Diseases of the Pleura Lecture 2
Dr.Mustafa Nema. Baghdad College of Medicine 2013Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Case 1A 28 years old previously healthy female presented with sudden onset of localized right sided chest pain and feeling of shortness of breath.
OE: looks in pain, RR 22, PR 125. normal BP and Temp.
CXR shown
What’s your primary diagnosis?
What’s your treatment plan?
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
case 1
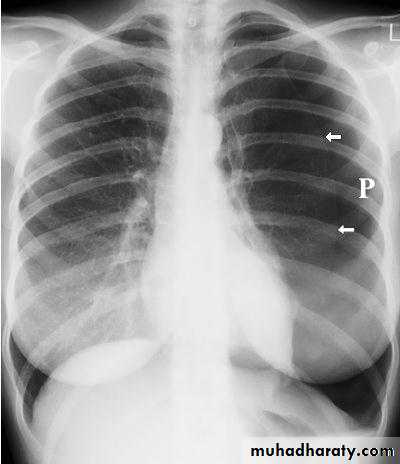
The chest X-ray shows thesharply defined edge
of the deflated lung with
complete translucency
(no lung markings)
between this and the
chest wall.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Case 2
A 56 years-old smoker man with history of COPD, presented with acute dyspnea and right sided chest pain. He looks distressed, cyanosed with PR 110, BP 90/60, RR 36, Temp 36.7.ECG: sinus tachycardia. No ischemic changes.
CXR seen.
What is your diagnosis?
What will you find on chest exam?
What is your management plan?
Is there any other important differential Diagnoses before viewing CXR?
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
PNEUMOTHORAXDiseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
PNEUMOTHORAX• Pneumothorax (PNX) is the presence of air in the pleural space.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Types of PNX
According to:
Presence or absence of external cause:
• Spontaneous PNX ( no external cause)
Primary
Secondary
• Traumatic PNX ( external cause + )
Presence or absence of valvular mechanism between the lung and the pleural space:
• Closed PNX
• Open PNX
• Tension PNX
Presence of different types of fluid with the air:
• Hydro- PNX ( usual pleural effusion)
• Haemo- PNX ( bloody effusion)
• Pyo-PNX ( pus=purulent effusion)
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Spontaneous:
Primaryoccur without evidence of overt lung disease. Air escapes from the lung into the pleural space through rupture of a small subpleural emphysematous bulla or pleural bleb.
It principally affects males aged 15-30 in whom smoking, tall stature and the presence of apical subpleural blebs are additional risk factors.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Bulla (bleb) on the lung apex

Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
lungChest wall
bleb
SecondaryOccurs in patients with underlying lung disease. This includes patients with:
Chronic obstructive pulmonary disease (COPD)
Cystic fibrosis
Chronic interstitial lung disease such as idiopathic pulmonary fibrosis
Malignancy.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Traumatic pneumothoraxOccurs when the lung is punctured by:
A needle - during procedures such as insertion of a central line or lung biopsy
Blunt force injury - for example, in a road traffic accident or fracturing a rib
Mechanical ventilation - when this is the cause of a traumatic pneumothorax, the pneumothorax may rapidly worsen because mechanical ventilation increases alveolar pressures
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Closed and open PNX
Where the communication between the lung and pleural space seals off as the lung deflates and does not reopen, the pneumothorax is referred to as 'closed PNX’.
In such circumstances the mean pleural pressure remains negative, spontaneous reabsorption of air and re-expansion of the lung occur over a few days or weeks, and infection is uncommon..
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013

Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Closed PNXMean pleural pressure is negative
_ _
'Open PNX’ occurs when the communication fails to seal and air continues to transfer freely between the lung and pleural space.
An example of the latter is a bronchopleural fistula which, if large, can also facilitate the transmission of infection from the air passages into the pleural space, leading to empyema.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013

Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Open PNXMean pleural pressure atmospheric
Broncho-pleural fistula
An open pneumothorax is commonly seen following rupture of an emphysematous bulla, tuberculous cavity or lung abscess into the pleural space.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Tension pneumothorax occur when equilibrium fails to be established.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Air continuously inter pleural spaceAir pushing mediastinum to other side
Tension PNX
Mean pleural pressure positive
+++If the communication between the airway and the pleura is small, it can act as a one-way valve allowing air to enter the pleural space during inspiration but not to escape on expiration.
Large amounts of trapped air accumulate in the pleural space and the intrapleural pressure may rise to well above atmospheric levels (a so-called 'tension' pneumothorax)..
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Clinical features
The commonest symptoms are sudden-onset unilateral pleuritic chest pain or breathlessness.
In those with underlying chest disease, breathlessness can be severe and may not resolve spontaneously.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
On examination
In patients with a small PNX the physical examination may be normal.A larger pneumothorax results in decreased or absent breath sounds.
The combination of absent breath sounds and resonant percussion note is diagnostic of pneumothorax
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
In tension PNX, the findings are progressive breathlessness associated with a marked tachycardia, hypotension, cyanosis and tracheal displacement away from the side of the silent hemithorax.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Tension PNX rapidly causes mediastinal shift and, if untreated, will lead to impaired venous return and cardiovascular collapse.
Death from respiratory or cardiovascular collapse may occur.
Occasionally, 'tension' PNX may occur without mediastinal shift if malignant disease or scarring has splinted the mediastinum
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Investigations
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
The chest x ray
When you suspect that a patient has a tension pneumothorax and the patient is about to go into cardiovascular or respiratory failure, you cannot delay treatment by requesting a chest x ray. You must start treatment based on your examination alone.In most patients, there is time to obtain a chest x ray.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
The purpose of this x ray is to:
Confirm the clinical diagnosisAllow you to estimate the size of the pneumothorax
Potentially allow you to identify underlying disease of the lung parenchyma - you can then classify the pneumothorax as secondary.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
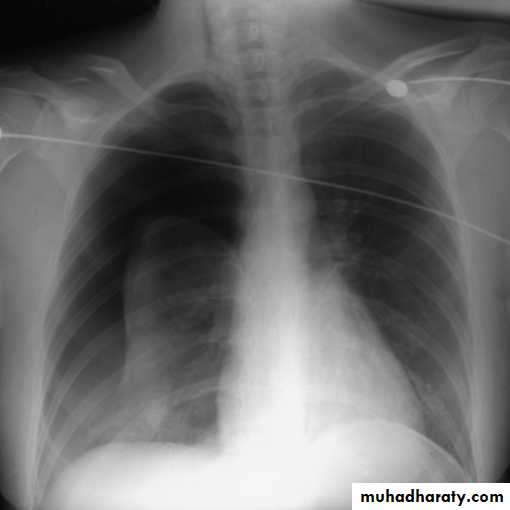
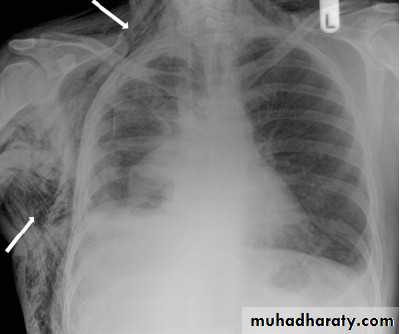
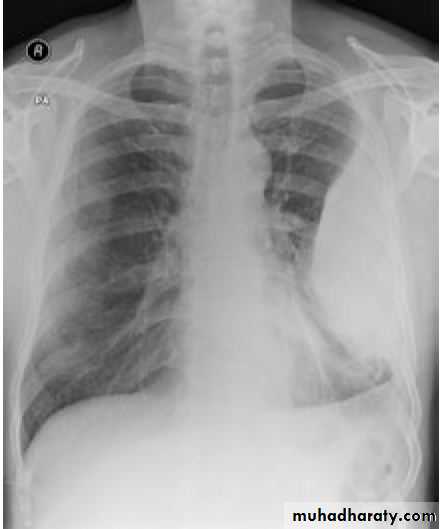
This frontal CXR reveals complete collapse ofthe right lung due to a massive right pneumothorax, which is also shiftingthe heart and other mediastinal structures to the left, (a tension pneumothorax).

Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
PNX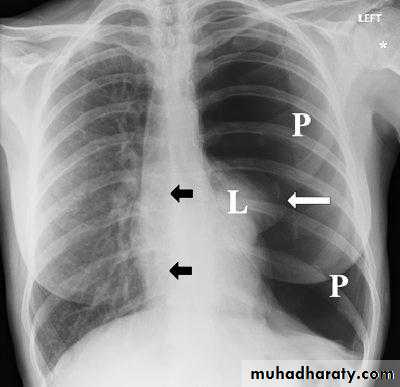
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Surgical emphysema may complicate PNX when air escape to subcutaneous tissuesDiseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
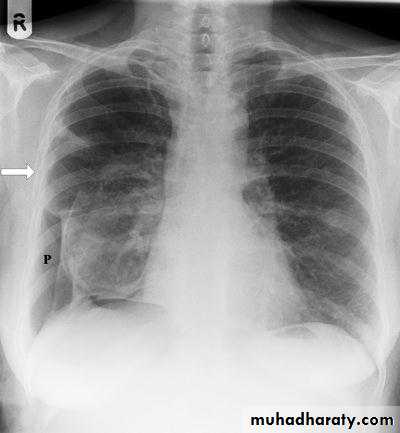
PNX in
Diseased lung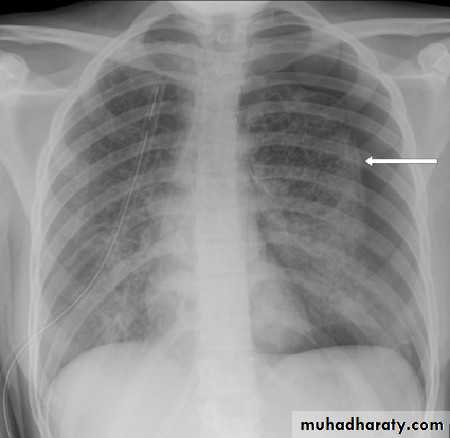
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
A lateral (or decubitus) projection is recommended if the initial chest x ray is inconclusive.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
CT
You should be able to diagnose and manage most pneumothoraxes through chest x ray.
Where radiography is not definitive and clinical suspicion is high, a CT scan may be needed.
If you are unable to distinguish between a pneumothorax and large bulla on the basis of the chest x ray, you may need to request a CT scan.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
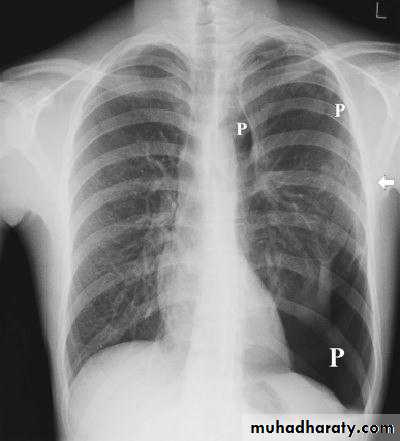
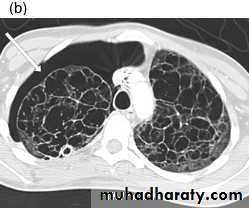
PNX inCystic lung
disease
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
CT adds information regarding the presence or absence of pleural fluid and underlying pulmonary disease.Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
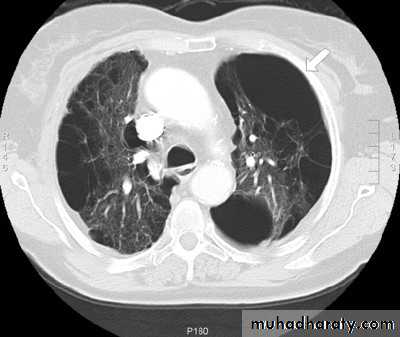
emphysematous bulla (not PNX)
TreatmentTwo main modalities: needle aspiration or intercostal chest tube drain. Less frequently surgery may be indicated.
The principal factors determining the mode of therapyare:
Patient symptomsThe size of the pneumothorax
The presence of underlying parenchymal lung disease.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
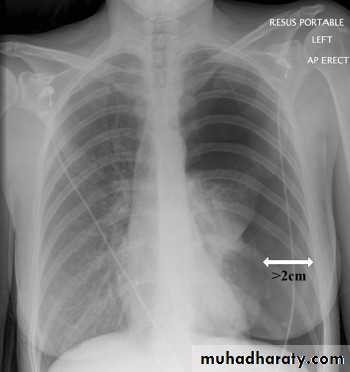
Patient symptomsPrimary pneumothorax where the lung edge is less than 2 cm from the chest wall and the patient is asymptomatic, normally resolves without intervention.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
When a patient is significantly symptomatic with breathless , a drainage procedure is always indicated, regardless of whether the pneumothorax is primary or secondary.
All patients should receive supplemental oxygen as this accelerates the rate at which air is reabsorbed by the pleura.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
In young patients presenting with a moderate or large spontaneous primary pneumothorax, percutaneous needle aspiration of air is a simple and well-tolerated with a 60-80% chance of avoiding the need for a chest drain.Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Size of PNX (small or large?)
The British Thoracic Society guidelines define a small pneumothorax as less than 2cm distance from the lung edge to the chest wall, and a large pneumothorax as equal to or more than 2cm.A two centimetre pneumothorax corresponds to a volume loss of 50%, and is regarded as an objective indication for treatment.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
The presence of underlying parenchymal lung disease
In patients with underlying chronic lung disease, however, even a small secondary pneumothorax may cause respiratory failure; hence all such patients require intercostal tube drainage and inpatient observation.
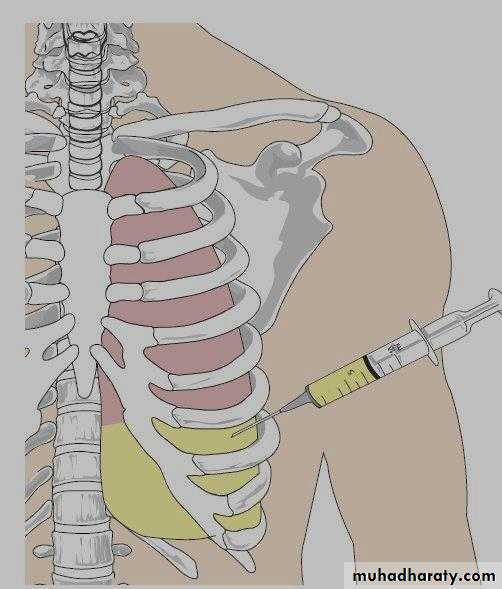
When needed, intercostal drains should be inserted in the 4th, 5th or 6th intercostal space in the mid-axillary line.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
indication for surgery:
Lung not fully reinflatedBronchopleural fistula
Recurrent PNX especially secondary one.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Note:Patients with a closed pneumothorax should not fly as the trapped gas expands at altitude.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Recurrent spontaneous PNX
After primary spontaneous pneumothorax, recurrence occurs within a year of either aspiration or tube drainage in approximately 25% of patients, and should prompt definitive treatment.Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
EMPYEMA
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013This term describes the presence of pus in the pleural space.
Microscopically, neutrophil leucocytes are present in large numbers.The causative organism may be isolated from the pus.
An empyema may involve the whole pleural space or only part of it ('loculated' or 'encysted' empyema) and is almost invariably unilateral.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Aetiology
Empyema is always secondary to infection in a neighbouring structure, usually the lung.The principal infections are the bacterial pneumonias and TB.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013Causes of empyema
'Para-pneumonic' effusion:• - Over 40% of patients with community-acquired pneumonia develop an associated pleural effusion ('para-pneumonic' effusion) and about 15% of these become secondarily infected and empyema may developed.
Infection of a haemothorax
Rupture of a subphrenic abscess through the diaphragm.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
The pus in the pleural space is often under considerable pressure and if the condition is not adequately treated pus may rupture into a bronchus causing a bronchopleural fistula and pyopneumothorax developed.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Clinical features
An empyema should be suspected in patients with pulmonary infection if there is persistence or recurrence of fever despite the administration of a suitable antibiotic.Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Once an empyema has developed, two separate groups of clinical features are found:
• Systemic and local.• systemic
Pyrexia, usually high and remittent
Rigors, sweating, malaise and weight loss
Polymorphonuclear leucocytosis, high CRP
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Local featuresPleural pain
Breathlessness
Cough and sputum usually because of underlying lung disease; copious purulent sputum if empyema ruptures into a bronchus (bronchopleural fistula)
Clinical signs of fluid in the pleural space
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Radiological picture
Chest X-RayThe appearances are often indistinguishable from those of pleural effusion.
D-shape opacity -if present- is characterestic
When air is present in addition to pus (pyopneumothorax), a horizontal 'fluid level' marks the interface between the liquid and air.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
D-shape opacity in epyema
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Pyopneumo-thoraxFluid level present

Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Ultrasound
Ultrasound shows the position of the fluid, the extent of pleural thickening and whether fluid is in a single collection or multiloculated by fibrin and debris.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
CT scanIn addition to showing the pleura, CT can be useful in assessing the underlying lung parenchyma and patency of the major bronchi.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Aspiration of pusThis confirms the presence of an empyema. Ultrasound or CT is recommended to identify the optimal place to undertake aspiration, which is best performed using a wide-bore needle.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
The pus is frequently sterile when antibiotics have already been given; the distinction between tuberculous and non-tuberculous disease can be difficult and often requires pleural histology and culture.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Management Treatment of non-tuberculous empyema
The only way in which an empyema can heal is by eradication of the infection, obliteration of the empyema space and apposition of the visceral and parietal pleural layers.
This cannot occur unless re-expansion of the compressed lung is secured at an early stage by removal of all the pus from the pleural space.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
When the patient is acutely ill and the pus is thin an intercostal tube should be inserted into the most dependent part of the empyema space and connected to a water-seal drain system.Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Although intrapleural fibrinolytic therapy is widely used in such situations, trial evidence of its benefit is conflicting.Antibiotic directed against the organism causing the empyema should be given for 2-4 weeks.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
An empyema can often be aborted if these measures are started early. If, however, the intercostal tube is not providing adequate drainage, which can happen when the pus is thick or loculated, surgical intervention is required.Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Treatment of tuberculous empyema
Antituberculosis chemotherapy must be started immediately and the pus in the pleural space aspirated. Intercostal tube drainage is often required.In many patients no other treatment is necessary but surgery is occasionally required to ablate a residual empyema space.
Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Empyema

Diseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013
Thank youDiseases of the Pleura Dr.Mustafa Nema. Baghdad College of Medicine 2013