Surgery
Specific urinary Tract Infections
Dr. Ismaeel
Lec. 43
Tuberculosis
Tuberculosis (TB) of the genitourinary (GU) tract is caused by
Mycobacterium tuberculosis.
TB predominantly affects Asian populations,
Higher incidence in males than females.
TB is endemic in IRAQ.
Pathogenesis
Primary TB
The primary granulomatous lesion forms in the mid to upper zone
of the lung.
It consists of a central area of caseation surrounded by epithelioid
and Langhans giant cells, accompanied by caseous lesions in the
regional lymph nodes.
There is early spread of bacilli via the bloodstream to the GU
tract;
Surgery
Specific urinary Tract Infections
Dr. Ismaeel
Lec. 43
However, immunity rapidly develops, and the infection remains
quiescent.
Acute diffuse systemic dissemination of tubercle bacilli can result
in symptomatic military TB.
Post-primary TB:
Reactivation of infection is triggered by immune compromise
(including HIV).
It is at this point that patients develop clinical manifestations.
Kidney
Hematogenous spread causes granuloma formation in the renal
cortex, associated with caseous necrosis of the renal papillae and
deformity of the calyces, leading to release of bacilli into the urine.
This is followed by healing fibrosis and calcification, which
causes destruction of renal architecture and autonephrectomy
Ureters
Spread is directly from the kidney and can result in stricture
formation (vesicoureteric junction, pelviureteric junction, and mid-
ureteric) and ureteritis cystica.
Bladder
Infection is usually secondary to renal infection, although
iatrogenic TB can be caused by intravesical BCG treatment for
carcinoma in situ.
The bladder wall becomes edematous, red, and inflamed, with
ulceration and tubercles (yellow lesions with a red halo).
Disease progression causes fibrosis and contraction (resulting in a
small capacity ‗thimble‘ bladder), obstruction, and calcification.

Surgery
Specific urinary Tract Infections
Dr. Ismaeel
Lec. 43
Prostate and seminal vesicles:
Hematogenous spread causes cavitation and calcification, with
palpable, hard-feeling structures.
Fistulae may form to the rectum or perineum.
Epididymis:
Hematogenous spread results in a ―beaded‖ cord.
Infection may spread to the testis.
Presentation:
1. Early symptoms include fever, lethargy, weight loss, night sweats,
and UTI not responding to treatment.
2. Later manifestations include LUTS(lower urinary tract symptoms),
hematuria, and flank pain.
Investigations:
1. Urine: At least 3 early morning urines (EMUs) are required, but
often many more EMU specimens will be needed before a positive
culture for TB is obtained.
A typical finding is sterile pyuria (leukocytes, but no growth).
Ziehl–Neelsen staining will identify these acid- and alcoholfast bacilli
(cultured on Lowenstein–Jensen medium).
2. PCR of urine and blood.
3• CXR and sputum
4• Tuberculin skin test
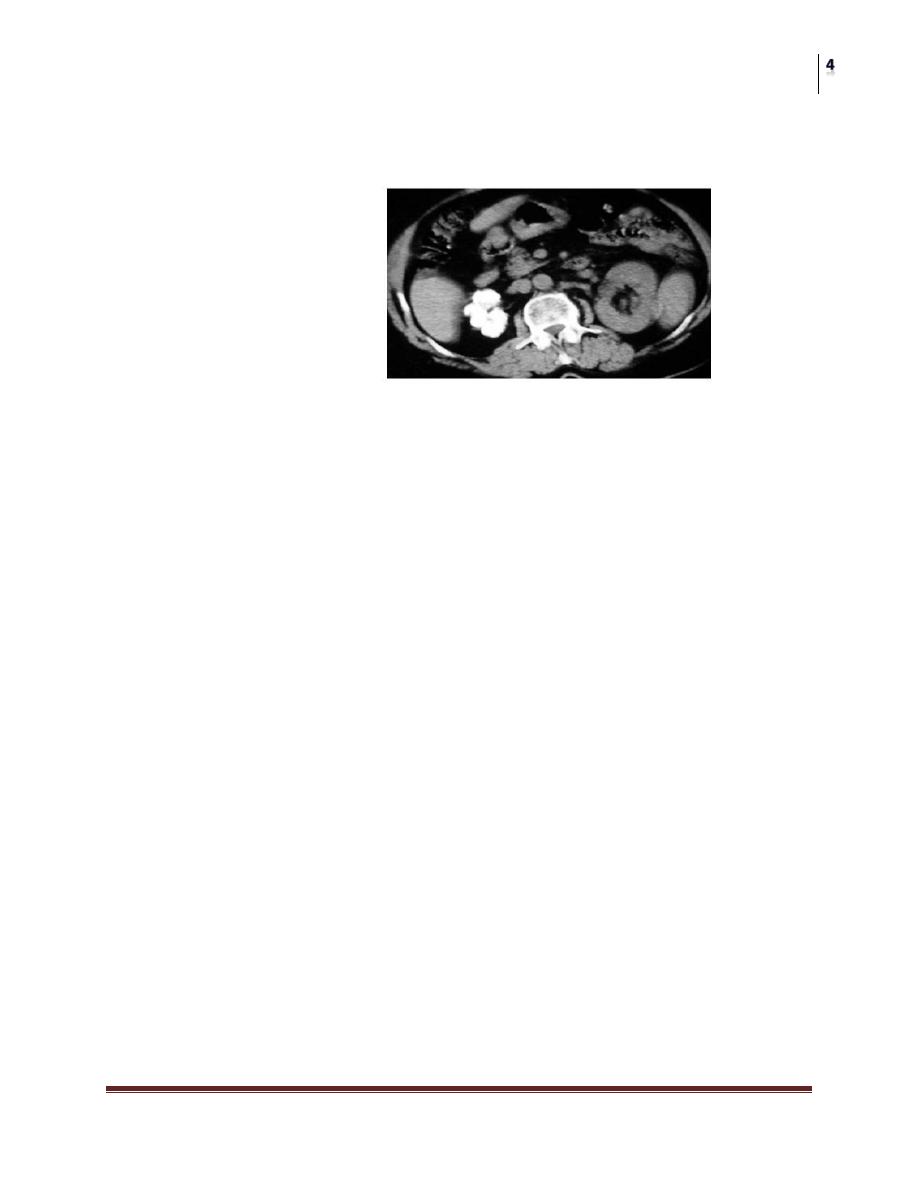
5• IVP or CT urogram: Findings include renal calcification
(nephrocalcinosis), irregular calyces (―moth-eaten kidney‖), infundibular
stenosis, cavitation, pelviureteric and vesicoureteric obstruction, and a
contracted, calcified bladder.
• Cystoscopy and biopsy
Surgery
Specific urinary Tract Infections
Dr. Ismaeel
Lec. 43
Sterile pyuria is TB until proved otherwise.
Beaded vas is TB until proved otherwise.
Chonic discharging scrotal sinus is TB proved otherwise.
Treatment:
Treatment is with 6 months of isoniazid, rifampicin, and
pyrazinamide.
Severely damaged kidney may need nephrectomy.
Regular follow-up imaging with IVP is recommended to monitor
for ureteric strictures, which may need stenting, nephrostomies, or
ureteric reimplantation.
Severe bladder disease may require surgical augmentation,
reconstruction, or urinary diversion.
Vesical ulcers may need transurethral electrocoagulation.
Surgery
Specific urinary Tract Infections
Dr. Ismaeel
Lec. 43
Parasitic infections
Schistosomiasis (bilharziasis)
Urinary schistosomiasis is caused by the trematode (or fluke)
Schistoma haematobium.
It is endemic in Africa, Egypt, and the Middle East(IRAQ).
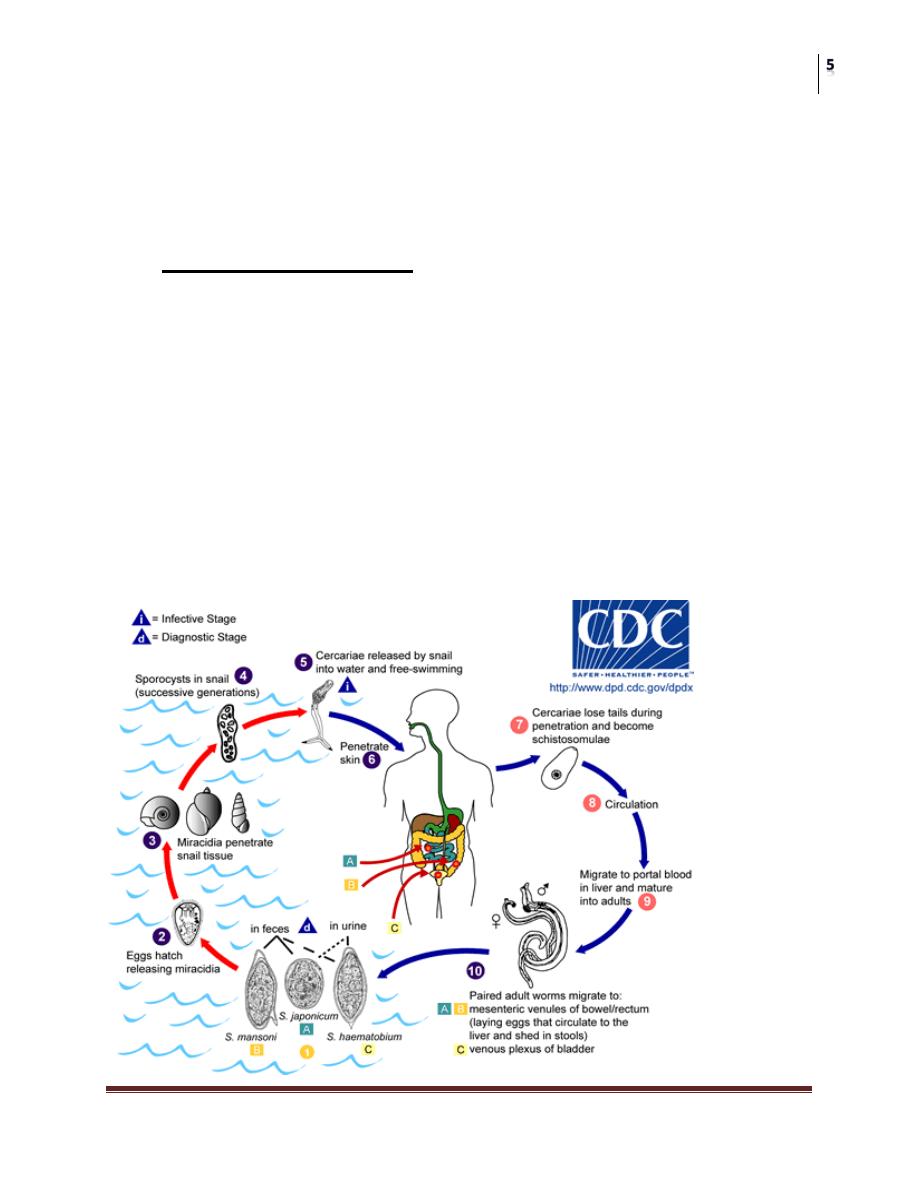
Life cycle
Fresh water snails release the infective form of the parasite
(cercariae),
Which can penetrate skin, and migrate to the liver (as
schistosomules), where they mature.
Adult flukes couple, migrate to vesical veins, and lay eggs
(containing miracidia larvae), which leave the body by penetrating
the bladder and entering the urine.

Surgery
Specific urinary Tract Infections
Dr. Ismaeel
Lec. 43
Pathogenesis:
The disease has two stages:
ACUTE STAGE:
Caused by the penetration and travel of cercariea .
CHRONIC STAGE:
1. Active (when adult worms are actively laying eggs) .clinically
manifested by dysuria and terminal haematuria.
2. Inactive (when the adult has died, and there is a reaction to the
remaining eggs).
Presentation
The first clinical sign is ―swimmer‘s itch‖—a local inflammatory
response.
Other early manifestations include Katayama fever, a generalized
allergic reaction, which includes fever, urticaria,
lymphadenopathy, hepatosplenomegaly, and eosinophilia.
Active inflammation results in hematuria, frequency, and
terminal dysuria.
Chronic disease manifestations: freq. , urgency,haematuria.
Investigation
• Midday urine specimen; bladder and rectal biopsies may contain eggs
(distinguished by having a terminal spine).
• Serology tests (ELISA).
• Cystoscopy identifi es eggs in the trigone (“sandy patches”).
• IVP or CT urogram may show a calcified, contracted bladder, and
obstructive uropathy.
Surgery
Specific urinary Tract Infections
Dr. Ismaeel
Lec. 43
Complications:
1. Chronic infection can lead to fibrosis and sometimes
calcifications leading to obstructive uropathy, ureteric stenosis,
renal failure, and bladder contraction, or ulceration.
2. Bilharizial ulcers.
3. The most significant and concerning complication is the
development of squamous cell carcinoma of the bladder that
often presents at an advanced stage.
Treatment
1.Acute stage:
Give praziquantel 40 mg/kg in 2 divided doses 4–6 hours apart.
Alternative medications include metrifonate or niridazole.
2. Chronic stage:
Bilharizial ulcers: cystoscopic fulguration.
Stricture formation in the ureter: release of stricture or reimplantation of
the ureter.
Bladder contracture: augmentation cystoplasty or even cystectomy and
urinary diversion.
Sq. cell ca. of the bladder: radical cystectomy with urinary diversion.
KEEP IN YOUR MIND:
1. Bilhariziasis is endemic in IRAQ.
2. Sq. cell ca. is the most fatal complication of the disease.
3. Surgical treatment is for the complications of bilharizial disease.