Surgery
Esophagus
Prof. Dr. Waleed Mustafa
Lec. 3
CARCINOMA ESOPHAGUS
Carcinoma of the esophagus is a disease of men between age) (50-70).
Two risk factors: Smoking, High consumption of alcohol.
Predisposing lesions:
1. Achalasia
2. Barret esophagus
3. Corrosive stricture
4. Plummer Vinson syndrome.
Pathology:
1. Squamous cell carcinoma > 95% most common (body).
2. Primary adenocarcinoma < 1-7% most common of them is adenocarcinoma arise in
Barrett’s esophagus.

Surgery
Esophagus
Prof. Dr. Waleed Mustafa
Lec. 3
3. Mucoepidermoid &Adenocystic carcinoma. Rare.
Most malignant lesions are ulcerating & encircling the esophagus. Malignant lesion
involving the EG junctions adenocarcinoma of gastric origin.
Spread:
1. Direct extension.
2. Lymphatic to cervical, mediastinal and sub diaphragmatic.
3. Blood metastases liver, lung &bone.
Clinical manifestations:
Dysphagia, to solid later to liquid, Weight loss, Aspiration pneumonia .Pressure
symptoms.
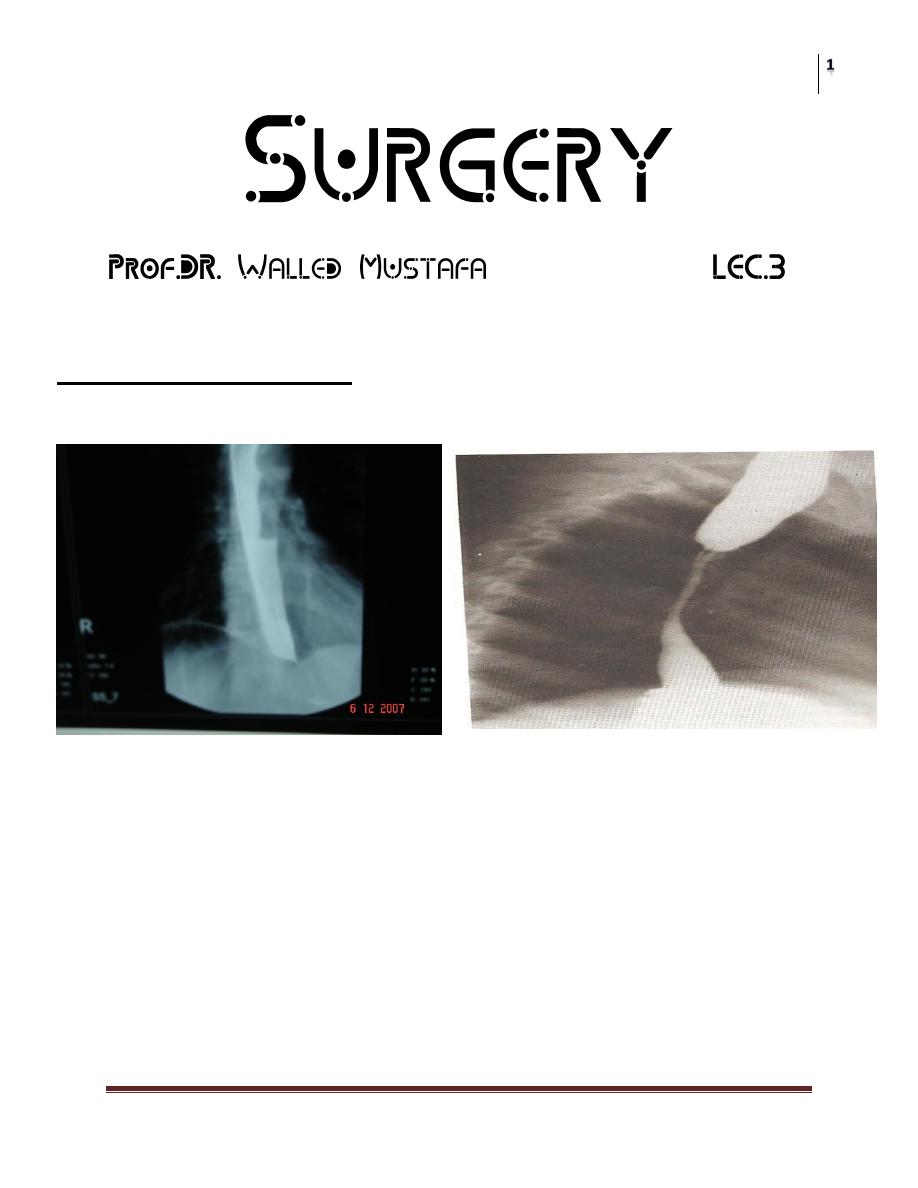
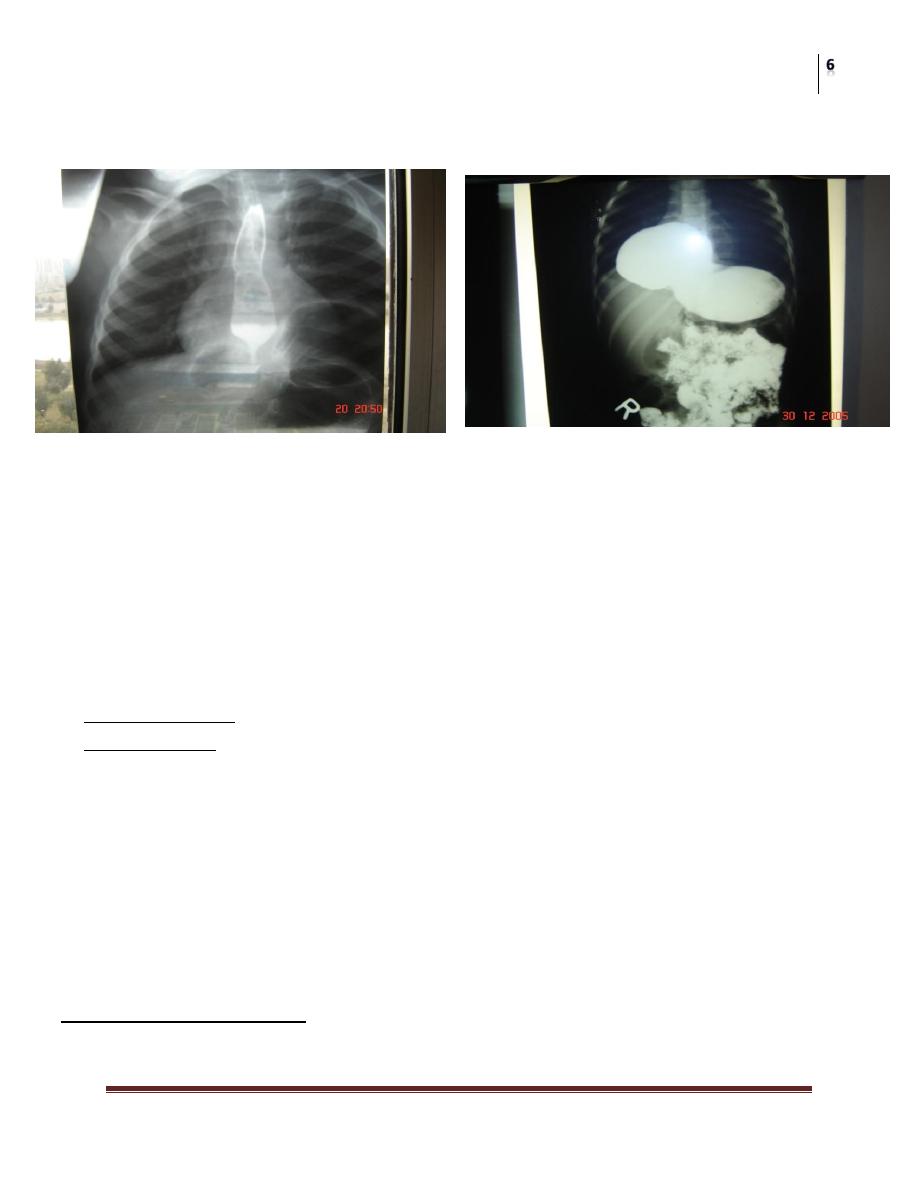
Barium – swallow: irregular ragged mucosal pattern with annular luminal narrowing.
Esophagoscopy: to see the tumor, to take biopsy (tissue diagnosis), and esophageal wash
for cytology.
CT with oral contrast
Treatment:
1. Chemo-therapy little value.
2. Radio-therapy useful but it may cause post radiation stricture, radiation pneumonitis.
3. Surgery a- palliative
b- Resection
Partial gastrectomy, partial esophagectomy & gastro esophageal anastomosis (Ivor Lewis
operation) through lapratomy & thoracotomy.
Approaches left thoracotomy
laparatomy & right thoracotomy
laparatomy & cervical incision
Thoracoabdominal.
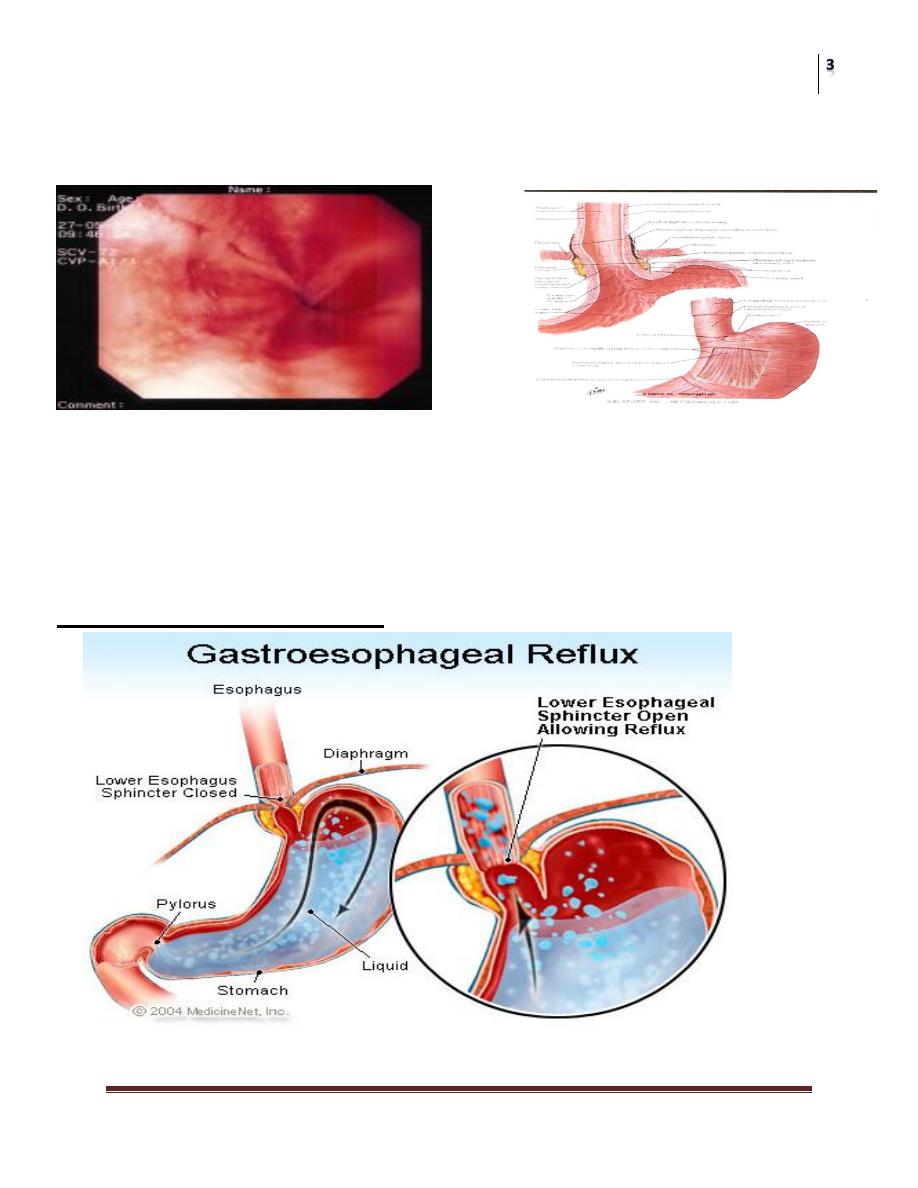
Gastro Oesophageal Reflux Disease (GORD)
Heart burn GORD
Heartburn: Mild, intermittent reflux of gastric content into the esophagus without tissue
injury. Common among adult.
Surgery
Esophagus
Prof. Dr. Waleed Mustafa
Lec. 3
GORD: Esophagitis with varying degree of erythema, edema & friability of the distal
esophageal mucosa.
Etiology:
1. Lower esophageal sphincter (LES) incompetence.
2. Gastric outlet obstruction.
3. 50% of patients with GORD have an associated hiatal hernia.
4. Defective esophageal function (Scleroderma )
Mechanism of Anti –Reflux
Surgery
Esophagus
Prof. Dr. Waleed Mustafa
Lec. 3
1. High resting pressure in the distal esophagus (10-20 mm Hg) which is greater than the
adjacent stomach acting as a barrier.
2. Muscle sling, the looping of the muscle fiber of the right crus of the diaphragm
around the esophago - gastric junction.
3. The phreno esophageal membrane which anchor the esophagus within the hiatus.
4. The presence of the intra-abdominal segment of the esophagus .It is subjected to a
highly positive intra-abdominal pressure.
5. The oblique angle of insertion of the esophagus into the stomach (angle of His).
6. The small diameter of the esophagus entering abruptly into the large diameter
(stomach) Law of Laplace.
Clinical features:
1. Epigastric or retro sternal pain, after meal or at night.
2. Pain similar to angina.
3. Reflux of food or gastric content, occurs with bending.
4. Odynophagia.
5. Pulmonary aspiration, nocturnal cough.
Diagnosis:
1. History and physical examination.
2. Barium swallows.
3. Oesophago gastro dudenoscopy (OGD ) & biopsy.
4. Ambulatory 24 – hours PH monitoring.
5. Esophageal manometry, when motility disorders is suspected.
Treatment
1. Medical:
a. Weight reduction.
b. Change diet (light frequent meal).
c. Stop smoking.
d. Elevate the head of the bed (4-5 inches).
e. Anti-acid.
f. Metoclopromide increase LES pressure & gastric emptying.
g. H2 receptor blockers Ranitidine (Zantac).
h. Proton pumps inhibitor omeprazole.
Surgery
Esophagus
Prof. Dr. Waleed Mustafa
Lec. 3
2. Surgical:
Indications:
a. Failure of medical treatment.
b. Presence of complications (stricture, respiratory symptoms).
c. Patient preference.
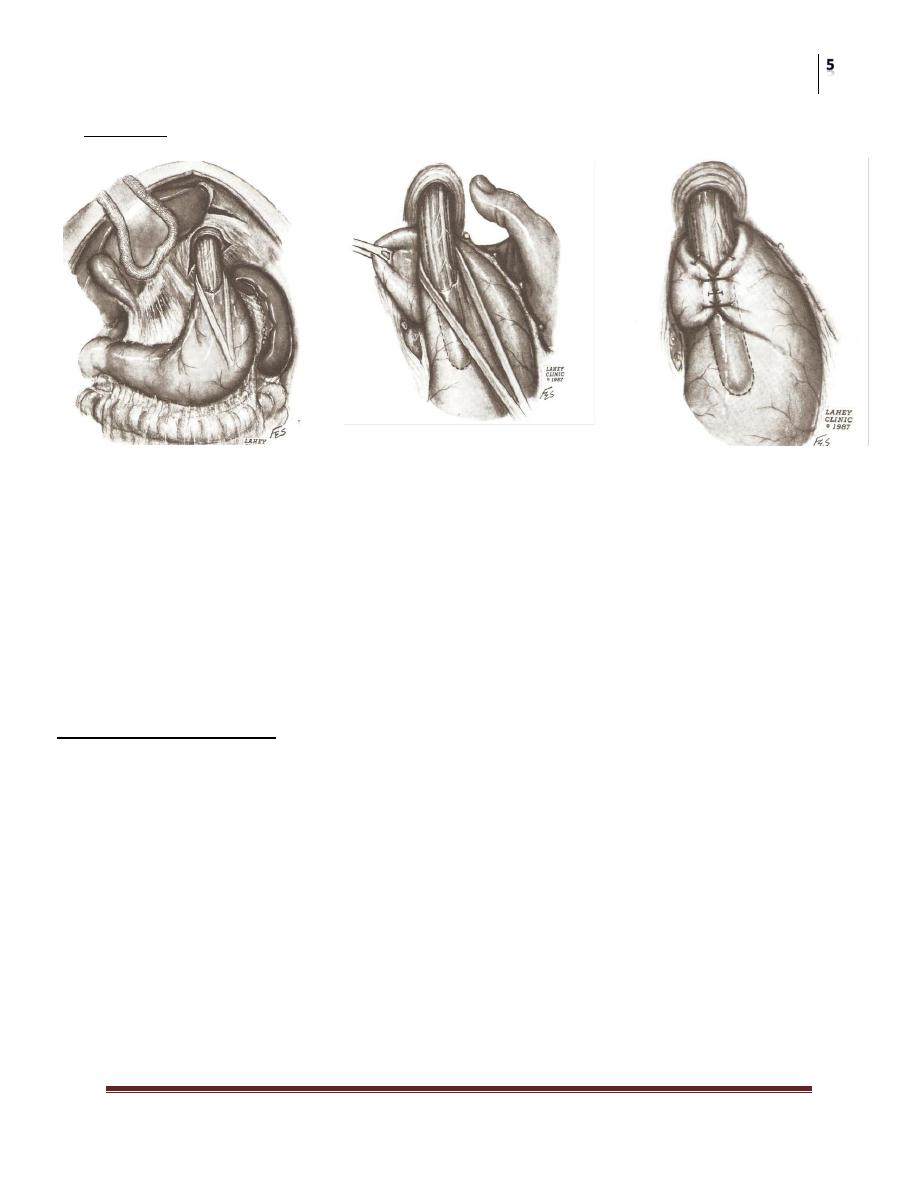
Surgery:
a. Laparoscopic Nissen‘s fundoplication.
b. Lapratomy Nissen‘s fundoplication.
c. Thoracotomy Belsy’s mark 1V repair.
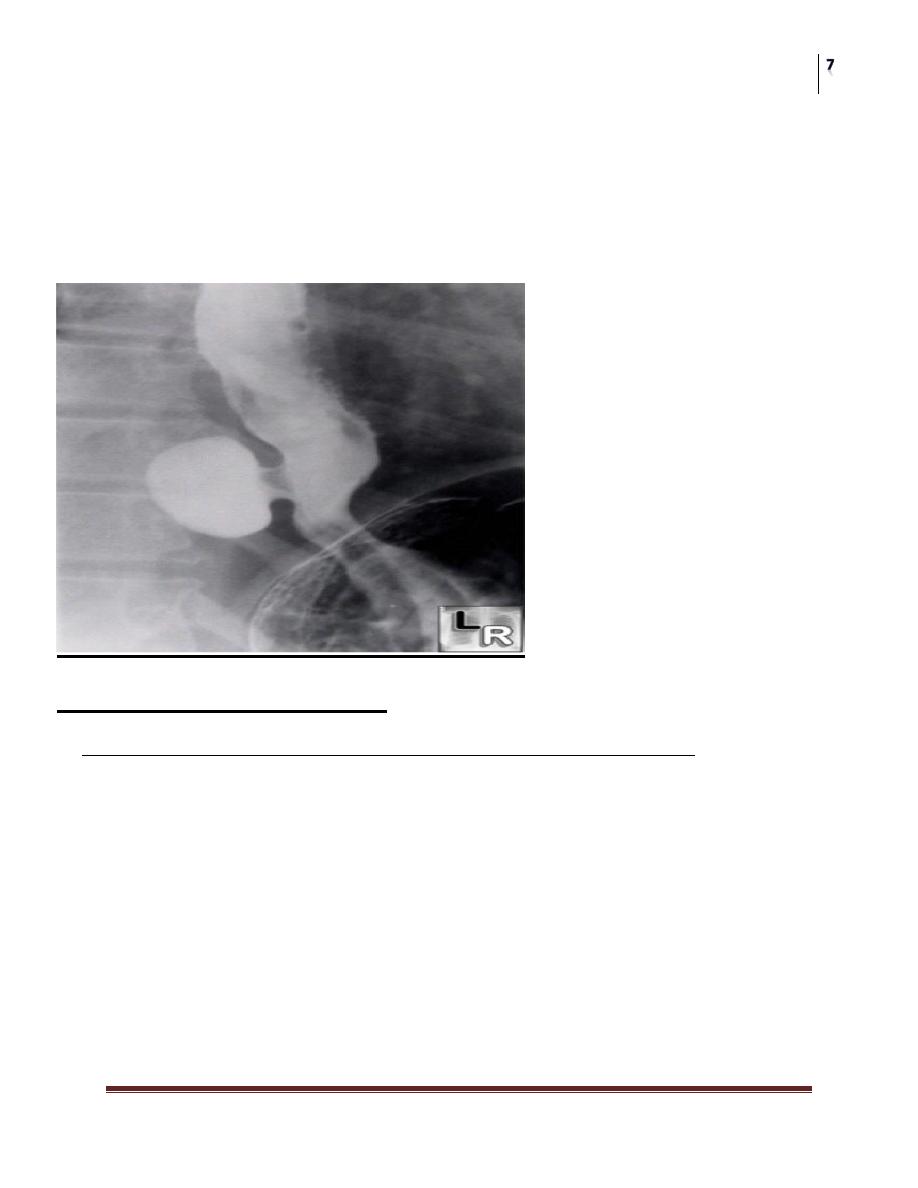
Esophageal hiatal hernia
It is the herniation of the stomach through the esophageal hiatus of the diaphragm.
Hiatal Hernia is of two types:
1. Type 1 axial (sliding H.H.): is common, usually insignificant, in which there are
hiatus opening dilatation and or stretching of phrenoesophageal membrane, so that a
portion of the fundus will slide upward into the hiatus. No true sac.
In some patients a large pouch can occur producing abnormal degree of GE reflux
(significant).
2. The Para-esophageal (rolling): less common but more significant, there is a defect
of phreno –esophageal mm. So this allows protrusion of the peritonium through the
fascia (true hernial sac) .this will lead to progressive enlargement of the hernia .the
Surgery
Esophagus
Prof. Dr. Waleed Mustafa
Lec. 3
entire stomach may herniate. May lead to gastric volvulus, strangulation and
intrathoracic gastric distention.
3. Combined H.H. in which herniation of the cardia well above the diaphragm in
addition to paraesophageal hernia. Increased incidence of reflux.
4. Multiorgan H.H. Other organs herniated (colon, small intestine).
Clinical presentation:
Heart burn &Regurgitation aggravated by posture
Commonly after meal. Dysphagia, Aspiration into the chest can occur often
awaken the patient, can lead to lung abscess.
3. Barium- swallow: in trendelenburg position.
4. Esophagoscopy:
Treatment:
The principal indication for H.H. Repair is paraesophageal type (II) H.H. (Surgery). No
indication for repair of type (I) unless severe reflux.
Medical treatment should start once reflux diagnosed.
Surgical Treatment:
Nissen‘s fundoplication (lapratomy or laparascopic)
Beksy’s mrak IV repair (Thoracotomy)
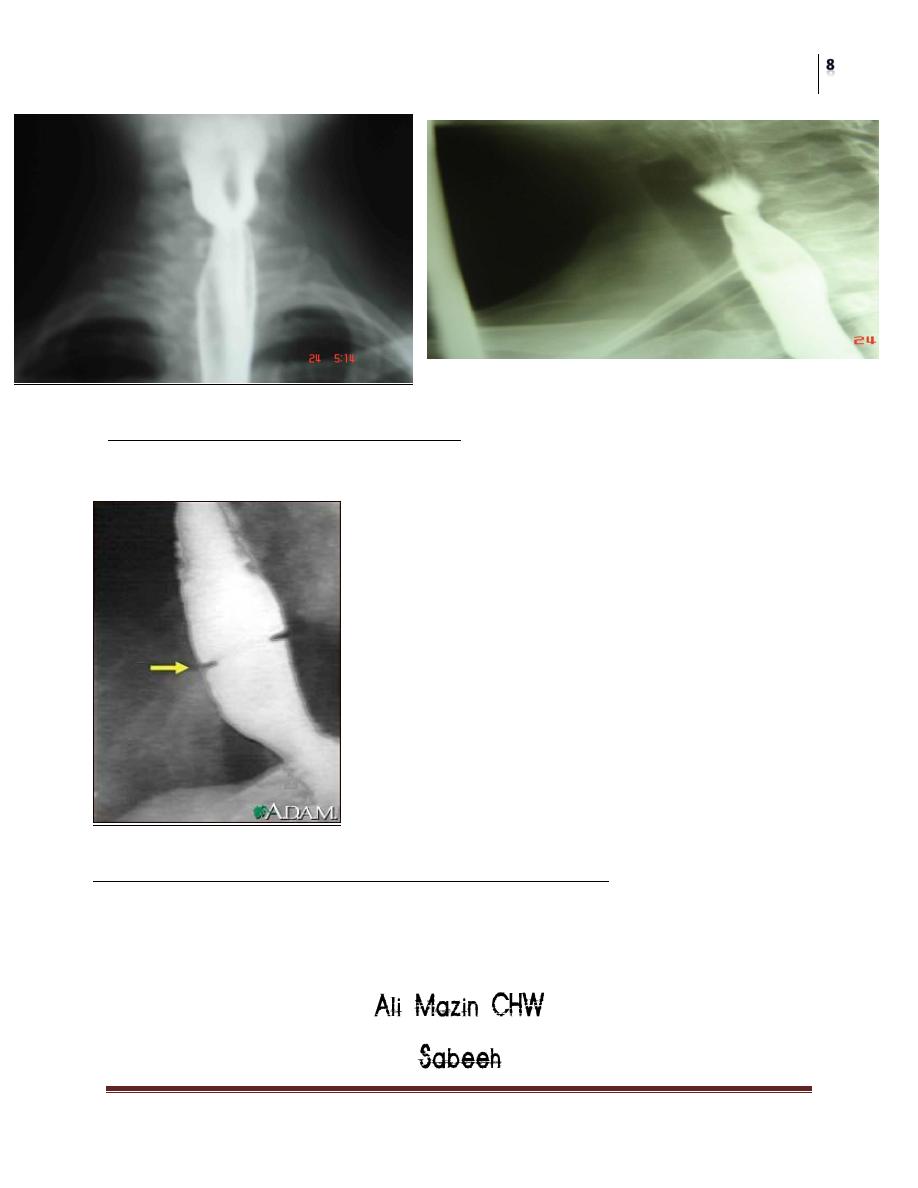
Esophageal divertuculae
Are epithelial -lined mucosal pouches that protrude from the esophageal lumen. Almost
all are acquired and occur predominantly in adults. Classified according to the site:
Surgery
Esophagus
Prof. Dr. Waleed Mustafa
Lec. 3
1. Pharyngo esophageal (at the junction of pharynx &Esophagus.)
2. Parabronchial (midesophageal), near the tracheal bifurcation.
3. Epiphrenic (Supra diaphragmatic) from the distal 10cm of the esophagus.
True diverticulum contains all layers of the normal Esophagus. False = = = consist
primarily of only (mucosa & submucosa)
Miscellaneous conditions
Sideropenic Dysphagia (Plummer-Vinson or Patterson-Kelly syndrome).
1. Cervical dysphagia in patients with iron deffiency .Anemia.
2. Usually edentulous women over the age of (40) years.
3. Have atrophic oral mucosa with glossitis.
4. Brittle spoon-shaped finger nails (Koilonychia.)
5. The presence of a cervical esophageal web.
6. It is regarded as (pre malignant) condition.
Treatment: Dilatation &correction of anemia.
Surgery
Esophagus
Prof. Dr. Waleed Mustafa
Lec. 3
Schatzki‘s Ring ;( Distal esophageal web)
Commonly seen in patient with a sliding H.H.,appearing as annular strictures
projecting into the lumen.
Mallory-Weiss Syndrome; (Emetogenic mucosal laceration)
A history of emesis followed by either melena or hematemesis. May occur in
pregnancy, alcoholism, bowel obstruction.
The END.