Surgery
Urological Emergencies 2
Dr. Ismaeel
Lec. 47
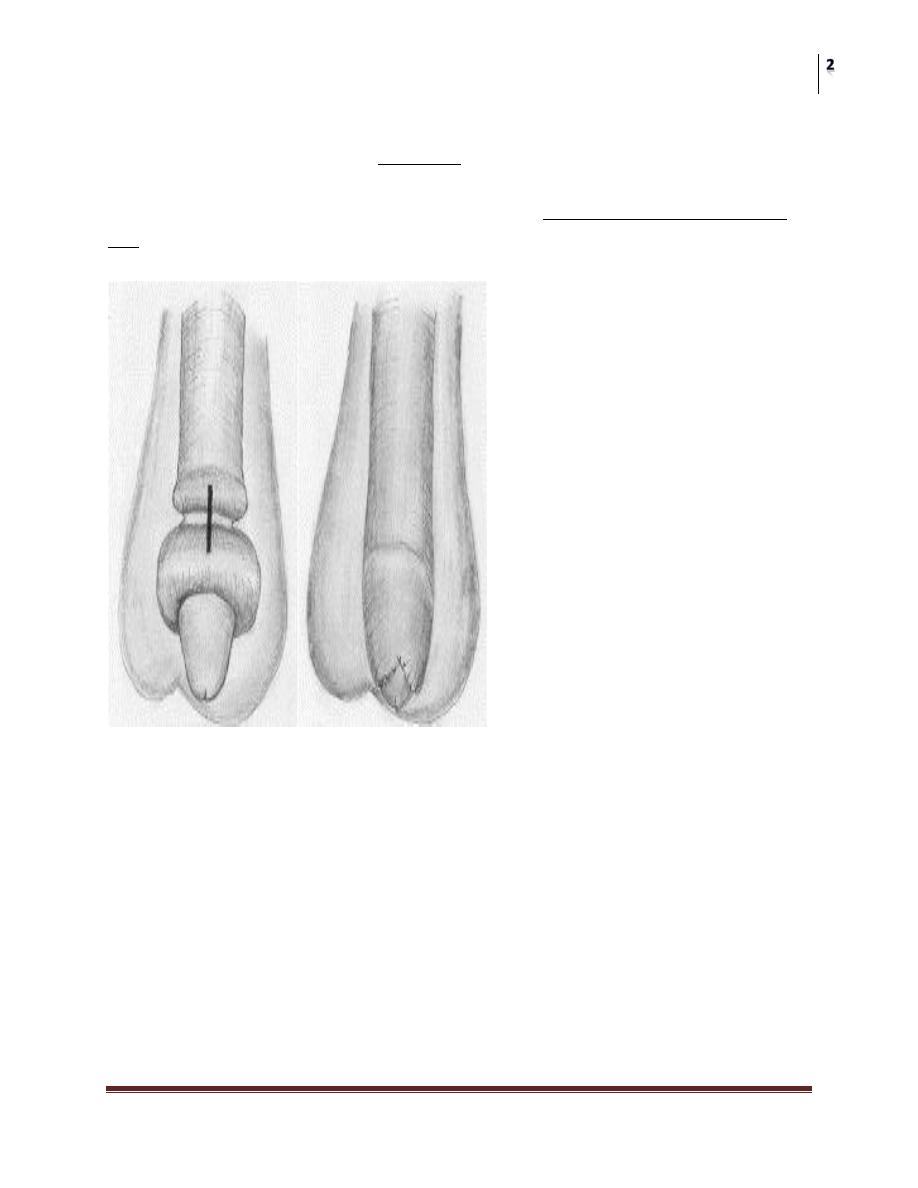
Paraphimosis
Definition:
Paraphimosis is when the uncircumcised foreskin is retracted under the glans penis
and the foreskin becomes edematous, and cannot be pulled back over the glans into
its normal anatomical position.
It occurs most commonly in:
1. Teenagers or young men.
2. In elderly men (who have had the foreskin retracted during catheterization,
but where it has not been returned to its normal position).
Paraphimosis if not treated urgently the result will be ischaemia of the glans with
subseq. Gangrene and necrosis of the glans.
Presentation:
1. Paraphimosis is usually painful
2. The foreskin is edematous and a small area of ulceration of the foreskin may
have developed.
Surgery
Urological Emergencies 2
Dr. Ismaeel
Lec. 47
Treatment:
1. The best initial maneuver for manually reducing paraphimosis is to forcefully
squeeze the edematous prepuce for several minutes.
2. If this fails, the traditional surgical treatment is a dorsal (longitudinal incision)
slit under general anesthetic or ring block.
3. Many patients subsequently require elective circumcision.
Fournier gangrene
Fournier gangrene is a necrotizing fasciitis (cellulitis of the skin and subcut.
tissue) of the genitalia and perineum primarily affecting males and causing
necrosis and subsequent gangrene of infected tissues.
Predisposing factors:
1. Diabetes,
2. Local trauma to the genitalia and perineum (e.g., zipper injuries to the foreskin,
traumatic catheterization or instrumentation of the urethra),
3. Surgical procedures such as circumcision.

Surgery
Urological Emergencies 2
Dr. Ismaeel
Lec. 47
Microbiology:
Culture of infected tissue reveals a mixed polymicrobial infection with aerobic (E.
coli, enterococcus, Klebsiella) and anaerobic organisms (Bacteroides, Clostridium
Mortality rate is about 20% despite proper treatment.
Presentation:
1. This is one of the most dramatic and rapidly progressing infections in
medicine.
2. Ill, toxic patient with fever and marked pain in the affected tissues.
3. The genitalia and perineum are edematous, and on palpation of the affected
area, tenderness and crepitus may be present (subcutaneous gas produced by
gas-forming organisms).
4. As the infection advances, blisters (bullae) appear in the skin and, within a
matter of hours, areas of necrosis and gangrene may develop on the genitalia
and perineum that spread to involve adjacent tissues (e.g., the lower
abdominal wall).
Treatment
1. Do not delay.
2. Transfer the patient to the operating room emergently so that debridement of
necrotic tissue (skin, subcutaneous fat) can be carried out.
3. IV access is obtained, blood taken for culture, IV fluids started, and oxygen
administered, broad-spectrum antibiotics are given to cover both gram-
positive and gram-negative aerobes and anaerobes.
4. Urinary diversion (suprapubic catheter).
5. Where facilities allow, consider treatment with hyperbaric oxygen therapy
Priapism
Priapism is prolonged and often painful erection in the absence of a sexual
stimulus, lasting >4–6 hours, which predominantly affects the corpus cavernosa.
Epidemiology
It peaks in incidence at ages 5–10 and 20–50 years.

Surgery
Urological Emergencies 2
Dr. Ismaeel
Lec. 47
Etiology:
primary (idiopathic).60%
secondary:
1. Intracavernosal injection therapy—PGE1; papaverine(most common).
2. Drugs—B-blockers; antidepressants; antipsychotics; psychotropics;
tranquilizers; anxiolytics; anticoagulants; recreational drugs; alcohol excess; total
parenteral nutrition.
3. Thromboembolic—sickle cell disease (roughly one-third develop
stuttering/recurrent priapism); leukemia; thalassemia.
4. Malignant infiltration of the corpora cavernosa (e.g., advanced bladder cancer).
5. Neurogenic—spinal cord lesion; autonomic neuropathy; anesthesia.
6. Trauma—penile or perineal injury resulting in cavernosal artery laceration or
arteriovenous fistula formation.
7. Infection—malaria; rabies; scorpion sting
Pathophysiology:
Priapism lasting for 12 hours causes trabecular interstitial edema,
Followed by destruction of sinusoidal endothelium and exposure of the
basement membrane at 24 hours,
And sinusoidal thrombi, smooth muscle cell necrosis, and fibrosis at 48
hours.
Classification:
1. Low-flow (ischemic) priapism:
This is due to veno-occlusion.
It is more common than high-flow priapism.
It manifests as a painful, rigid erection, with absent or low cavernosal blood
flow.
Ischemic priapism beyond 4 hours requires emergency intervention.
Blood gas analysis shows hypoxia and acidosis.
2. High-flow (nonischemic) priapism:
This is usually post-traumatic in nature
Does not require emergent intervention.
It is due to unregulated arterial blood flow, presenting with a semi-rigid,
painless erection.
Surgery
Urological Emergencies 2
Dr. Ismaeel
Lec. 47
Blood gas analysis shows similar results to arterial blood.
3. Stuttering (recurrent) priapism: usually occurs in sickle cell anaemia.
Evaluation:
• CBC to exclude sickle cell and leukemia.
• Cavernous arterial blood samples to determine the type of priapism (high or low
flow).
• Color Doppler ultrasound scan of cavernosal artery and corpora cavernosa.
1. Reduced blood flow in ischemic priapism;
2. Ruptured artery with pooling of blood around injured area in nonischemic
priapism.
ISCHAEMIC PRIAPISM is a Urological Emergency because if left untreated the
result will be IMPOTENCE.
Management
Low-flow priapism
Ischemic priapism of >4 hours implies a compartment syndrome and requires
decompression of the corpora cavernosa.
@Aspiration of blood from corpora ± intracavernosal injection of A1-adrenergic
selective agonist (phenylephrine100–200 μg are performed every 5–10 minutes
until detumescence occurs.
@if this fail: SHUNT procedures (create a shunt for the evacuation of the
blood).shunt procedures could be distal or proximal.
Sickle cell disease requires, in addition, aggressive rehydration,
oxygenation, analgesia, and hematological input (consider exchange
transfusion),plus
Repeated aspirations or irrigations and sympathomimetic injections are often
necessary.
Surgery
Urological Emergencies 2
Dr. Ismaeel
Lec. 47
High-flow priapism
Early stages may respond to a cool bath or icepack (causing vasospasm±
arterial thrombosis).
Delayed presentations require arteriography and selective embolization of
the internal pudendal artery.
Complications
These include fibrosis and impotence (90% after 24 hours).