Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
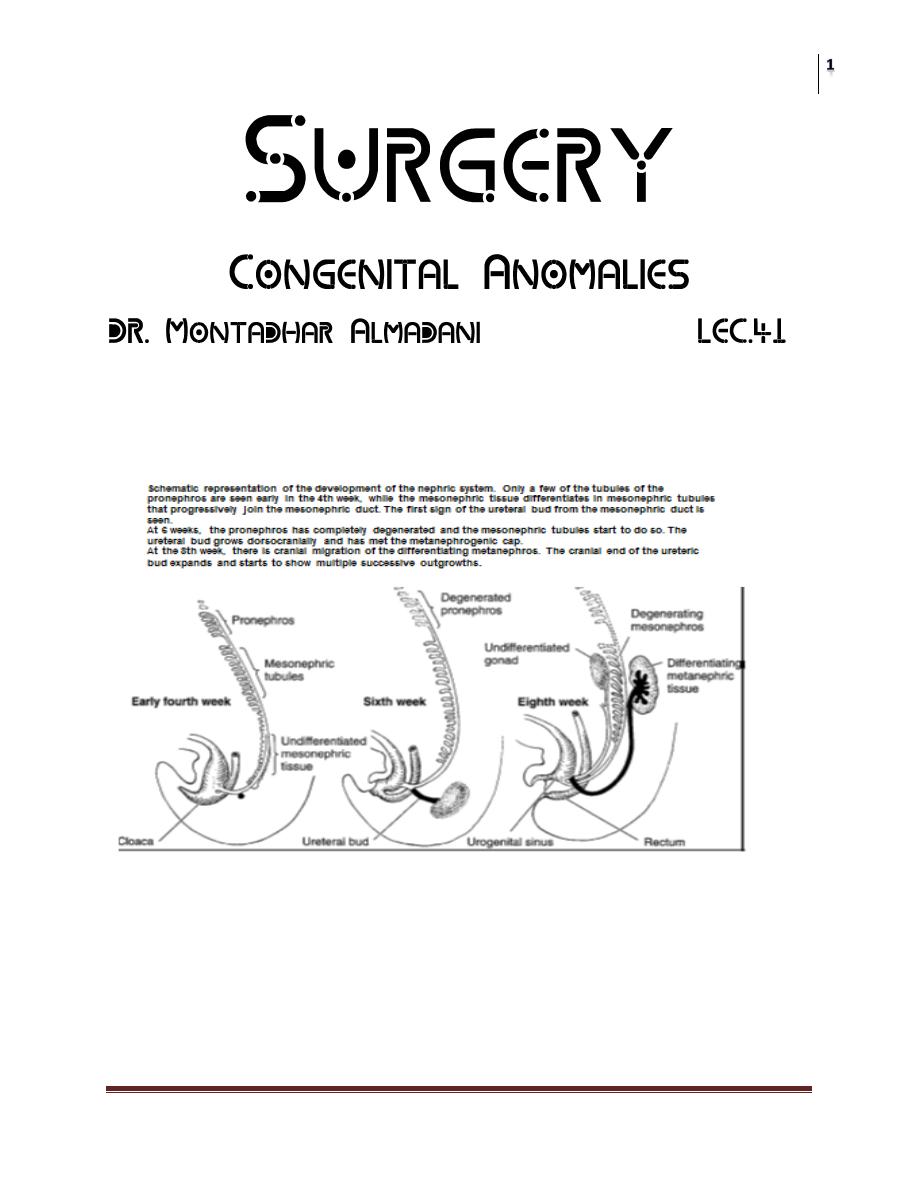
I. UPPER URINARY TRACT
A. Abnormalities of the Kidney Position and Number
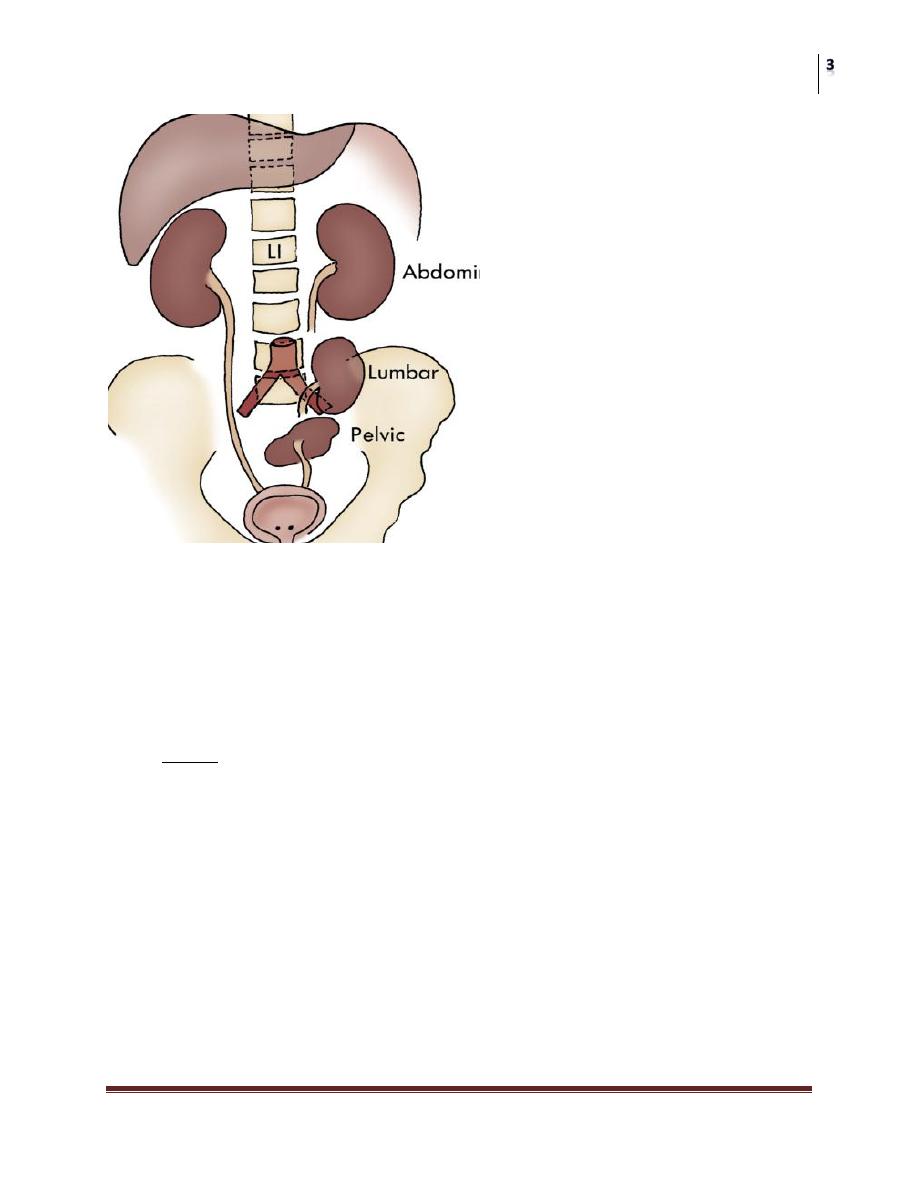
1. Simple ectopia
Incidence is approximately 1 per 900 Associated findings include small size with
persistent fetal lobations, anterior or horizontal pelvis, anomalous vasculature,
contralateral agenesis, vesicoureteral reflux, Mu¨llerian anomalies in 20–60% of
females; undescended testes, hypospadias. Only workup, ultrasound, voiding
cystourethrography.
Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
2. Thoracic ectopia.
Comprises less than 5% of ectopic kidneys. Origin is delayed closure of
diaphragmatic angle versus ‘‘overshoot’’ of renal ascent.
Adrenal may or may not be thoracic.
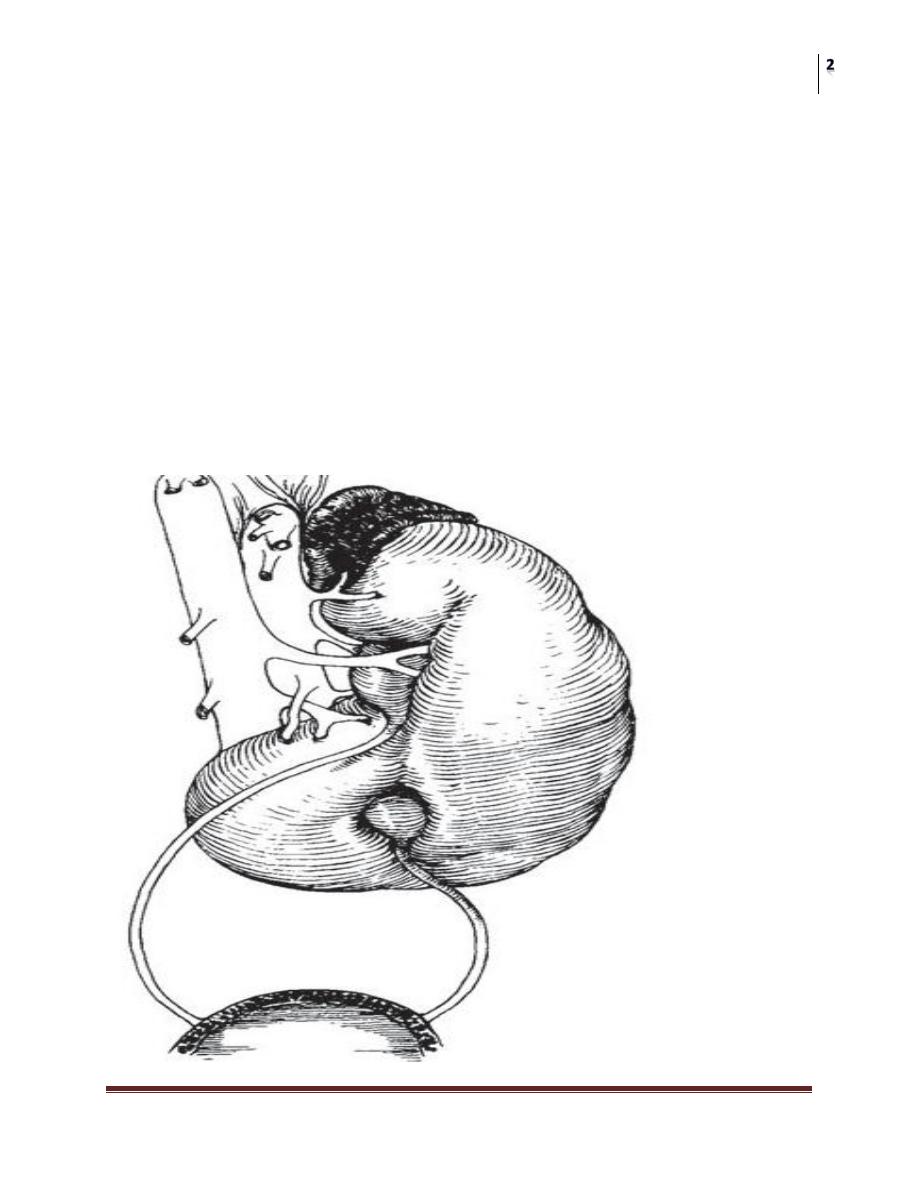
3. Crossed ectopia and fusion (Bauer).
Incidence is 1 per 1000 to 1 per 2000; 90% crossed with fusion; 2:1 male,
3:1 left crossed; 24 cases solitary, five cases bilateral reported to date.
Origin from abnormal migration of ureteral bud or rotation of caudal end of
fetus at time of bud formation
• Crossed renal ectopy with fusion. The renal mass lies in the
left flank. The right ureter must cross over the midline.
Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
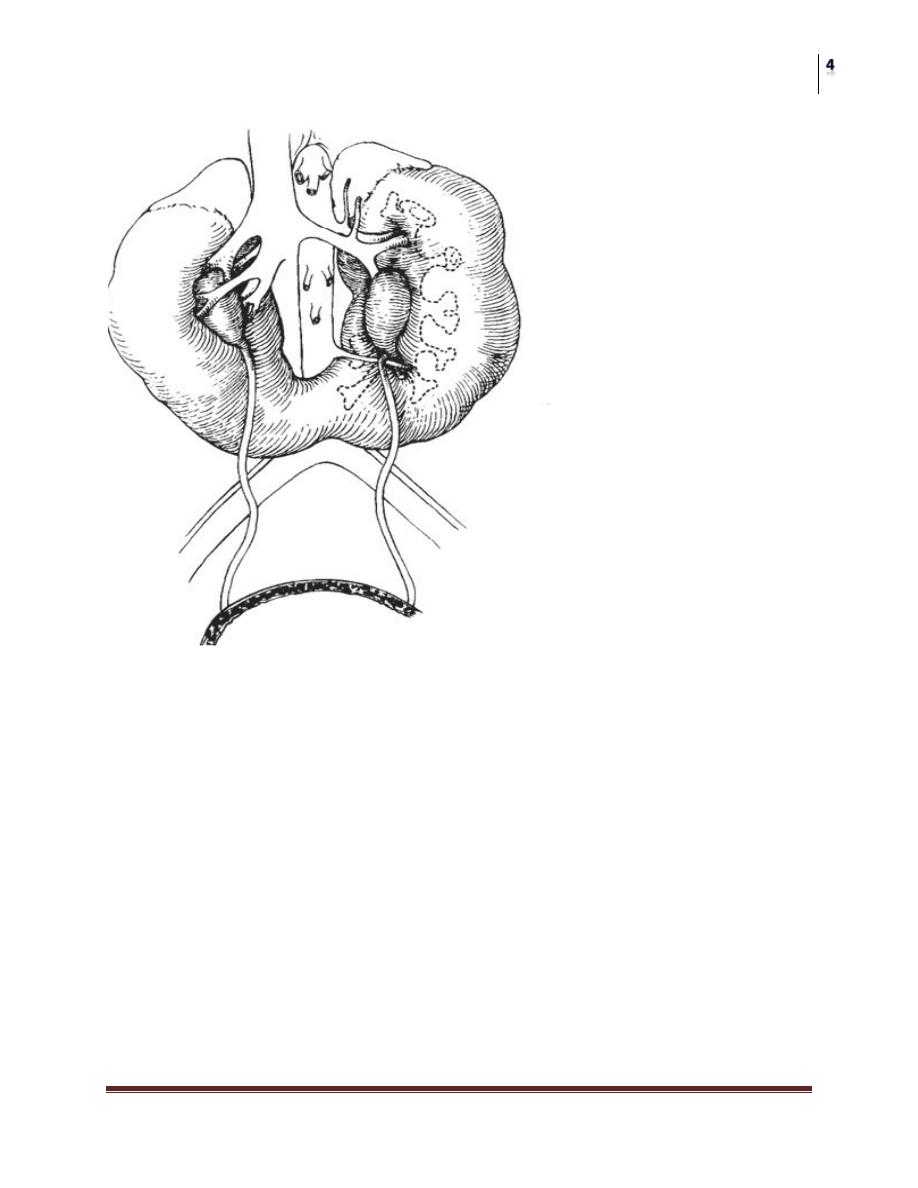
4. Horseshoe kidney.
Incidence is 1 per 400 ; 2:1 males.
Origin is fusion of lower poles before or during rotation (4½ to 6 weeks’
gestation).
Stones; infection may result from stasis
• NOTE
• Pelves are anterior.
• Note the aberrant artery obstructing the left ureter and the low position of
renal mass.
• CT clearly outlines the renal mass
Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
Treatment
No treatment is necessary unless obstruction or infection is present. Drainage of a
horseshoe kidney may be improved by dividing its isthmus. If one pole of a
horseshoe is badly damaged, it may require surgical resection.
5. Bilateral renal agenesis.
Incidence is 1 per 4800 births or 1 per 400 newborn autopsies (75% are
male) and typically lethal.
Origin either ureteral bud failure or absence of the nephrogenic ridge.
Associated findings include absent renal arteries, complete ureteral atresia in
50%, bladder atresia in 50%,
Potter’s syndrome

Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
typical Potter's facial appearance
6. Unilateral renal agenesis.
a) Incidence is 1 per 1100 in autopsy series
b) Origin is probably ureteral bud failure; there is a familial trend.
c) Associated findings include absent ureter with hemitrigone (50%), adrenal
agenesis (10%), genital anomalies (20–40% in both sexes).
7. Supernumerary kidney.
a) Incidence is unknown.
b) Origin a combined defect of ureteral bud and metanephros.
c) Associated findings are hydronephrosis (50%),
A.
Cystic Abnormalities of the Kidney
1. Autosomal dominant polycystic kidney disease.
a) Chromosome 16 and chromosome 4.
b) Autosomal dominant transmission.
c) Adult type is the most common cystic disease in humans, with an incidence
of 1 per 1250 live births and accounts for 10% of all end-stage renal disease.

Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
d) Usually presents after between 30 and 50 years with pain, hematuria, and
progressive renal insufficiency
e) Intravenous urography (IVU) reveals irregular renal enlargement with
calyceal distortion; ultrasound shows multiple cysts of variable sizes.
f) Associated findings are liver cysts without functional impairment in one
third of patients and berry aneurysms in 10–40%.
g) Complications include uremia, hypertension, myocardial infarction, and
intracranial hemorrhage (9%).
h) Management involves control of blood pressure and urinary infection, relief
of cardiac failure, and eventually dialysis or transplantation.
2. Autosomal recessive polycystic kidney disease.
a) Chromosome 6.
b) Infantile type. Rare (1 per 10,000 live births), usually presents with bilateral
flank masses in infancy but can present in childhood with renal or hepatic
insufficiency.
IVU shows huge (12–16 times normal) kidneys with a pronouncedly delayed
nephrogram and characteristic streaked appearance (‘‘sunburst’’ pattern).
c) Associated findings are congenital hepatic (periportal)
Fibrosis
Complications are renal and hepatic failure, hypertension, and respiratory
compromise in the newborn; patients usually die within the first 2 months of life.
B. Ureteral Anomalies
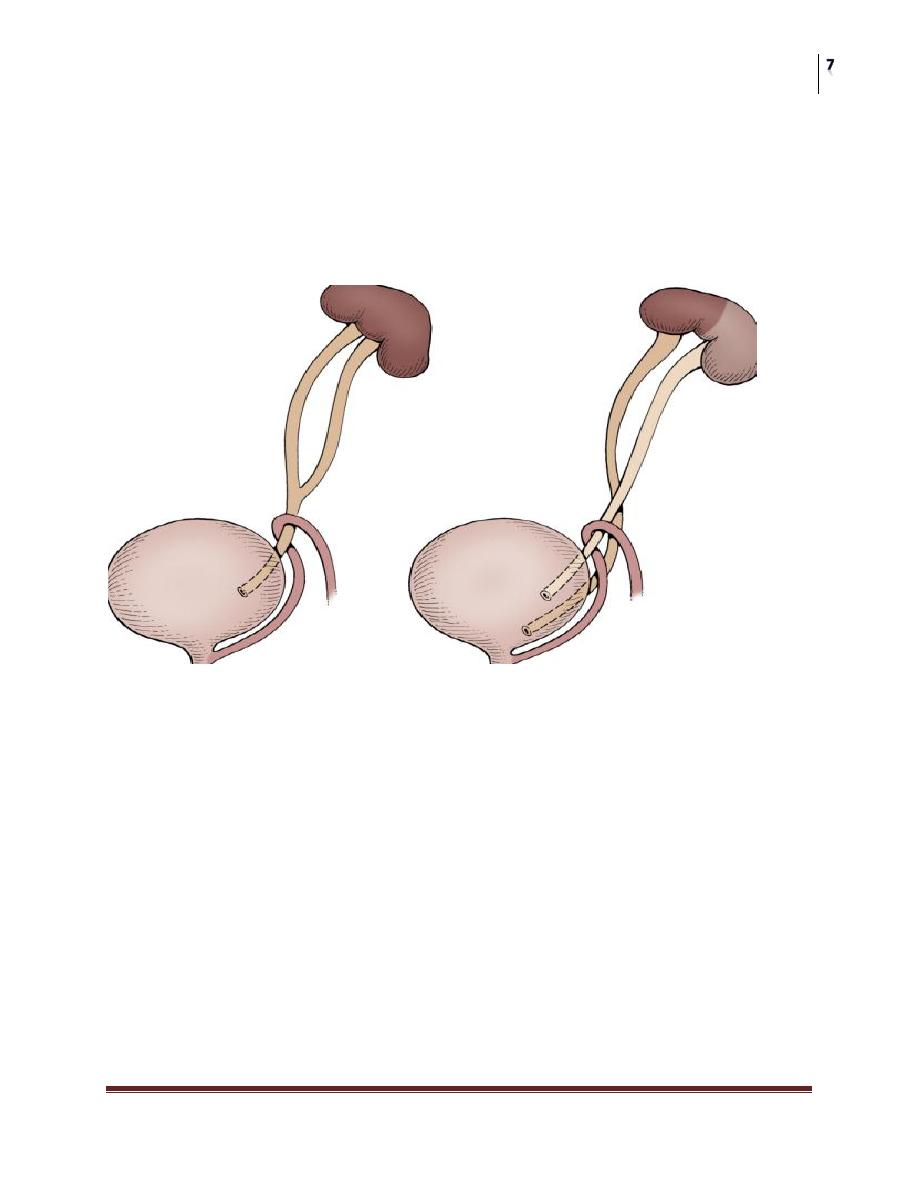
1. Duplication of ureter occurs in 1 per 125 autopsies; 1.6:1 female, 85%
unilateral.
a) Autosomal dominant with incomplete penetrance.
b) Seems to arise from two ureteral buds meeting the metanephros—in most
cases,
c) Associated with reflux (42%),
d) Duplication itself is of no clinical significance, but the associated anomalies
may require intervention (see ureterocele, ectopia
Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
Complications;
1- Incomplete:Bifid ureter is often clinically unimportant, but stasis and
pyelonephritis my occur.
2- Complete duplication;The upper ureter my be ectopic and lower ureter my be
refluxing, ureterocele my be associated with ectopic ureter.
2. Atresia is usually associated with a multicystic dysplastic Kidney
3. Megaureter has a 3:1 male and 3:1 left-sided predominance; the term is used
loosely to describe any dilated ureter, but there are three distinct types.
a) Refluxing megaureter originates because of the reflux
b) A widened ureteral bud gives rise to a ureter dilated down to the orifice,
which is in the normal position, and there is no obstruction (nonreflux,
nonobstructed type).
c) The primary obstructed type is the most common and results from a stenotic
or aperistaltic distal short segment; the orifice is in the normal position.
d) The refluxing type, with its laterally ectopic orifice
e) The ultrasound will show moderate to severe hydronephrosis

Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
VCUG will diagnose the reflux type; a Lasix
renogram would distinguish obstructed from non-obstructed types.
g) Surgical correction is needed for some obstructed and refluxing megaureters.
h) Follow-up includes ultrasound at 1 month and renal scan at 3 months. An
ultrasound is done 1 year postoperatively.
4. Vesicoureteral reflux (VUR)
Occurs in approximately 1 per 1000 in the general population ; it can be found in
50% of infants and 30% of children with a UTI.
a) It may occur because the ureteral bud arises ectopically leading to a laterally
placed orifice and short submucosal tunnel or because the development of
the intrinsic smooth muscle of the distal ureteral segment is delayed or
incomplete
b) Duplicated ureters and renal hypodysplasia may be associated with refluxing
ureters with laterally ectopic orifices.
Infection and renal scarring are prominent findings with all types of refluxing
ureters regardless of grade.
Voiding dysfunction and urethral obstruction by valves are associated with an
acquired form of reflux.
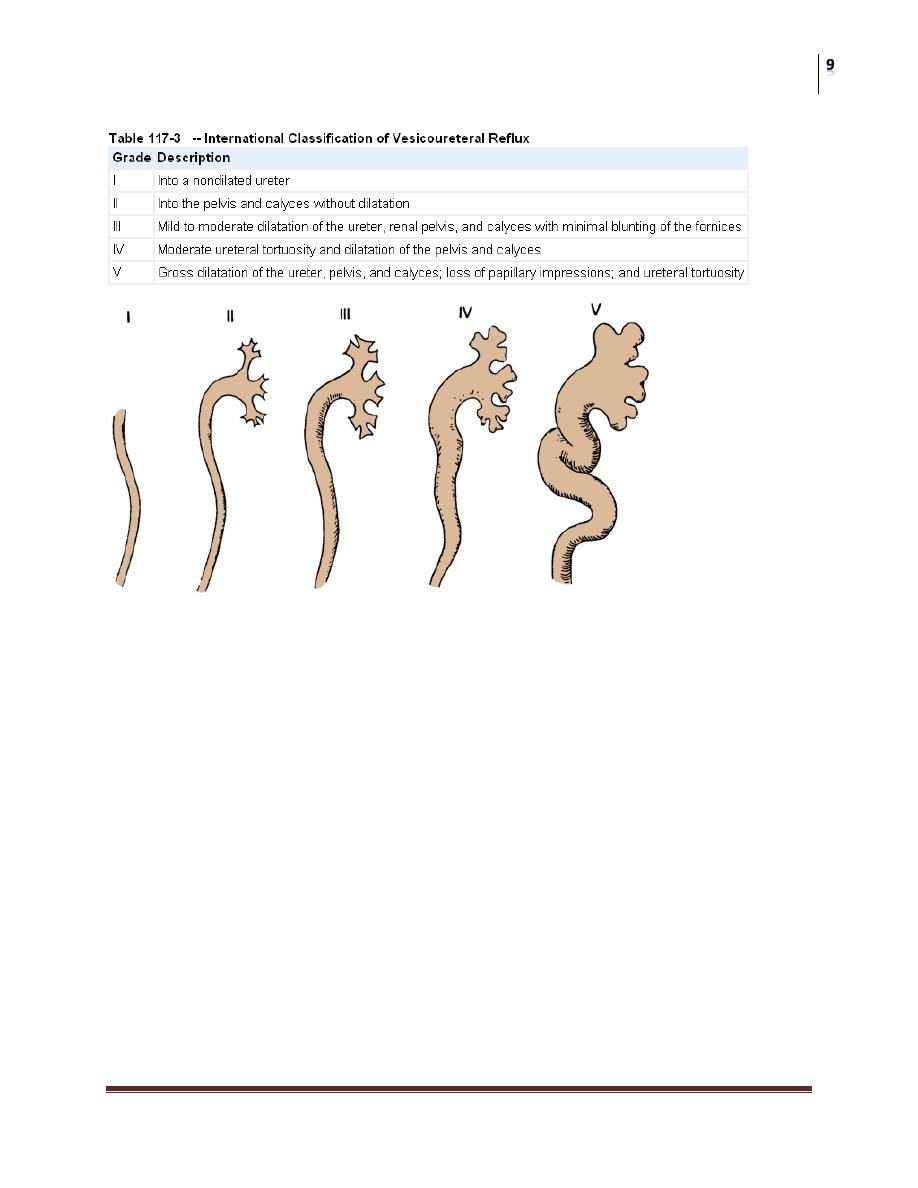
c) Reflux is best graded I to V by the International Reflux
Study system depending on the degree of dilation
d) All children with reflux should be placed on prophylactic antibiotics at one-
fourth the therapeutic dose. Trimethoprim-sulfamethoxazole and
nitrofurantoin are the most commonly used drugs after 2 months of age.
Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
Upper tract radiographic
Assessment usually with ultrasound and re-evaluation of the reflux by VCUG .
Some advocate the use of dimercaptosuccinic acid (DMSA).
e) Grades I–III (minimally dilated) are usually treated medically initially; grades
IV–V usually require surgical correction.
Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
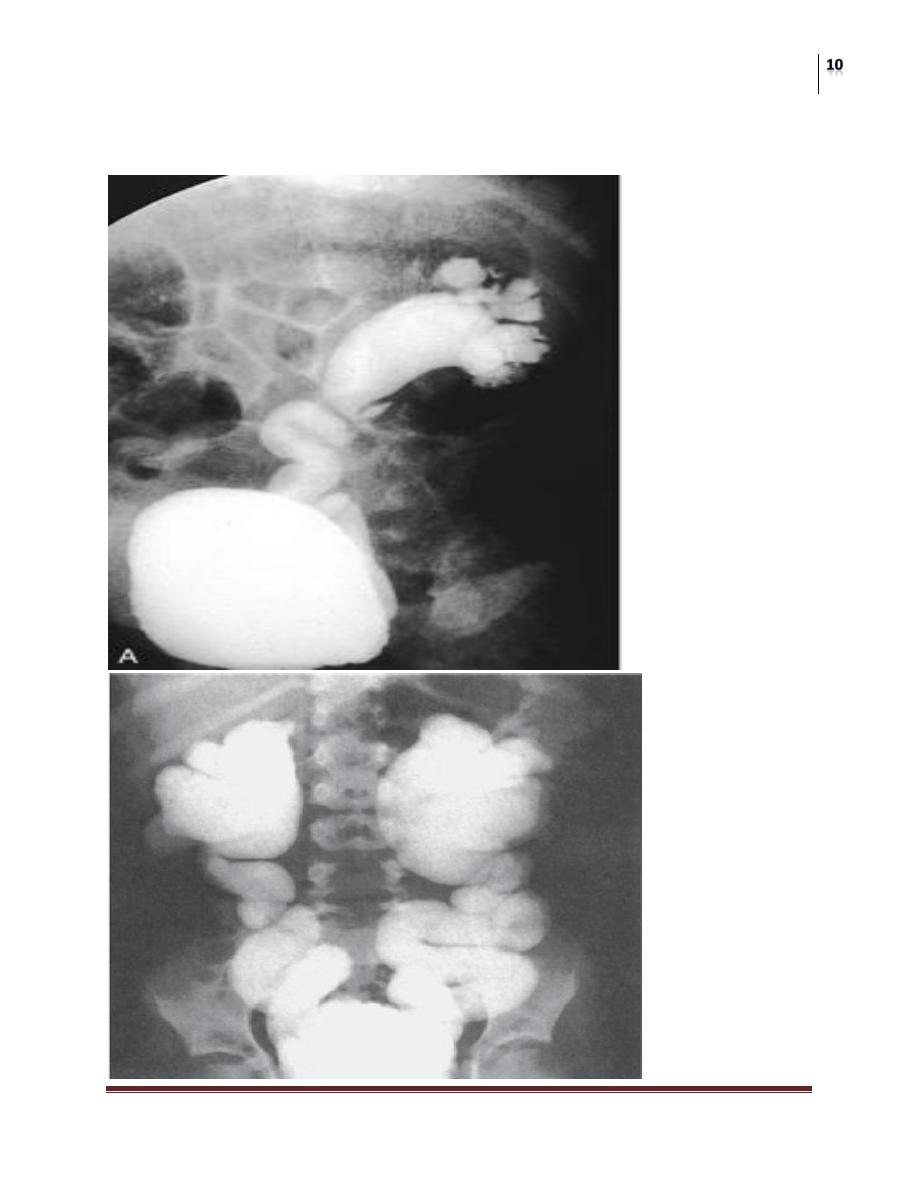
ASSESSMENT OF THE LOWER URINARY TRACT
Cystographic Imaging

Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
g) Breakthrough infections, failure to comply with the antibiotic prophylaxis
regimen, persistent reflux into puberty in females, progressive scarring, and
worsening renal function are all considerations that favor surgical intervention, but
there are no absolute indications for surgery for reflux.
5. The incidence of ureteral ectopia is approximately 1 per 1900; ectopic ureters
are duplex in 80% of females, more often single in males; there is a 3:1 female
predominance, and approximately 10% are bilateral.
a) The cause is a failure of the ureteral bud to separate from the
mesonephric duct, probably due to its ectopic origin on the duct.
b) Locations
c) Associated findings.
i) Renal dysplasia correlates with the degree of ectopy.
ii) Contralateral duplication
iii) Incontinence and ureteral obstruction
d) Management is most often removal of the renal segment and ectopic
ureter
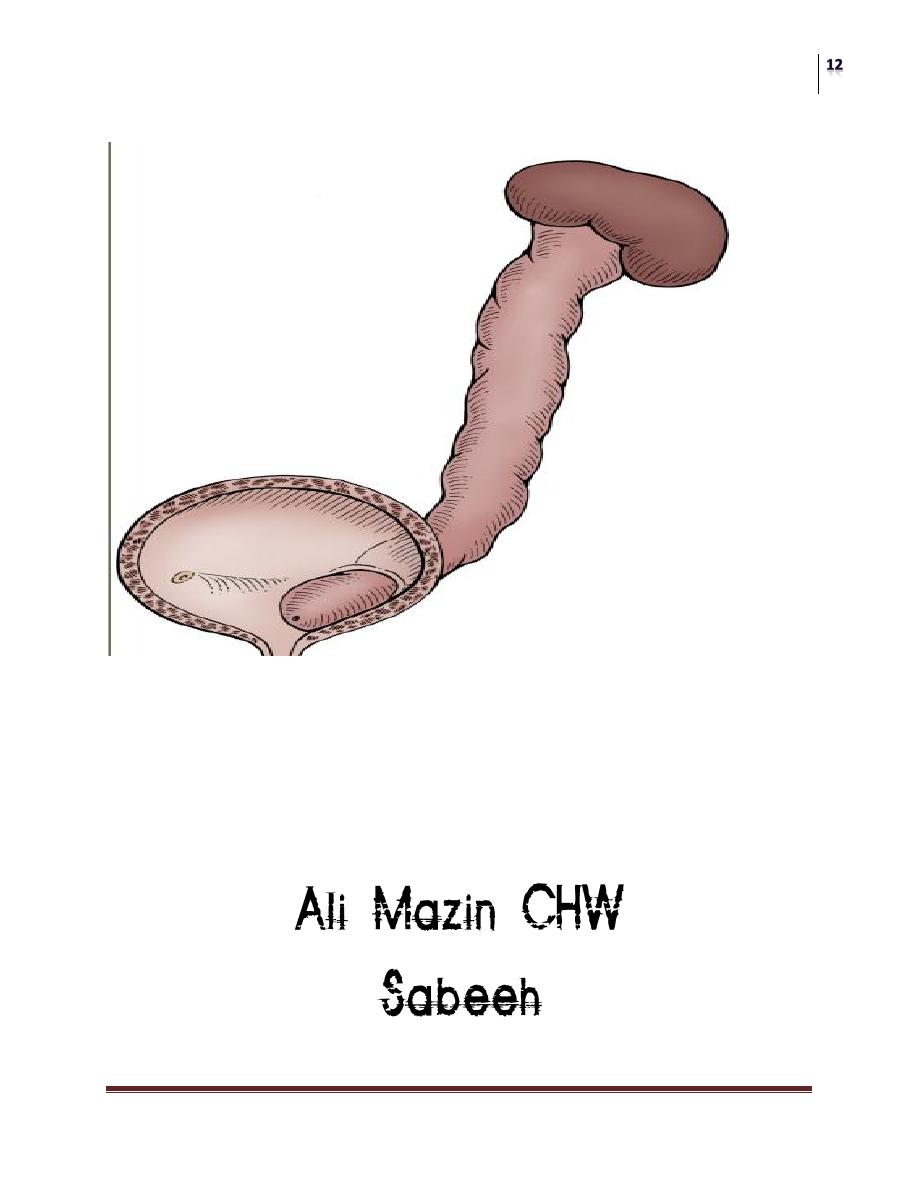
6. Ureterocele occurs with a frequency between 1 per 500 1% of pediatric urologic
admissions and is bilateral in 10–15% of cases. Females 4:1 over males.
Classification is based on location of the orifice and is typically defined as
intravesical or ectopic. Cecoureterocele, a subclassification of ectopic ureterocele,
differs in that a ‘‘cecum’’ extends beyond the orifice down the urethra; it may be
associated with poor bladder neck development and incontinence.
Surgery
Congenital Anomalies
Dr. Montadhar Al-Madani
Lec. 41
URETEROCELE
e) Management is varied.
1. Puncture of the ureterocele as newborn.
2. Upper pole nephrectomy with decompression of the ureterocele.