Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50
Benign tumors and lesions
Non cutaneous
• Congenital and acquired inclusion cysts
• Retention cysts
• Syringomas (sweat gland tumors)
• Neurilemoma
• Angioma, lipoma
• Iatrogenic pseudotumor following injections
• Pyogenic granuloma following injections
Cutaneous
• Pearly penile papules (normal in 15% of postpubertal males)
• Zoon balanitis (shiny, erythematous plaque on glans or prepuce)
• Lichen planus (fl at-topped violaceous papule)
Viral-related lesions
Condyloma acuminatum
• This is also known as genital warts
• Related to human papillomavirus (HPV) infection.
• There are soft, usually multiple benign lesions on the glans, prepuce and
shaft; they may occur elsewhere on genitalia or perineum.

Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50
• A biopsy is worthwhile prior to topical treatment with podophyllin 5%have
urethral involvement, which may require diathermy.
Bowenoid papulosis
Resembles carcinoma in situ, but with a benign course.
Multiple papules appear on the penile skin, or a fl at glanular lesion.
These should be biopsied.
HPV is the suspected cause.
Kaposi sarcoma
This reticuloendothelial tumor.
Second-most common malignant penile tumor.
In immunocompromised men, particularly in gay men with HIV/AIDS.
Treatment is palliative, with intralesional chemotherapy, laser, cryoablation,
or radiotherapy.
Premalignant cutaneous lesions
Histologically benign lesions are recognized to have malignant potential.
Occur in close association with SCC of the penis.
A chronic red or pale lesion on the glans or prepuce is a cause for concern.
Early follow-up after use of steroid, antibacterial, or antifungal creams is
recommended.
If persistent, biopsy is advised.
Balanitis xerotica obliterans (BXO)
Also known as lichen sclerosus et atrophicus.
This is a common sclerosing condition of glans and prepuce.
It occurs at all ages.
Most commonly presents as non-retractile foreskin (phimosis).
Obstructed and spraying voiding.
Occurs in association with penile SCC.

Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50
Leukoplakia:
Solitary or multiple whitish glanular plaques.
Usually involve the meatus.
Treatment is excision and histology.
associated with in situ SCC;
Follow-up is required.
Erythroplasia of Queyrat:
Known as carcinoma in situ of the glans, prepuce, or penile shaft.
A red, velvety, circumscribed painless lesion occurs, though it may ulcerate,
resulting in discharge and pain.
Treatment is excision biopsy if possible; radiotherapy, laser ablation, or
topical 5-fl uorouracil may be required. Histology reveals hyperplastic
mucosal cells with malignant features.
Bowen disease:
this is carcinoma in situ of the remainder of the
keratinizing genital or perineal skin.
Treatment is wide local excision, laser, or cryoablation.
Buschke–Löwenstein tumor:
known as verrucous carcinoma or giant condyloma acuminatum,
An aggressive locally invasive tumor of the glans.
Metastasis is rare, but wide excision is necessary to distinguish it from
SCC.
Urethral erosion and fi stulation may occur.
Squamous cell carcinoma (SCC)
is the most common penile cancer,accounting for 95% of penile
malignancies.
Others include Kaposi sarcoma and, rarely, basal cell carcinoma, melanoma,
sarcoma, and Paget disease.
Metastases to the penis are occasionally seen from the bladder, prostate,
rectum, and other primary sites.

Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50
Incidence and etiology of SCC
1% of male cancers.
Age: penile cancer incidence rises during the sixth decade and peaks in the
eighth decade. It is unusual <40 years of age, but has been rarely reported in
children.
Premalignant lesions42% of patients with penile SCC are reported to have
had a pre-existing penile lesion.
A prepuce (foreskin):penile cancer is rare in men circumcised at a young
age. Smegma that forms from desquamated epithelial cells is thought to be a
primary instigating factor in penile cancer; good hygiene and circumcision
limit smegma accumulation.
Geography:Highest incidence worldwide is in Brazil. It is virtually non-
existent in Israel.
Human papilloma virus (HPV) genital wart infection, especially with types
16, 18, and 21.
Multiple sex partners.
Smoking and tobacco.
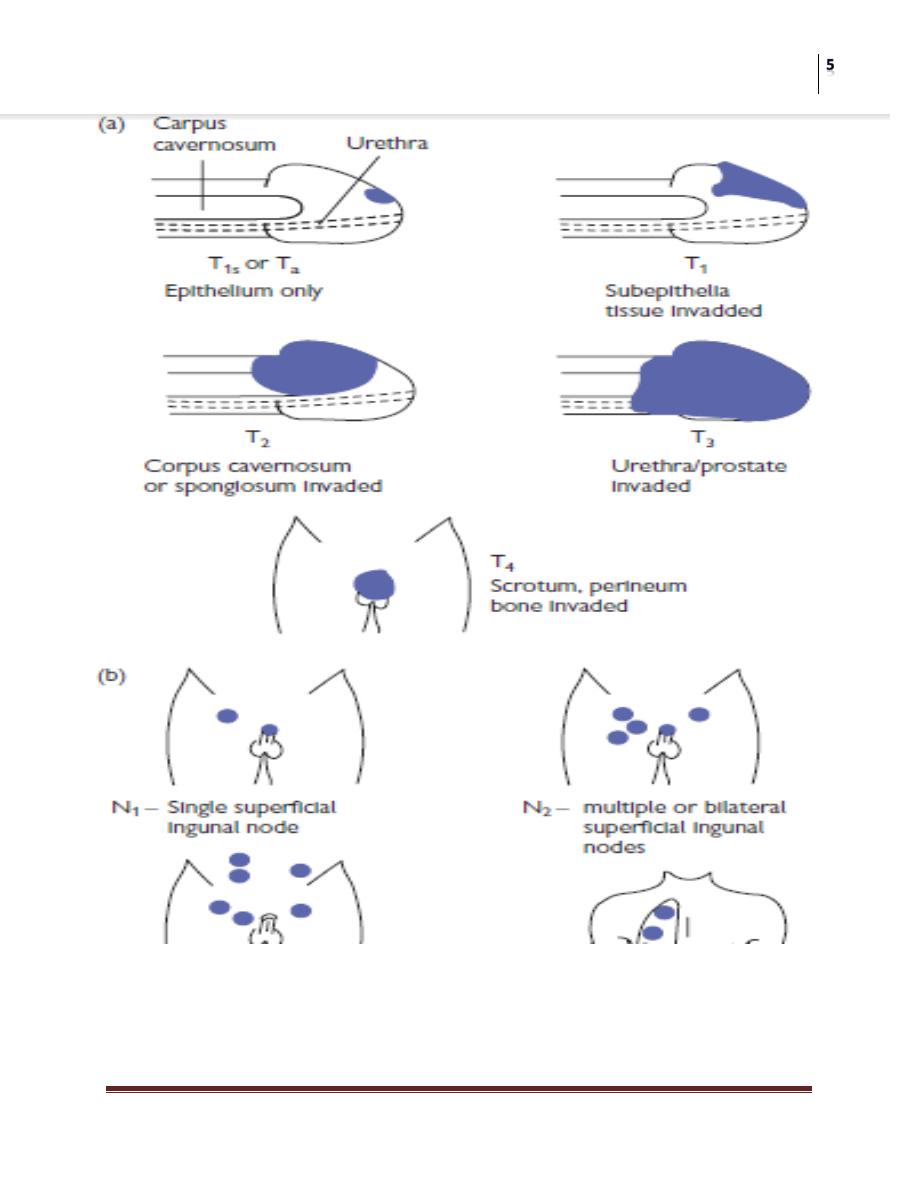
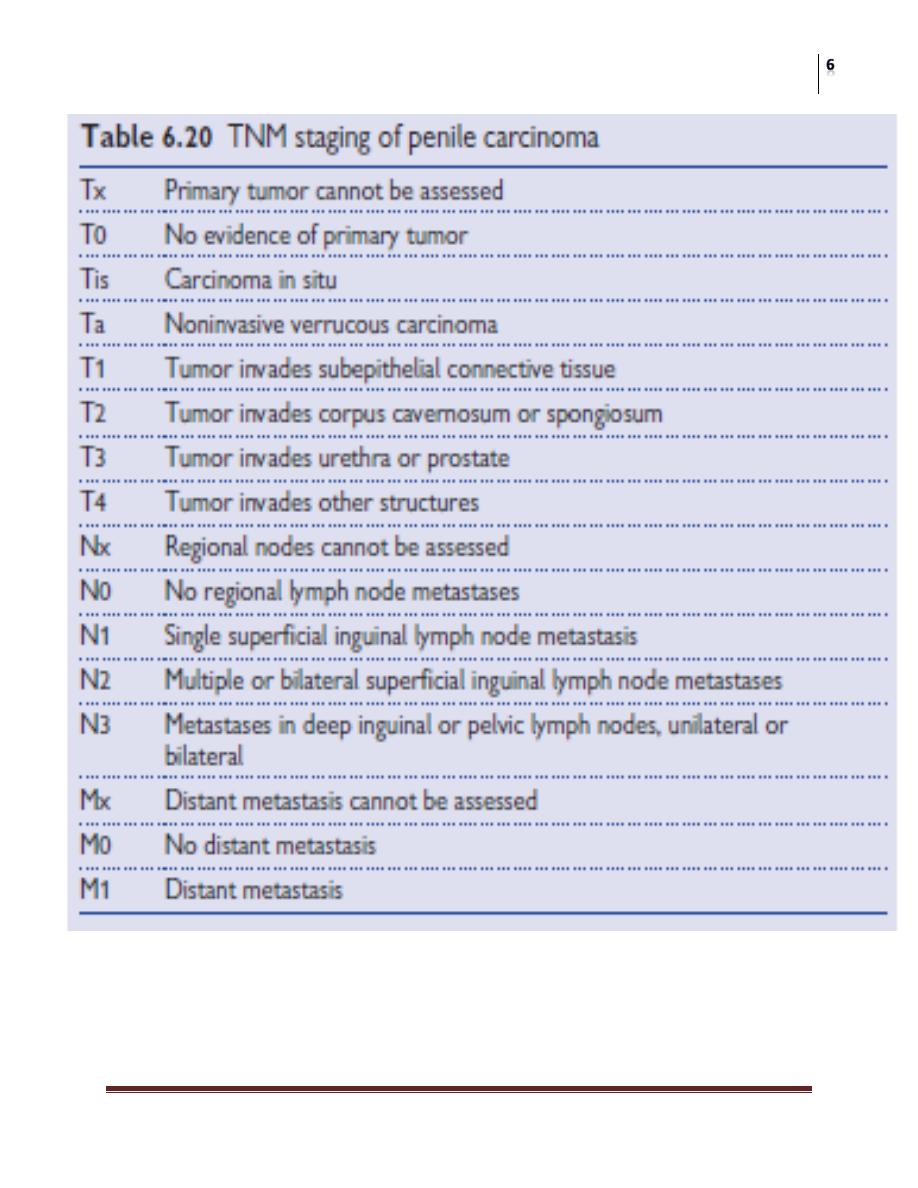
Pathology and staging of penile SCC
Believed to be preceded by carcinoma in situ.
SCC starts as a slow-growing papillary, flat or ulcerative lesion on the glans
(48%), prepuce (21%), glans and prepuce (9%), coronal sulcus (6%), or
shaft (2%).
The remainder is indeterminate.
It grows locally beneath the foreskin before invading the corpora cavernosa,
urethra, and, eventually, the perineum, pelvis, and prostate.
Metastasis is initially to the superficial then deep inguinal and, subsequently,
iliac and obturator lymph nodes.
Skin necrosis, ulceration, and infection of the inguinal lymph nodes may
lead to sepsis or hemorrhage from the femoral vessels.
Blood-borne metastasis to lungs and liver is rare (1–10% of cases).
Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50
Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50

Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50
SCCs are graded using the Broder classification system:
• Grade I: well differentiated, keratinization, prominent intercellular bridges,
keratin pearls
• Grade II to III: greater nuclear atypia, increased mitotic activity, decreased
keratin pearls
• Grade IV: cells deeply invasive, marked nuclear pleomorphism, nuclear mitoses,
necrosis, lymphatic and perineural invasion, no keratin pearls
Presentation
About 15–50% of patients delay presentation for >1 year because of
embarrassment, personal neglect, fear, or ignorance.
A hard, painless lump on the glans penis is the most common presentation.
A bloody discharge may be confused with hematuria.
Rarely, a groin mass or urinary retention are presenting symptoms.
Investigations
A biopsy is indicated.
Chest radiology, pelvic CT scan,
serum calcium, and
Liver function tests are usually obtained.
Treatment
The management of penile cancer should take place in regional or
supraregional centers that can provide multidisciplinary surgical and
oncological expertise.
The first-line treatment of penile cancer, regardless of the inguinal node
status, is surgery
Circumcision is appropriate for preputial lesions, but local recurrence is
observed in 22–50%.

Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50
1/ Primary tumor:
for smaller G1–2 Ta–1 tumors
Penis-preserving wide excision of glanular lesions with skin graft glanular
reconstruction.
Alternatives to surgery include laser or cryoablation, radiotherapy or
brachytherapy, photodynamic therapy, or topical 5-fl uorouracil.
For G3T1 and more advanced tumors, partial or total penile amputation is
required, depending on the extent of the tumor.
• Radiotherapy remains an alternative
Patients with M1 disease are offered palliative surgery.
2/ Lymphadenopathy:
Six weeks of broad-spectrum antimicrobials (e.g., Augmentin or
cephalosporin) are given after the primary tumor has been removed.
If nodes become clinically nonpalpable (50% of patients), who may then be
followed up.
For those with persistent inguinal lymphadenopathy, in the absence of
demonstrable pelvic or metastatic disease, bilateral inguinal
lymphadenectomy should be considered
Radiotherapy and chemotherapy:
Are alternative or adjuvant treatments for metastatic nodal disease in unfi t,
elderly, or inoperable patients.
Prophylactic lymphadenectomy:
This is currently practiced in the United States for tumors exhibiting
vascular invasion, are high grade, or stages T2–4.
Distant metastatic disease:
This is treated using single-agent systemic chemotherapy: cisplatin,
bleomycin,or methotrexate.

Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50
Urethral cancer
Primary urethral cancer is rare, occurring in elderly patients.
It is 4 times more common in women than in men.
Risk factors:
Urethral stricture and sexually transmitted disease are implicated.
Direct spread from tumor in the bladder or prostate is more common.
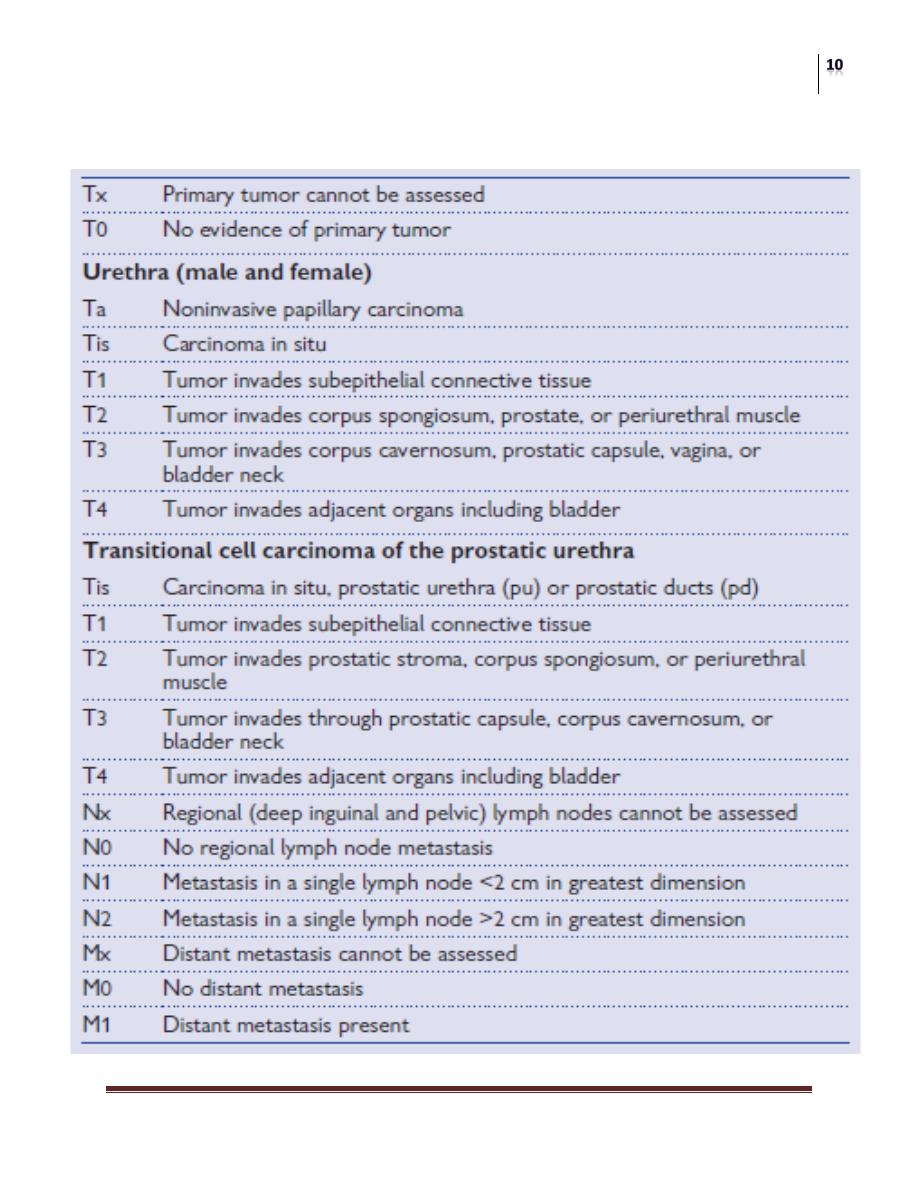
Pathology and staging:
75% are SCC, occurring in the anterior urethra;
15% are UC, occurring in the posterior/prostatic urethra;
8% are adenocarcinoma;
And the remainder includes sarcoma and melanoma.
Urethral cancer metastasizes to the pelvic lymph nodes from the posterior
urethra
To the inguinal nodes from the anterior urethra in 50% of patients.
Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50
Staging is by the TNM system

Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50
Presentation
This is often late; many patients have metastatic disease at presentation
• Painless hematuria; initial, terminal, or a bloody urethral discharge
• Voiding-type LUTS (less common)
• Perineal pain (less common)
• Periurethral abscess or urethrocutaneous fi stula (rare)
• Past history of sexually transmitted or stricture disease
• Examination may reveal a hard, palpable mass at the female urethral meatus or
along the course of the male anterior urethra. Inguinal lymphadenopathy, chest
signs, and hepatomegaly may suggest metastatic disease.
Differential diagnosis
In men
• Urethral stricture
• Perineal abscess
• Metastatic disease involving the corpora cavernosa
• Urethrocutaneous fi stula (secondary to benign stricture disease)
In women
• Urethral caruncle
• Urethral cyst
• Urethral diverticulum
• Urethral wart (condylomata acuminata)
• Urethral prolapse
• Urethral vein thrombosis
• Periurethral abscess
Investigations
Cystourethroscopy,
Biopsy.
Bimanual examination under anesthesia.
Chest radiography
abdominopelvic CT scan.
Surgery
Penile Neoplasia
Dr. Montadhar Almadani
Lec. 50
Treatment
1/ for localized anterior urethral cancer, radical surgery or radiotherapy are the
options.
Male patients would require perineal urethrostomy.
Postoperative incontinence is minimum.
For posterior/prostatic urethral cancer,
cystoprostatourethrectomy should be considered for men in good overall
health,
While anterior pelvic exenteration (excision of the pelvic lymph nodes,
bladder, urethra, uterus, ovaries, and part of the vagina) should be
considered for women.
2/ for locally advanced disease, a combination of preoperative radiotherapy and
surgery is recommended.
3/ For metastatic disease, chemotherapy is the only option with regimens of
systemic cisplatin, bleomycin, and methotrexate or 5-fl uorouracil.