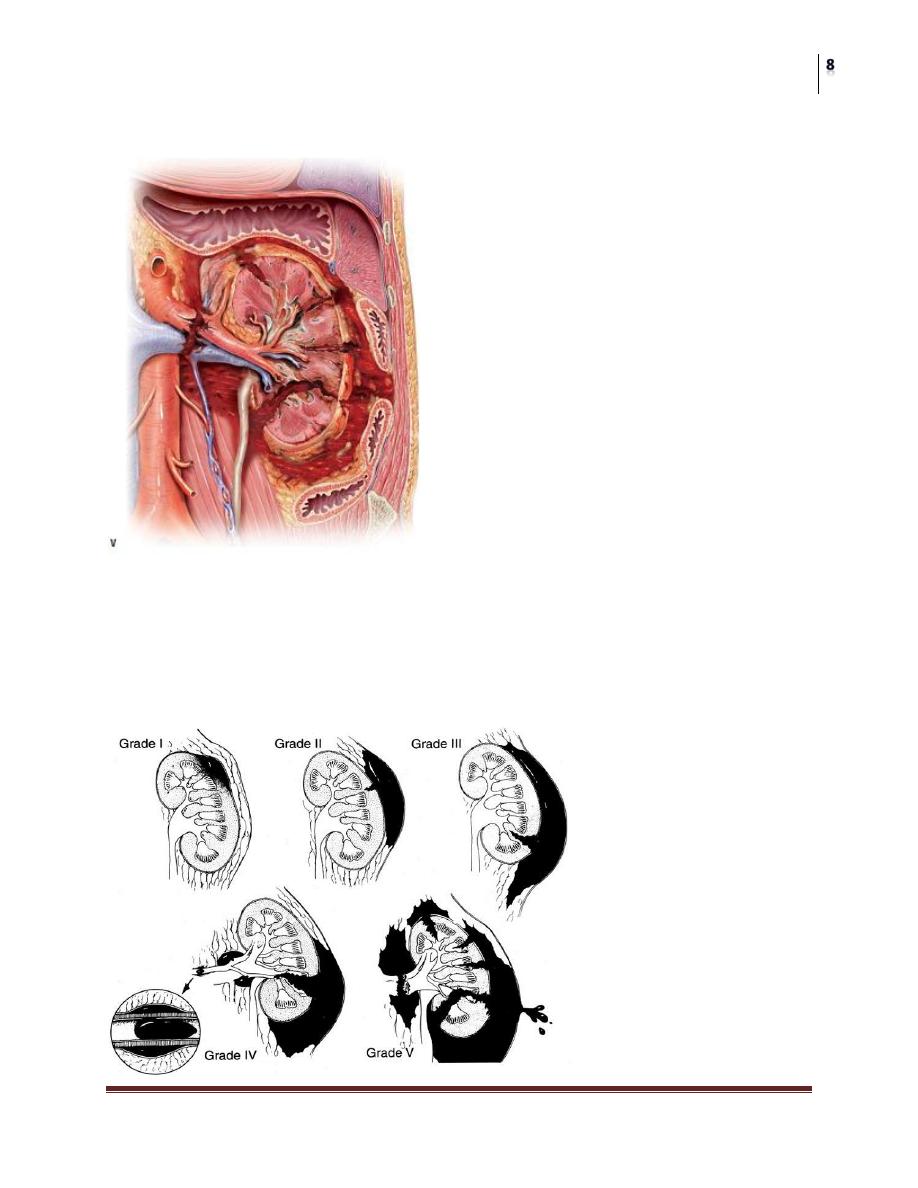
main renal vascular injury with controlled hemorrhage
Stage 5
Completely shuttered kidney
Multiple major laceration with devitalized tissue
Main renal vascular hemorrhage with uncontrolled hemorrhage
Hilar avulsion
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Indication for Full Imaging and Staging
frank hematuria
microscopic hematuria with shock
deceleration injury
suspected other abd organ injury as liver
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Non-visualized kidney on imaging
total pedicle avulsion
arterial thrombosis
severe contusion causing vascular spasm
absent kidney (cong. or surgically removed)
COMPLICATIONS
EARLY COMPLICATIONS:
bleeding: is the most important and should be monitored carefully and
treated vigorously
urinary extravasation “urinoma” prone to infection and abscess formation
LATE COMPLICATIONS:
hypertension
hydronephrosis
AV fistula
calculus formation
renal atrophy
TREATMENT
Emergency measures:
this includes resuscitation, treating shock, as well as staging the injury
Blunt injury:
In 85% bleeding stops spontaneously with bed rest, antibiotics, and good hydration
Indications of Surgical Exploration
persistent or expanding hematoma
big urinary extravasation
evidence of non-viable parenchyma
renal pedicle injury
Failed conservative management
Penetrating injury
Usually treated surgically unless complete staging shows a minor parenchymal
laceration with no urine extravasation
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Treatment of complications
urinoma, abscess, hypertension, hydronephrosis, calculi
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
INJURIES TO THE URETER
They are rare but may occur, etiology includes:
Difficult pelvic and abd surgery
Penetrating injury
Endoscopic manipulation
Devascularization during LN dissection
Pathology
Ureter may be:
Ligated leading to HN and renal damage
Cut: urine extravasation
Extraperitoneal: sepsis, ureterovag, or cut fistulae
intraperitoneal: peritonitis, and sepsis
Devascularized:
sloughing, and urine leak
Healing by fibrosis and stricture formation
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Clinical Findings
Fever >38.3 °C
Flank and lower quadrant pain
Paralytic ileus, nausea, vomiting
Fistulae: cutaneous or vag.
If bilateral causes anuria
Signs of peritonitis
GUE shows hematuria in 90% of cases
Diagnosis
At time of injury, during surgery, is the best opportunity for treatment.
U/S is helpful in early post-operative period.
EXU and CT are the best to show either urinary leak or stricture and HN.
Retrograde uretrography helps to define the exact site of injury and planning
managent
Dif. Diag: includes post-operative peritonitis and bowel obstruction
Complications:
Stricture formation and HN
Urine extravasation and urinoma formation
Pyelonephritis
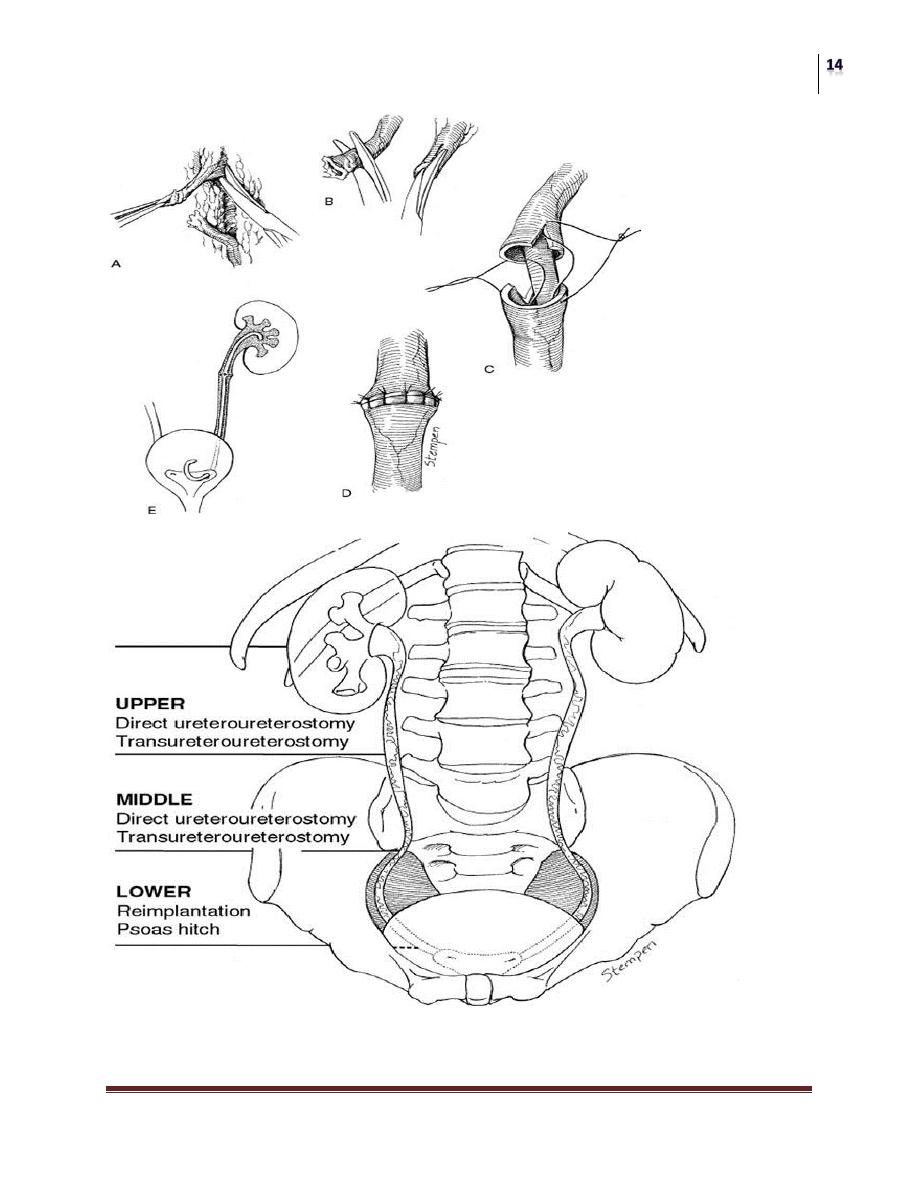
Treatment
If discovered at surgery, immediate repair is done
If discovered late and the patient has complications, do proximal urinary
diversion by nephrostomy (formal, or percut) and manage the injury later
Principles of repair are:
Remove all fibrosed tissues
Tension free
Spatulation
Water tight
Ureteral stenting
Retroperitoneal drainage
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
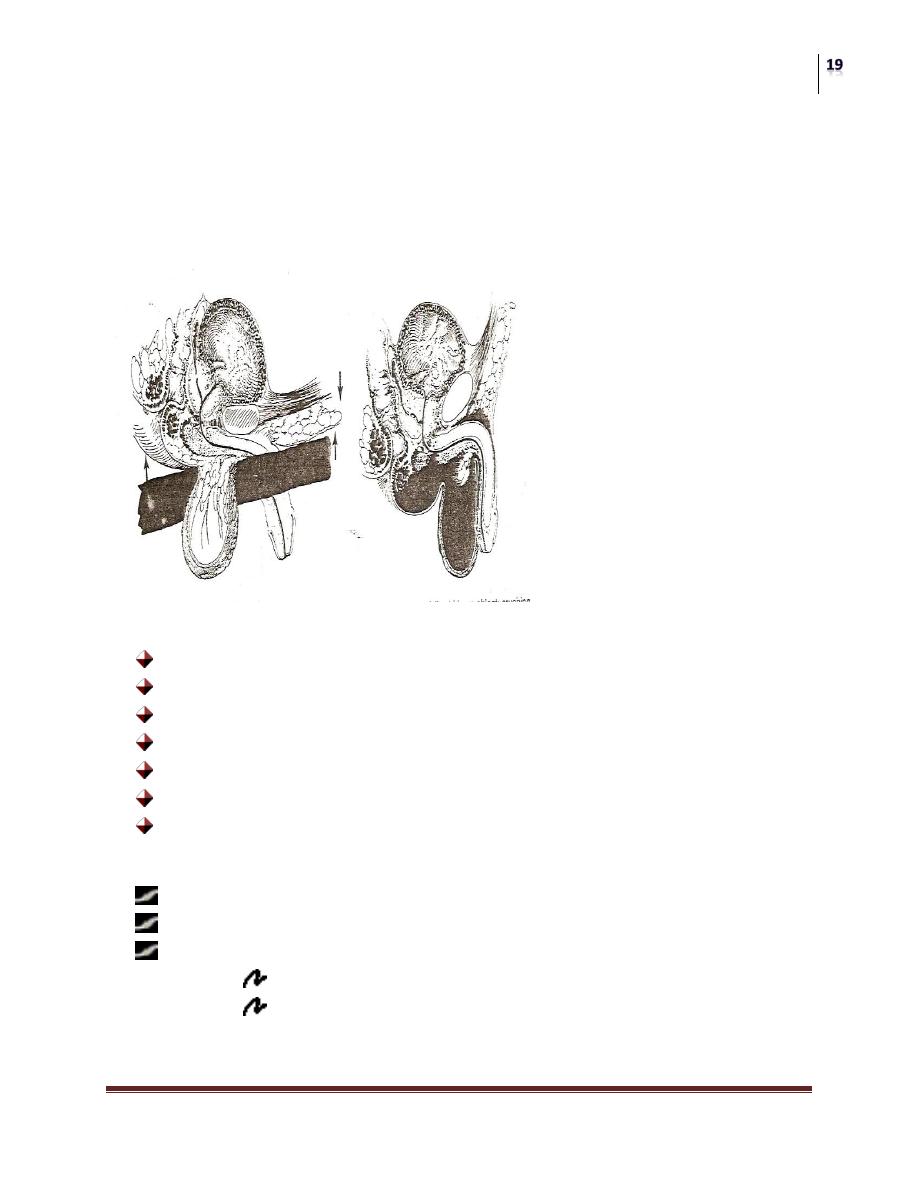
INJURIES TO THE BLADDER
Occurs most often due to external force or pelvic fracture
About 15% of all pelvic fractures are associated with bladder injury
90% of bladder ruptures are associated with pelvic fracture
Pathology
Sharp bony chips can penetrate the bladder causing usually extraperitoneal
rupture
Blunt lower abd trauma to distended bladder may result in bladder disruption
usually intraperitoneal
Extravasated urine may become infected causing abscess formation or
peritonitis
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Clinical Features
History of trauma
Patient is unable to urinate
Hematuria usually gross
Suprapubic tenderness, or mass
Associated inj: wound, fracture, shock…etc
Keep in mind:
Look for blood at EUM
On DRE marks may be indistinct because of the large pelvic hematoma
X ray Findings
Plain:
o Evidence of pelvic fracture
o Lower abd haziness due to blood or urine accumulation
Cystogram:
o Shows the urinary leak site and degree
o Technique: full under gravity, 300 mls., and allow to drain.
CT cystogram:
Excellent method for diagnosis
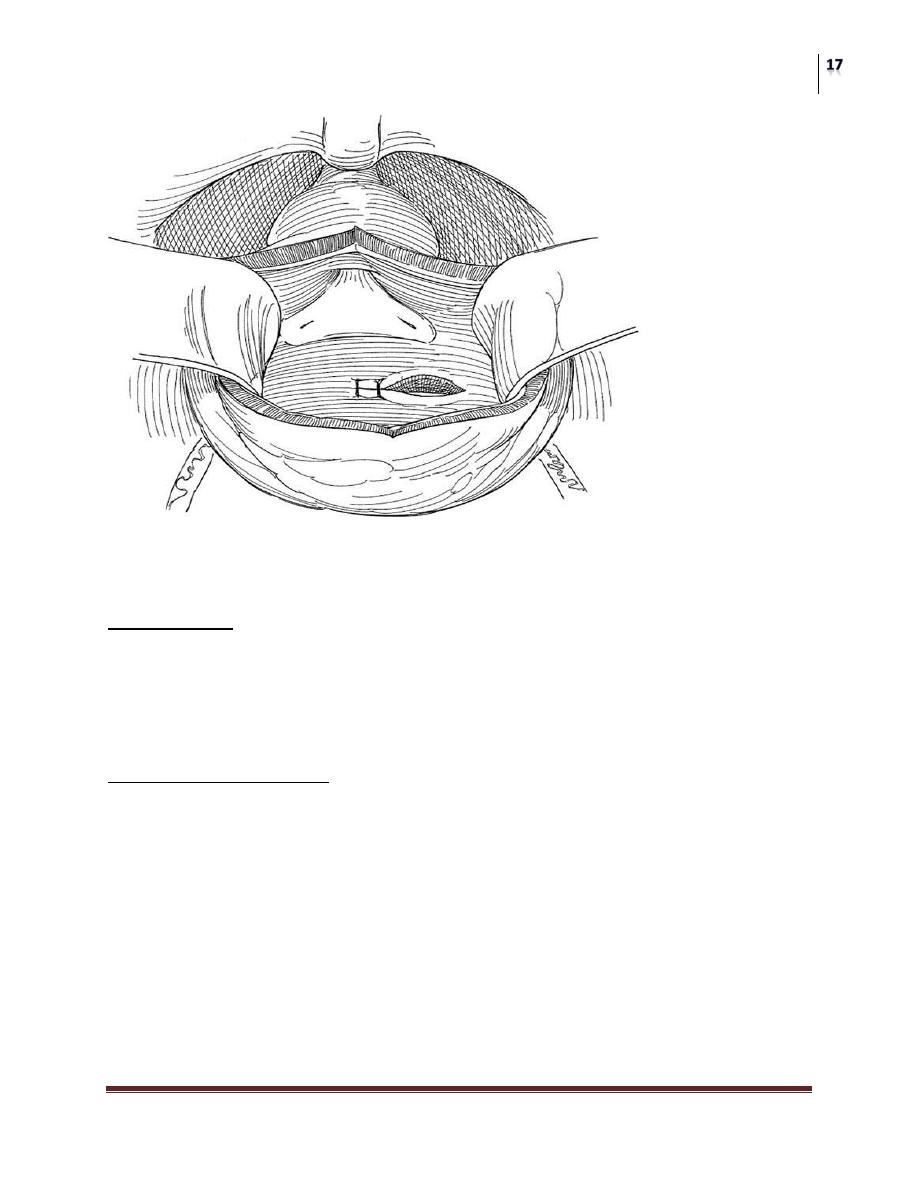
Treatment
A) Emergency measures: treat shock, and other vital organ injuries
B) Surgical repair:
Bladder should be carefully explored and searched for multiple
penetrations specially in association with pelvic fractures
All penetrations should be sutured water tight with absorbable
material
Trigon and bladder neck should be repaired meticulously
Bladder should be drained via urethral and suprapubic catheters
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
However a small extraperitoneal rupture may be treated conservatively by urethral
cath.
Complications:
Pelvic abscess formation
Peritonitis
Partial incontinence
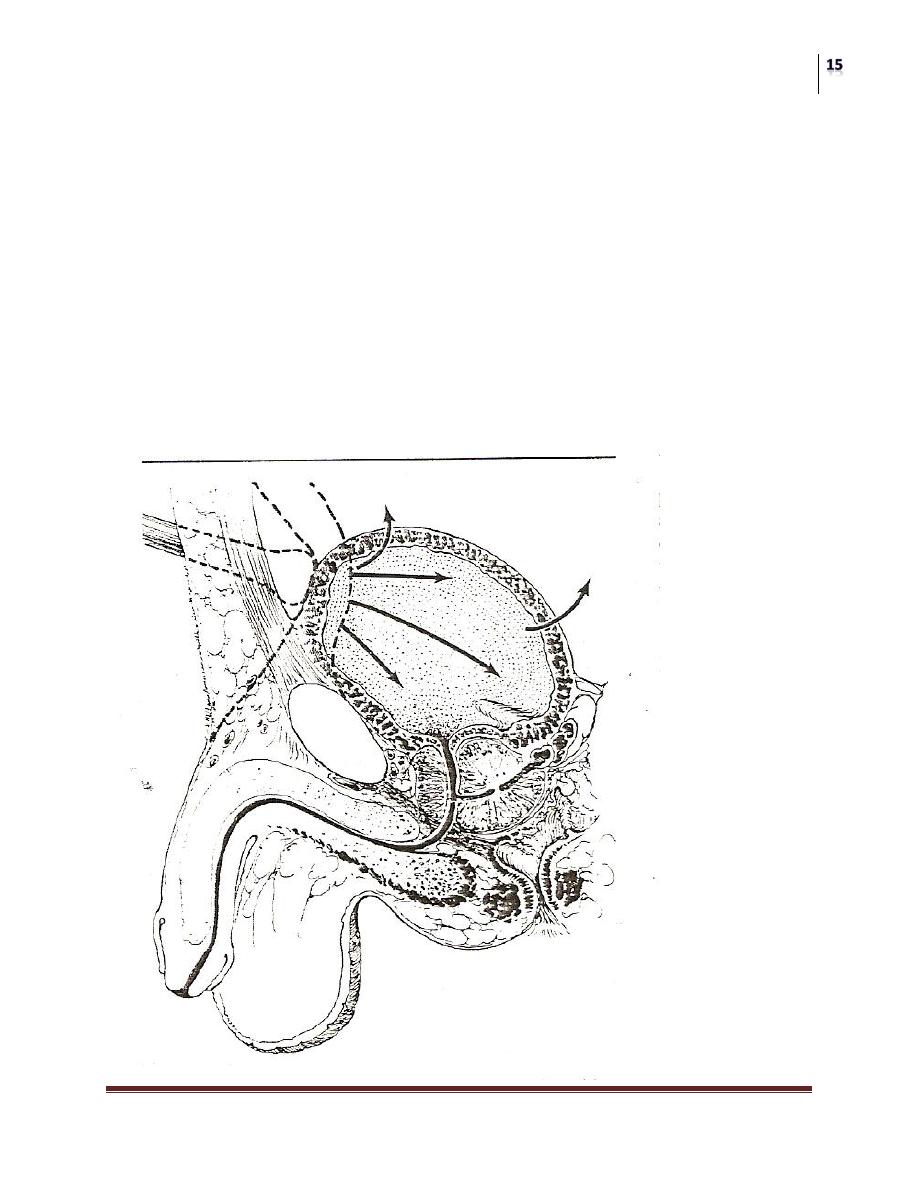
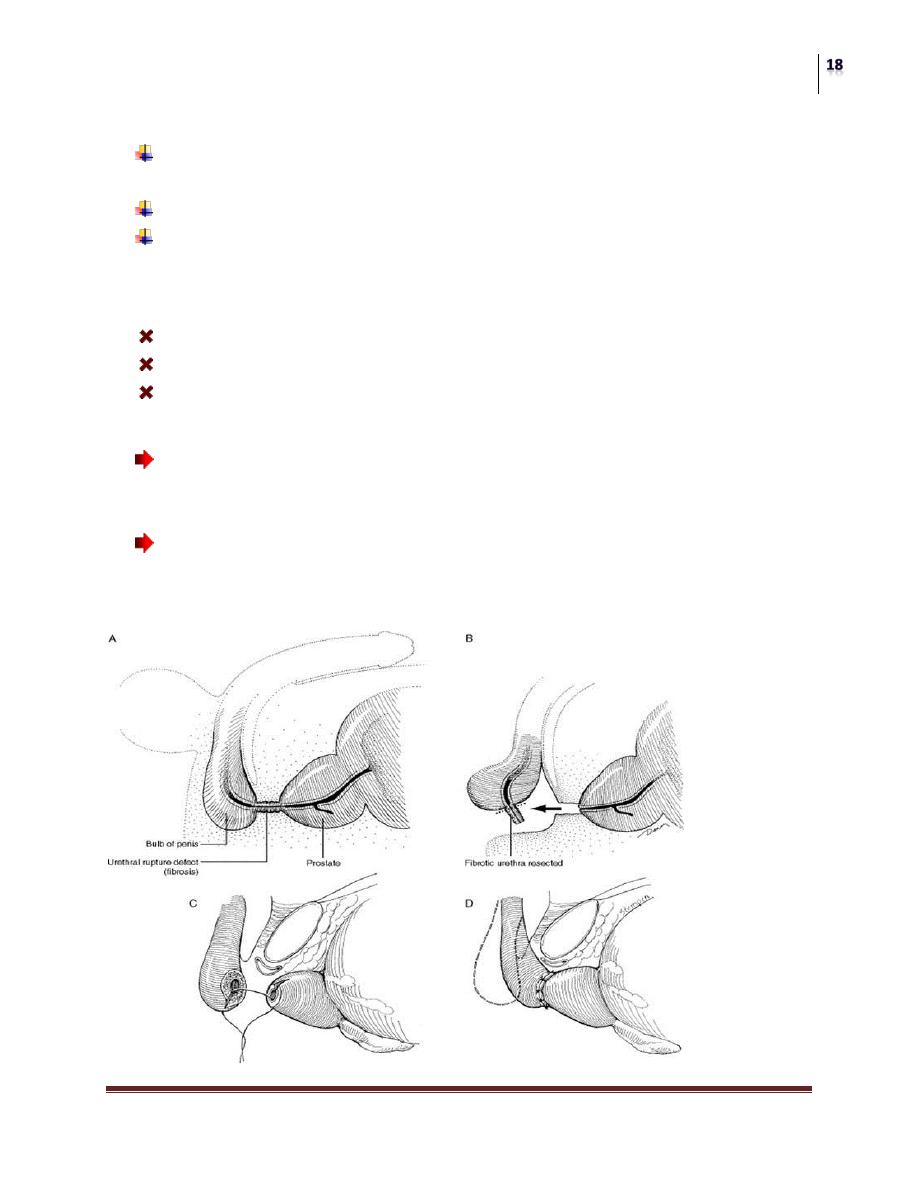
URETHRAL INJURIES
Posterior urethral injuries:
The membranous urethra is sheared from the prostatic apex at the prostato -
membranous junction
It usually accompanies pelvic fractures
The prostate is displaced superiorly
Extravasation is periprostatic and perivesical
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Clinical Features
Blood at the EUM: never attempt catheterization, or you may introduce
infection or make an incomplete rupture a complete one, instead do RUG
DRE may be misleading because a big hematoma may feel like a prostate
Don’t let the patient void until full evaluation,and look for associated
bladder injury.
Complicatoins
Stricture
Incontinence
Impotence
Treatment
Once a urethral rupture is diagnosed it is better to avoid immediate repair
because of the high risk of complications, instead do formal suprapubic
cystostomy.
Urethral reconstruction can be done after 3 months, by removal of all
fibrosed tissue and end to end anastamosis, with or without buccal mucosal
graft
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Anterior Urethral Injuries
Usually caused by a direct trauma as straddle injuries or falling astride
But it may follow urethral instrumentation
These may cause contusion or laceration
Extravasated urine is enclosed within colle’s fascia
Clinical features
History of trauma
Blood at the EUM
Tender perineum with or without swelling
DRE normal
Patient has desire to urinate, never allow!
Don’t try cath.
Diagnosis made by RUG
TREATMENT
If no extravasation, simple contusion, a trial of gentle cath may be done
If laceration and extravasation, do percut suprapubic cystostomy
After 2-3 weeks do voiding study and assess the urethra
Normal
Stricture optical urethrotomy
Surgery
Injuries to the GUT
Dr. Ismaeel
Lec. 35
Complications
Bleeding , may be heavy, so apply pressure to perineum preferably with ice
Abscess formation
Stricture formation