Current Guidelines forAsthma Treatment Ass.Prof.Dr:MUHAMMED WAHEEB AL,OBAIDYConsultant Chest Physician MEDICAL CITY
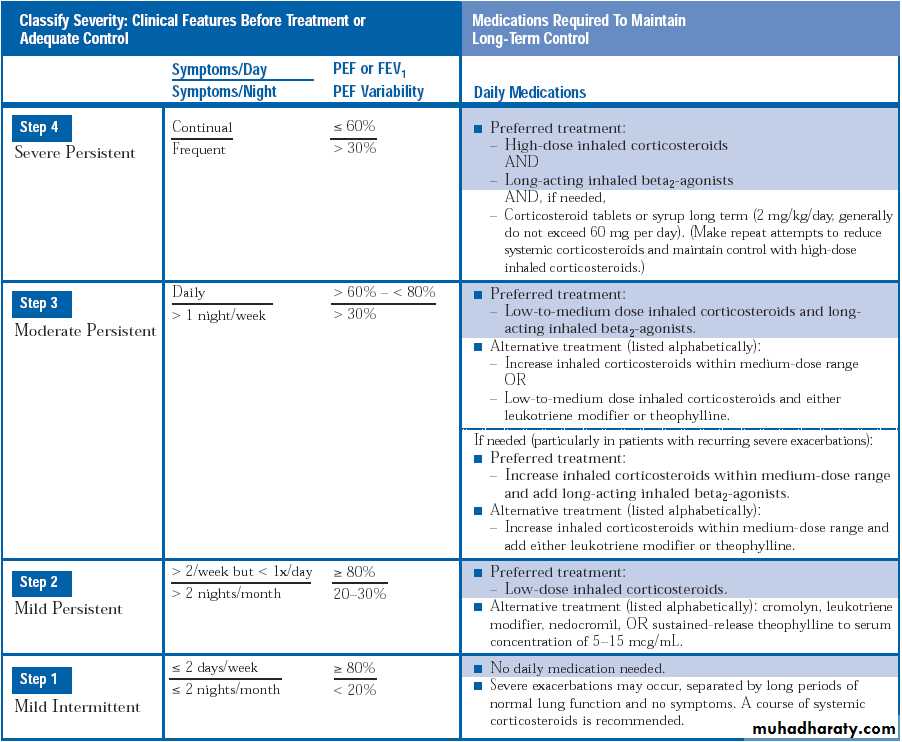
Mild Intermittent Asthma
Symptoms < 2 days/weekSymptoms < 2 nights/month
PEF or FEV1 > 80%
PEF variability < 20%
No daily medication needed
PRN beta agonists
Course of systemic steroids for exacerbations
Mild Persistent Asthma
Symptoms > 2 days/wk but < 1x/day> 2 nights/month
PEF or FEV1 > 80%
PEF variability 20-30%
Preferred treatment low dose inhaled corticosteroids
Alternatives include cromolyn, leukotriene modifiers, necromodil, or sustained release theophylline
Moderate Persistent Asthma
Symptoms daily
> 1 night/week
PEF or FEV1 > 60% and < 80%
PEF variability > 30%
Preferred treatment is low to medium dose inhaled corticosteroid and a long acting inhaled beta 2 agonist
Alternative includes increasing ICS within moderate dose range, or low to medium dose ICS with either leukotriene modifier or theophylline
Severe Persistent Asthma
Continual symptomsFrequent nocturnal attacks
PEF or FEV1 < 60%
PEF variability > 30%
Preferred treatment is high dose inhaled corticosteroid and long acting beta 2 agonists
If needed, can add systemic corticosteroids
Goals of Therapy
Minimal or no chronic symptoms day or nightMinimal or no exacerbations
No limitations on activities; no school/work missed
Maintain (near) normal pulmonary function
Minimal use of short-acting inhaled beta 2 agonist
Minimal or no adverse effects from medications
Stepwise Approach
Review treatment every 1 to 6 months, and gradually step down treatment
If asthma controlled not maintained, then a step up in treatment may be warrantedReasons for Poor Asthma Control
Inhaler TechniqueCompliance
Environment
Also assess for an alternative diagnosis
“All that wheezes is not asthma, and not all asthma wheezes”
Factors Affecting Compliance
EducationRoute of drug administration (inhaled vs. oral)
Complexity of drug regimens
Side effects of medications
Cost
Beta 2 Agonists
Beta 2 Agonists
Most potent and rapidly acting bronchodilators currently available for clinical use
Given in different forms:
short acting = isoproterenol
intermediate acting = albuterol, levalbuterol ,pirbuterol,metaproterenol, terbutaline, fenoterol
long acting = salmeterol, formoterol
Mechanism of Action
Beta 2 agonists interact with beta 2 receptors on the surface of a variety of cells that may play a role in asthma pathogenesisBeta agonists have the potential to relax bronchial smooth muscle,
Also B2 agonist :
Decrease mast cell mediator releaseInhibit neutrophil, eosinophil, and lymphocyte functional responses
Increase mucociliary transport
Affect vascular tone and edema formation
MDI with Spacer vs. Nebulizer
Equivalent bronchodilation can be achieved by giving beta 2 agonist with a spacer/holding chamber or by nebulizer therapyContinuous administration with a nebulizer may be more effective in severely obstructed adults and in those who have difficulty with an MDI plus spacer
Chronic Use of Beta Agonists
Arguments against chronic use:
Mortality may be increased
Control of asthma may worsen
Equal or superior efficacy can be achieved with inhaled corticosteroids
Increased Mortality with Chronic Use?
A case-control study using linked health insurance databases found:Increased risk of death or near-death from asthma was associated with the regular use of inhaled beta agonists, especially fenoterol
Did not appear to be confounded by asthma severity, and there was no relation to non–asthma mortality
Increased Mortality with Chronic Use?
However, increased odds ratios were also noted for theophylline and oral corticosteroidsIncreased Mortality with Chronic Use?
A subsequent analysis demonstrated a relationship between CV death and use of beta agonists taken orally or by nebulizer but not when taken by MDIRisk of CV death was also greater in patients who used theophylline
Most of CV deaths in patients with underlying CV disease, including acute coronary insufficiency and congestive cardiomyopathy*
Long Acting Beta Agonist Monotherapy
Prolonged treatment with long-acting beta agonists and without inhaled corticosteroids has been associated with increased mortality28-week placebo-controlled trial assessing the safety of the long-acting beta agonist salmeterol enrolled over 25,000 patients, but was stopped early when interim analysis revealed a significantly increased risk of death in those not taking concomitant inhaled corticosteroids .
*"The Pink Sheet" FDC Reports. Chevy Chase, MD. 2003; 65(4):10
Tolerance to Beta Agonists
More frequent in chronic use
Induced more with oral rather than inhaled preparations
Tolerance to long acting beta agonists may or may not occur (conflicting data)
Corticosteroids
GlucocorticoidsMost potent antiinflammatory agents available for the treatment of asthma
More effective than beta agonists, theophylline, and cromolyn sodium in reducing airway hyperresponsiveness during maintenance therapy
Glucocorticoid Mechanisms
Alleviating airway inflammationReducing collagen and tenascin deposition, two features associated with airway remodeling
Inhibit the synthesis of almost all known cytokines
Alteration of the number and availability of circulating leukocytes
Reduction in vascular permeability
Inhibition of mediator synthesis and release
Steroids and Long Acting Beta Agonists
Results in greater improvements in lung function and symptom control than monotherapy with escalating doses of inhaled glucocorticoidAct synergistically to activate transcription factors, decrease smooth muscle proliferation, and impair eosinophil adhesion
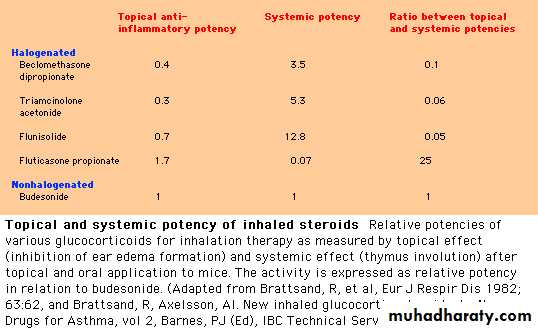
Potency of Inhaled Corticosteroids
COMBINATION INHALERS
There is no difference in effi cacy in giving inhaled steroid and long-acting β2 agonist in combination or in separate inhalers.Once a patient is on stable therapy, combination inhalers have the advantage of guaranteeing that the long-acting β2 agonist is not taken without inhaled steroid.
In adult patients at step 3 who are poorly controlled, the use of budesonide/formoterol in a single inhaler as rescue medication instead of a short-acting β2 agonist, in addition to its regular use as a controller treatment, has been shown to be an effective treatment option.
This management technique has not been investigated with other combination inhalers
Can ICS Cause Osteoporosis?
Three year prospective study looked at dose of inhaled triamcinolone and rate of bone loss in premenopausal women with asthmaThere was a dose-related decline in bone density in the total hip and trochanter
No dose-related decline in the femoral neck or spine