Renal trauma
Dr.Mohammed Bassil4/10/2015
1
classification and grading
Blunt injures ::::1 Direct blow to the kidney:
a fall, assault, or sports injury
2 Rapid deceleration:
Because the renal pedicle is the site of attachment of kidney to other fixed retroperitoneal structures, renal vascular injuries (tears or thrombosis) or UPJ disruption may occur.
4/10/2015
2Penetrating injuries::::
1-Stab or gunshot injuries.
2-Half of patients with penetrating trauma and hematuria have grade III, IV, or V renal injuries.
4/10/2015
3
clinical and radiologicalassessment
History :::: mechanism of the trauma.Examination:
1-Pulse rate, systolic blood pressure, respiratory rate.
3-location of entry exit wounds, flank bruising, and rib fractures need to be assessed.
3-The lowest recorded systolic blood pressure.
4/10/2015
4
Indications for renal imaging
1-Gross hematuria2- Microscopic Hematuria in a hypotensive patient .
4-History of rapid deceleration .
(e..g., fall from a height, high-speed motor vehicle accident).
5- Penetrating chest and abdominal wounds (knives, bullets) with any degree of hematuria or suspicion of renal injury based on wound location.
6- Any child with urinalysis showing microscopic hematuria after blunt trauma
4/10/2015
5
Degree of hematuria
The relationship between the presence, absence, and degree of hematuria and the severity of renal injury is neither predictable nor reliable.4/10/2015
6
Staging of the renal injury
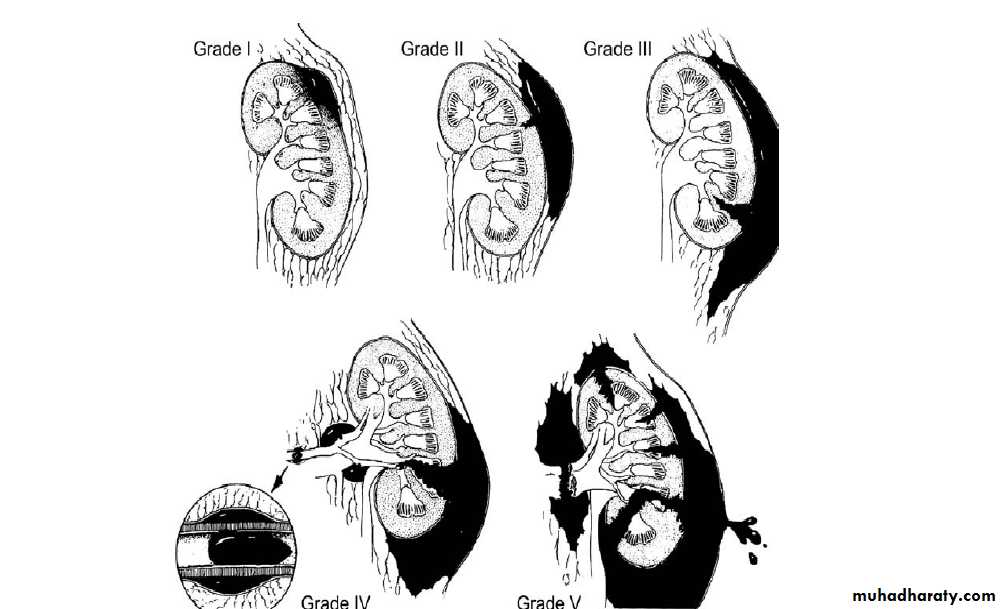
Using CT, renal injuries are staged according to the American Associationfor the Surgery of Trauma (AAST) Organ Injury Severity Scale. Higher injury severity scales are associated with poorer outcomes.
Grade I Contusion or subcapsular hematoma with no parenchymal
laceration
Grade II Parenchymal laceration of cortex <1 cm deep, no extravasation of urine (i.e., collecting system intact)
Grade III Parenchymal laceration of cortex >1 cm deep, no extravasation of urine (i.e., collecting system intact)
Grade IV Parenchymal laceration involving cortex, medulla, and collecting system OR segmental renal artery or renal vein injury with contained hemorrhage.
Grade V Completely shattered kidney OR avulsion of renal hilum.
4/10/2015
7
4/10/2015
8The hemodynamically unstable patient
In this situation, an intraoperative on-table IVP is indicated if:• A retroperitoneal hematoma is found and/or
• A renal injury is found that is likely to require nephrectomy.
4/10/2015
9

4/10/2015
10Renal CT with IV contrast in blunt trauma patent shows a
superfi cial (grade 2) laceration amenable to nonoperative management.
Treatment
Conservative (nonoperative) management::::
• Most blunt (95%) and many penetrating renal injuries (50% of stab injuries and 25% of gunshot wounds) can be managed nonoperatively.
4/10/2015
11
Treatment
Dipstick or microscopic hematuria:If systolic BP since injury has always been >90 mmHg and there is no history of deceleration, imaging and admission is not required. Outpatient follow-up of microhematuria should be considered.
4/10/2015
12
Treatment
Gross hematuria: In a hemodynamically stable patient:High-grade injuries can be managed nonoperatively if they are cardiovascularly stable.
However, grade IV and, especially, grade V injuries may require prompt nephrectomy to control bleeding . (grade V injuries function poorly if repaired).
4/10/2015
13
Treatment
Surgical exploration:::
This is indicated ( blunt or penetrating injury) if
1- Expanding, large, or pulsatile perirenal hematoma is present (suggests a renal pedicle avulsion; hematuria is absent in 20%).
2- The patient develops shock that does not respond to resuscitation with fluids and/or blood transfusion.
3- The hemoglobin decreases (there are no strict definitions of what represents a significant fall in hemoglobin).
4- There is urinary extravasation and associated abdominal injury.
4/10/2015
14

4/10/2015
15Left renal artery thrombosis after blunt trauma resulting in devitalized parenchyma successfully treated non operatively.

4/10/2015
16
deep central renal laceration and large perirenal hematoma with intravascular contrast extravasation
Treatment
Nephrectomt:::::For severe renal injuries producing life-threatening bleeding, prompt nephrectomy is warranted.
These are usually unstable patients who persist in shock despite multiple transfusions and have deep renal lacerations near the hilum
4/10/2015
17Ureteral injuries
4/10/201518
mechanisms and diagnosis
External:::• nearly always due to penetrating trauma.
• rarely due to blunt trauma.
• pelvic or abdominal surgery
4/10/2015
19
Diagnosis
External injury: diagnosis:::• wound location.
• In stable patients, contrasted CT with delayed cuts (10–20 minutes) is superior to IVP for clearly determining the presence of a ureteric injury.
• Retrograde pyelography.
4/10/2015
20
Iatrogenic injury: diagnosis:::
The injury may be suspected at the time of surgery, but injury may not become apparent until some days or weeks postoperatively.4/10/2015
21
Intraoperative diagnosis:::
• Direct inspection of the ureter.• IV injection of methylene blue or indigo carmine may reveal a laceration.
• Direct injection into the ureter, either retrograde or antegrade, may also reveal extravasation from a laceration.
• Discoloration of the ureter observed during laparotomy suggests ischemic injury .
4/10/2015
22
Postoperative diagnosis:::
1- Symptoms and signs of ureteral injury::These may include the following:
• Ileus (due to urine within the peritoneal cavity)
• Prolonged postoperative fever or overt urinary sepsis
• Drainage of fluid from drains, abdominal wound, or vagina. Send
aliquot for creatinine estimation. Creatinine level higher than that
of serum = urine (creatinine level will be at least 300 μmol/L
[4.0 mg/dL]).
• Flank pain if the ureter has been ligated
• Abdominal mass, representing a urinoma
• Vague abdominal pain
• The pathology report on the organ that has been removed may note
presence of segment of ureter.
4/10/2015
23
• 2-Investigation ::
Ultrasonography may demonstrate hydronephrosis, but hydronephrosismay be absent when urine is leaking from a transected ureter into the retroperitoneum or peritoneal cavity.
IVP may show an obstructed ureter or possibly a contrast leak from the site of injury,
4/10/2015
24
CT with delayed film.
Retrograde pyelogram is an accurate method of delineating the site of injury, but is best used in conjunction with attempted stent placement.4/10/2015
25
Ureteral injuries: management
When to repair the ureteral injury:• In general, the best time to repair the ureter is as soon as the injury has been diagnosed (if intraoperatively), or if the diagnosis is made within the first week after injury.
• Delay definitive ureteral repair when:
• The patient is unable to tolerate a prolonged procedure under general anesthesia.
• There is evidence of active infection at the site of proposed ureteral repair (infected urinoma).
• Diagnosis is made more than 14 days after injury.
4/10/2015
26
Definitive treatment of ureteral injuries
The options depend on the following:• Whether the injury is recognized immediately.
• The nature and level of injury.
• Other associated problems.
4/10/2015
27
The options are as follows
• JJ stenting for 3–6 weeks.• Primary closure of partial transection of the ureter and stent placement.
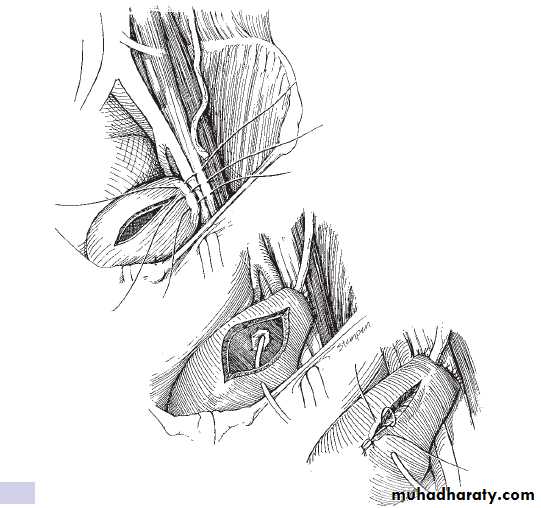
• Direct spatulated anastomosis (primary ureteroureterostomy).
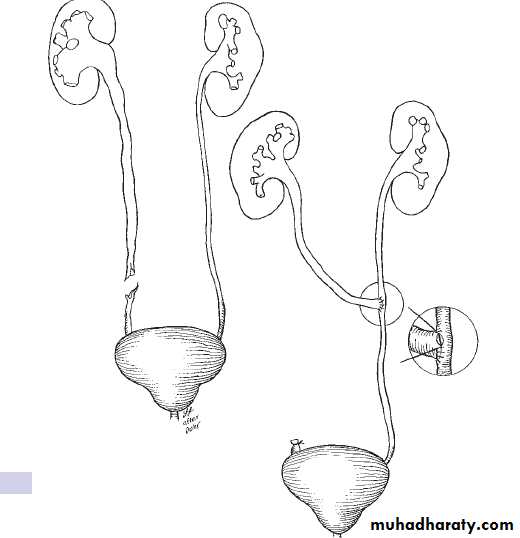
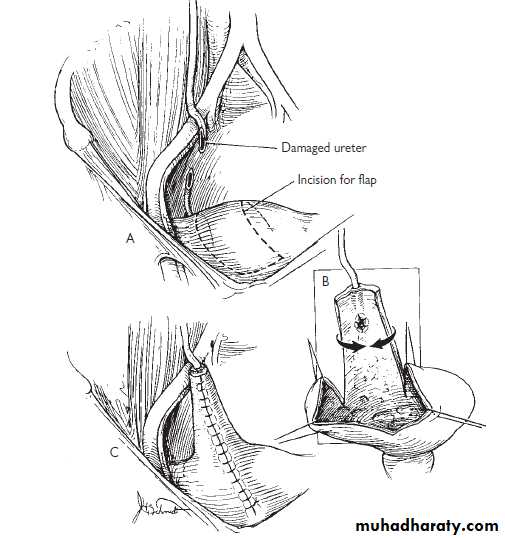
• Reimplantation of the ureter into the bladder (ureteroneocystostomy), or with psoas hitch and/or a Boari bladder flap.
• Transureteroureterostomy.
• Replacement of the ureter with ileum.
• Autotransplantation of the kidney into the pelvis.
• Permanent cutaneous ureterostomy .
• Nephrectomy.
4/10/2015
28
4/10/2015
29
4/10/2015
30