AFTER MID
SURGERY
DR. Mahmood Kdhier
Orthopaedic
The painful foot
Dr.Mahmood Khdier
LECTURE 7

The painful foot
Pain is usually well localized to a single area that can be the heel, midtarsal region or
the forefoot.
A. The painful heel:
In children the most likely cause is Sever’s disease (apophysitis). It is not really a
disease but a mild traction injury occurring in boys around 10 years. Pain and
tenderness are localized to the tendo Achilles at is insertion. The heel of the shoe
should be raised a little and strenuous activities restricted for a few weeks.
In adolescent girls a calcaneal knob is common. The posterlateral portion of the
calcanium is too prominent and the shoe rubs on it causing pain. If attention to
footwear does not help, the bony knob is removed.
Young adults sometimes develop pain above the heel. The tendo Achilles is
thickened and tender. It is common in athletes and is due to a peritendinitis. The
acute form may be relieved by rest, ice packs and strapping. The chronic form
may need operation to divide the tendon sheath and fascia; if there is a necrotic
area in the tendon, this may need excision.
Acute Plantar fasciitis: Pain is under the heel and sharply localized tenderness
may occur in gout or in Reiter’s disease, or Rh. arthritis. It is due to inflammation
of the tough ligamentous tissue inserting into the undersurface of the calcanium
(the planter fascia of the foot). The underlying disorder should be treated and the
painful area protected from uneven pressure.
Older adults (40-60 years) may also develop a painful plantar fasciitis usually less
distressing than the acute disorder. It’s very common, its related to chronic stress
as longtime standing or overweight (‘policeman’s heel’), but more often the cause
is not apparent.
Clinically the patient presents with chronic pain on the inferior aspect of the heel
that has the character of relapse and remission, it occurs as a result of long
standing or prolong walking.
The tenderness on examination is localized to the site of attachment of the
planter fascia to the under heel, pain is characteristically present and severe after
periods of rest as after getting up from sleep as the patient complain of inability
of normal walking and painful heel after getting out of bed and they use to tip-toe
for few minutes until the acute pain is relieved as they can walk normally and
plantigrade.
A pressure-relieving pad together with an arch support if there is flat foot, may
help with the use of NSAID and possibly local steroid injection. Sometimes it’s
resistant to treatment and may indicate surgery.

B. Painful tarsus:
In children Osteochondritis of the navicular bone (Kohler’s disease) may cause
pain and tenderness over the dorsum of the mid-foot. If activities are
restricted for a few weeks, the pain usually disappears.
In young adults, pain over the medial aspect of the naviculum may due to a
congenital accessory navicular bone.
The accessory bone may be prominent under the skin and feels tender. X-ray
will show the type of this accessory segment that may need surgical removal;
otherwise simple adjustment of shoe wear can be of great help.
In adults, pain in the same region is sometimes associated with a prominent
ridge of bone.
X-rays show osteophytes formation at the joint between the media] cuneiform
and first metatarsal. If shoe adjustment fails to provide relief the lump may be
removed surgically.
C. Painful forefoot (metatarsalgia):
Any foot abnormality that results in faulty weight distribution may cause nagging
pain in the forefoot. It is therefore a common complaint in patients with:
1. Hallux valgus.
2. Claw toes.
3. Pescavus.
4. Flat foot.
5. Foot strain.
6. Freiberg ‘s disease.
7. Stress fracture.
8. Morton’s metatarsalgia.
9. Gout.
10. RA.
Freiberg ‘s disease:
This is a ‘crushing’ type of osteochondritis of the second metatarsal head
(rarely the third). It affects young adults, usually women. A bony lump (the
enlarged head) is palpable and tender; the joint is irritable.
X-rays show the head to be wide and flat. If discomfort is marked the
metatarsal head is excised.
Stress fracture:
Usually of the second or third metatarsal occurs in young adults after
unaccustomed activity. The affected shaft feels thick and tender. The x-ray
appearance is at first normal; but later shows fusiform callus around a fine
transverse fracture line. Rest is all that is needed.
Morton’s metatarsalgia:
The patient usually a woman of 40-50 years complains of sharp pain in the
forefoot, radiating to the toes. Tenderness is localized to one of the interdigital
spaces - usually the third - and sensation may be diminished in the cleft and
adjacent toes. This is essentially an entrapment syndrome affecting one of the
digital nerves, but secondary thickening of the nerve creates the impression of
a ‘neuroma’.
If symptoms do not respond to protective padding the ‘neuroma ‘is excised.
Toenail disorders:
The toenail of the hallux may be ingrown, overgrown or undergrown.
Ingrowing toenail:
The nail burrows into the nail groove, which ulcerates, and its wall grows over the
nail, so the term (embedded toenail) would be better.
The patient is taught to cut the nail square, to insert a cotton-wool pieces under
the ingrown edges and always to keep the feet clean and dry.
If these measures fail, the gutter treatment is worth trying, a small wedge of soft
tissue (where the nail digs in) is excised; a fine polythene tube is cut vertically in
half and a segment inserted between nail and soft tissue.
More radical measures include partial or complete removal of the nail, taking care
to remove the whole germinal matrix.
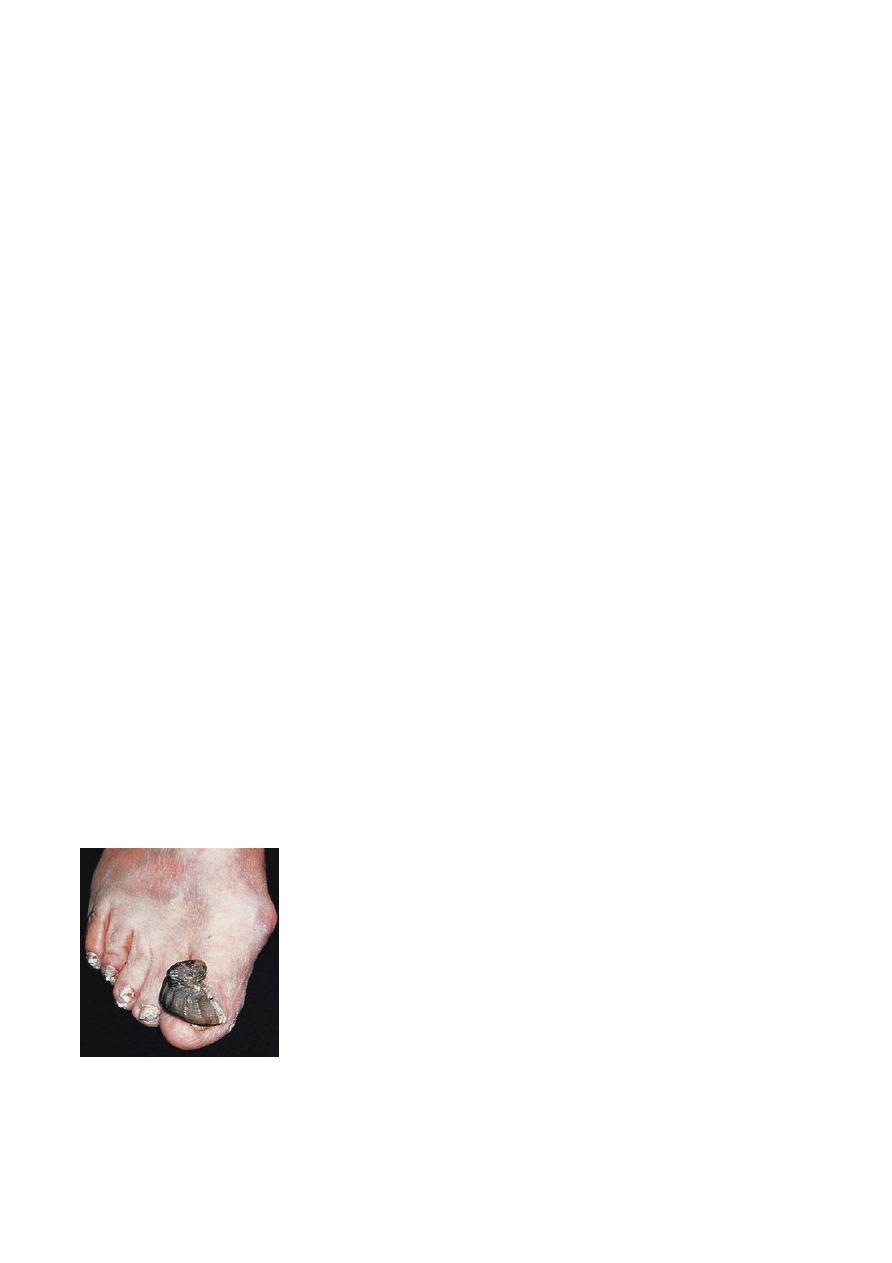
Overgrowing nail (onychogryposios):
The nail is hard, thick and curved. A chiropodist (person who care for feet) can
usually make the patient comfortable, but occasionally the nail may need excision.
Undergrown nail:
A subungual exostosis usually grows on the dorsum of the terminal phalanx and
pushes the nail upwards. The exostosis should be removed.
Done by : Murtedha Abbas