Prevention and Management of diabetic foot
byDr. Ammar Tlib Al-yassiri
Prevention:
*The best way of preventing complications is to insist on regular attendance at a diabetic clinic.*full compliance with medication
*examination for early signs of vascular or neurological abnormality. *advice on foot care and footwear and a high level of skin hygiene.
Foot care for the at risk patients
To do list:*Inspect the foot daily using a mirror to see the sole and don’t forget between the fingers.
*Wash feet daily
*Apply lotion to avoid skin cracks and if present skin cracks should be kept clean and covered
*Use a comfortable shoe wear and change it often
*Inspect shoes before wearing it from inside and outside. *Great care is needed with nail trimming
Not to do list:
* Smoking
*Step into bath tub without checking the temperature of the water.
*use hot water bottles or heating pad.
*use keratolytic agent to treat the calluses or corn. *Wearing a tight shoes or stocking.
*walking with barefeet
Management of diabetic foot
For the management of diabetic foot there should be a multidisciplinary team comprising a physician (or endocrinologist) ,orthopaedic surgeon, surgeon, chiropodist and orthotistEvaluation of diabetic foot patient
Peripheral neuropathy:Sensory: Examination for early signs of neuropathy should include the use of
*Semmes-Weinstein hairs (for testing skin sensibility) *Biothesiometer (for testing vibration sense),
*Thermal discrimination test,
*And joint position sense.
Motor: examine for wasting, weakness, absent or diminished tendon reflex, and deformities (claw toes, hammer toes, pes cavus). This can be enhanced by the EMG & N/C study.



Peripheral vascular damage: examine for
the pulses,skin temperature,
trophic changes in the skin and nails
Peripheral vascular examination is enhanced by using
Doppler ultrasound probe,
ankle brachial index measurement,
Absolute toe pressure,
transcutaneous oxygen measurement,
angiography.



Infection: examine for
* the local and systemic signs of infection.* Ulcers must be swabbed for infecting organisms.
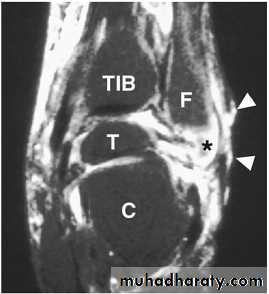
* Magnetic resonance imaging (MRI) is the most specific
and sensitive non-invasive test to evaluate OM and is
also useful for the evaluation of a probable abscess or
sinus tract formation.
* Bone scans, such as the white blood cell labeled Indium-111, Technetium-99m HMPAO and Sulfur Colloid Marrow Scan, may prove beneficial between distinguishing acute and chronic infections, also it is useful for identifying OM from Charcot
neuroarthropathy

Osteopathy: examine for
Charcot deformities (flatening of the foot arches, rocker-bottom deformity, prominent metatarsl heads.X-ray examination may reveal periosteal reactions, osteoporosis, cortical defects near the articular margins and osteolysis - often collectively described as 'diabetic osteopathy
Laboratory investigations
* WBC elevated in 50% of patients. * renal function,
* electrolytes,
* acidosis,
* and blood glucose level.
* Hemoglobin A1C levels provide a barometer of glycemic control averaged over the previous 2-3 months.
* Acute phase reactants ESR &CRP (baseline and post-treatment CRP, ESR and WBC were significantly elevated in patients who ultimately required amputation).
* Total serum protein and albumin, well known as determinants of nutritional status.
* microbiological analysis permits the appropriate selection of antimicrobial therapytreatment
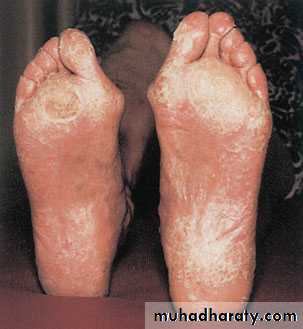
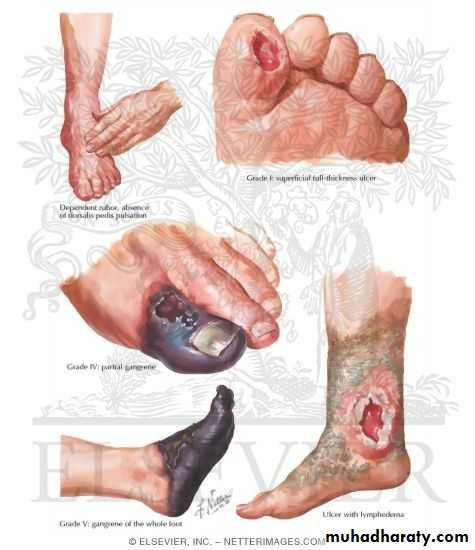
According to wagner classification:Grade 0 (skin intact): calluses should be trimmed so as not mask active ulcer, advise the patient how to do daily foot care and apply the preventive measures.(extra depth shoes and pressure relieving insole)
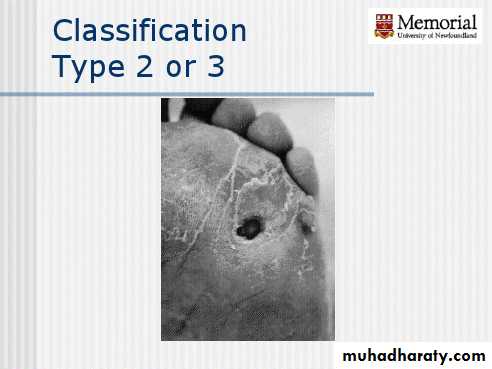
Grade 1&2(superficial & deep ulcer but without infection ): the aim here is to heal the skin, after desloughing the ulcer and removing the hyper keratotic skin the ulcer can be dressed locally, the application of a skin - tight POP(total contact cast) changed weekly will allow most of the ulcers to heal. It also allows the patient to be mobile
Grad 3 (grade2 with infection):
deep infection without abscess formation can be treated by strict rest, elevation, soft tissue support and AB.Occasionally, septicemia calls for admission to
hospital and treatment with intravenous antibiotics.
Any form of abscess formation needs to be drained urgently and the deeper tissues thoroughly debrided.
Deep ulcers in certain sites are more problematic than elsewhere . Once an ulcer is healed the use of appropriate insoles and shoes can prevent further ulceration.
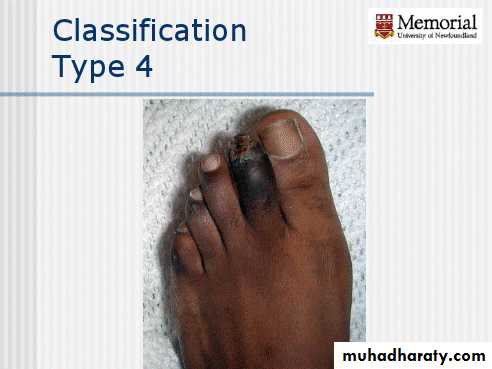
Grade 4(localized gangrene):
Ischaemic changes need the attention of a vascular surgeon who can advise on ways of improving the local blood supply. Arteriography may show that bypass surgery is feasible.
Dry gangrene of the toe can be allowed to demarcate before local amputation.
With diabetic gangrene septic arithritis is not uncommon , the entire ray(toe+metatarsal bone ) should be amputated.
In More extensive gangrene partial foot amputation done e.g. through the midtarsal joints(Chopart),thruogh tarsometatarsal joints(lisfranc), thruogh metatarsal bone, syme’s amputation
Grade 5(Global foot gangrene) :
severe occlusive disease with wet gangrene may call for immediate amputation.This should be undertaken at a level where there is a realistic chance of the wound healing.
Treatment of special problems
Ischaemic changes : need the attention of a vascular surgeon who can advise on ways of improving the local blood supply. Arteriography may show that bypass surgery is feasible.Insufficiency fractures: should be treated, if possible, without immobilizing the limb; or, if a cast is essential, it should be retained for the shortest possible period.
Fixed foot deformities : corrective surgery should be considered.
Neuropathic joint disease : is a major challenge.
Arthrodesis is fraught with difficulty, not least a very poor union rate, and sometimes is simply not feasible. 'Containment' of the problem in a weight-relieving orthosis may be the best option.