1
4th stage
Surgery
Lec-4
د.احمد ابراهيم
17/4/2016
Tumours of the large intestine
Surgical Treatment
Pre operative preparation
• Mechanical preparation,
• In colonic cancer there is good evidence that there is no benefit of pre operative
preparation .While rectal cancer suggest mechanical bowel preparation is still
appropriate .
• The antiembolic stocking ,prophylactic subcutaneous low molecular weight heparin .
• *single dose of proper antiembiotic to reduce wound infection and sepsis .
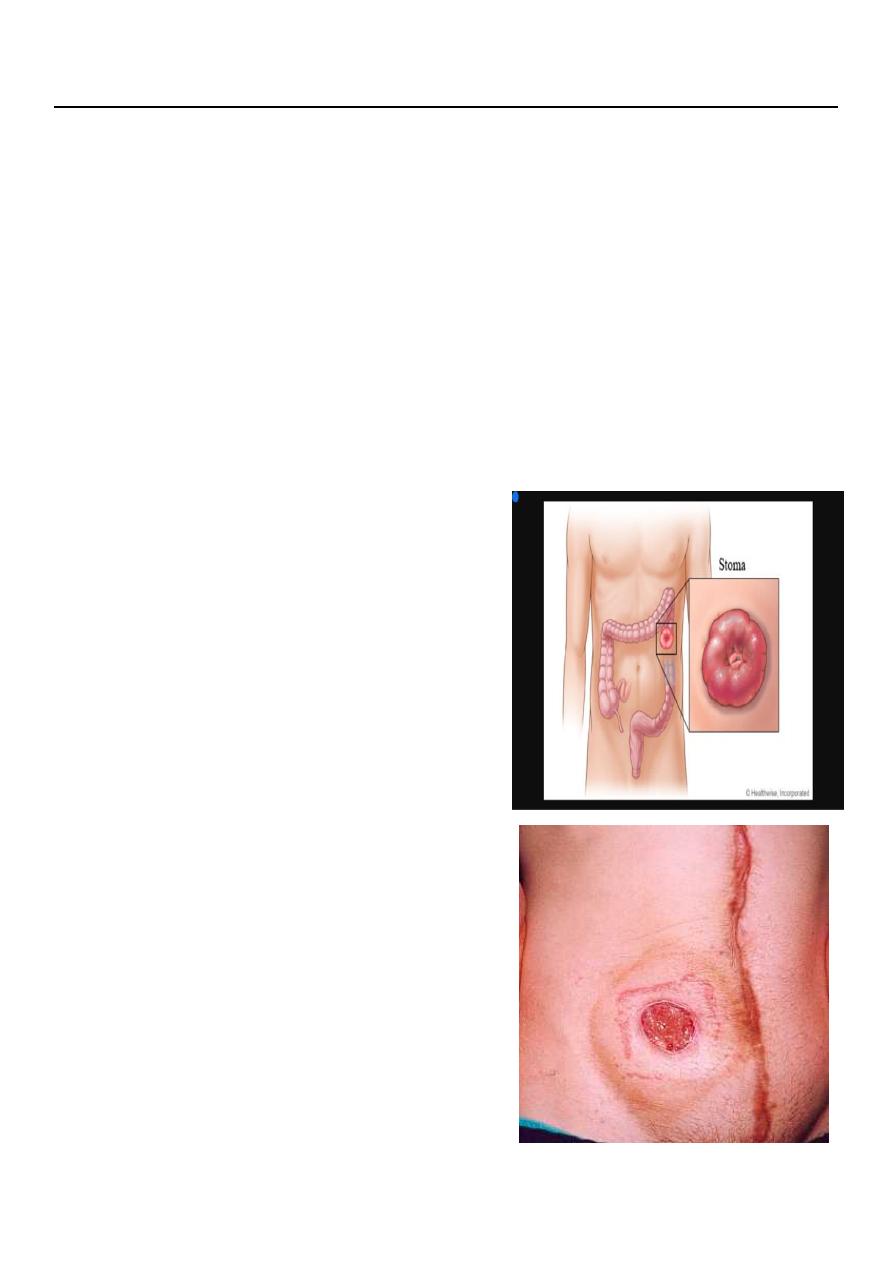
• *In all cases where stoma seem most likely
careful pre operative counselling
• Operations:
• Designed to remove the primary tumour and
draining locoregional lymph nodes .
2
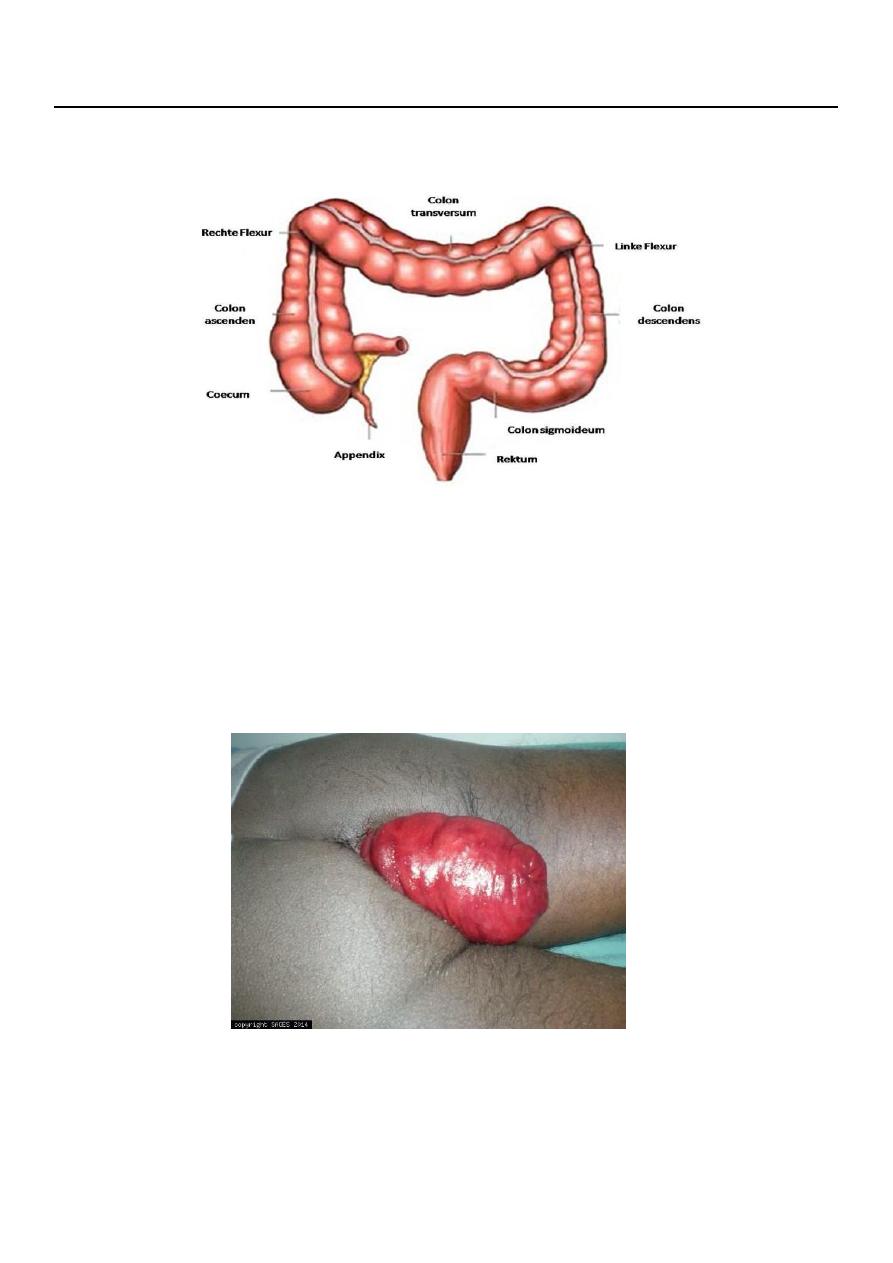
• Right hemicolectomy for right sided cancer .
• Extended right hemicolectomy for ca of transverse colon and splenic flexure ,to
remove in addition the whole transverse colon and splenic flexure .
• Left hemicolectomy ,for descending colon and sigmoid cancers.
• Laparoscopic surgery for colonic cancer nowadays
• Emergency surgery:
• In UK 20% of colonic cancer patients presents as emergency,the majority with
obstruction .
•
In right sided cancer
,usually possible to do primary anastomoses during the
operation of right hemicolectomy .while if there is perforation and the patient is
unstable ,advisable to bring out an ileo/ colostomy rather than anastamosing bowel .
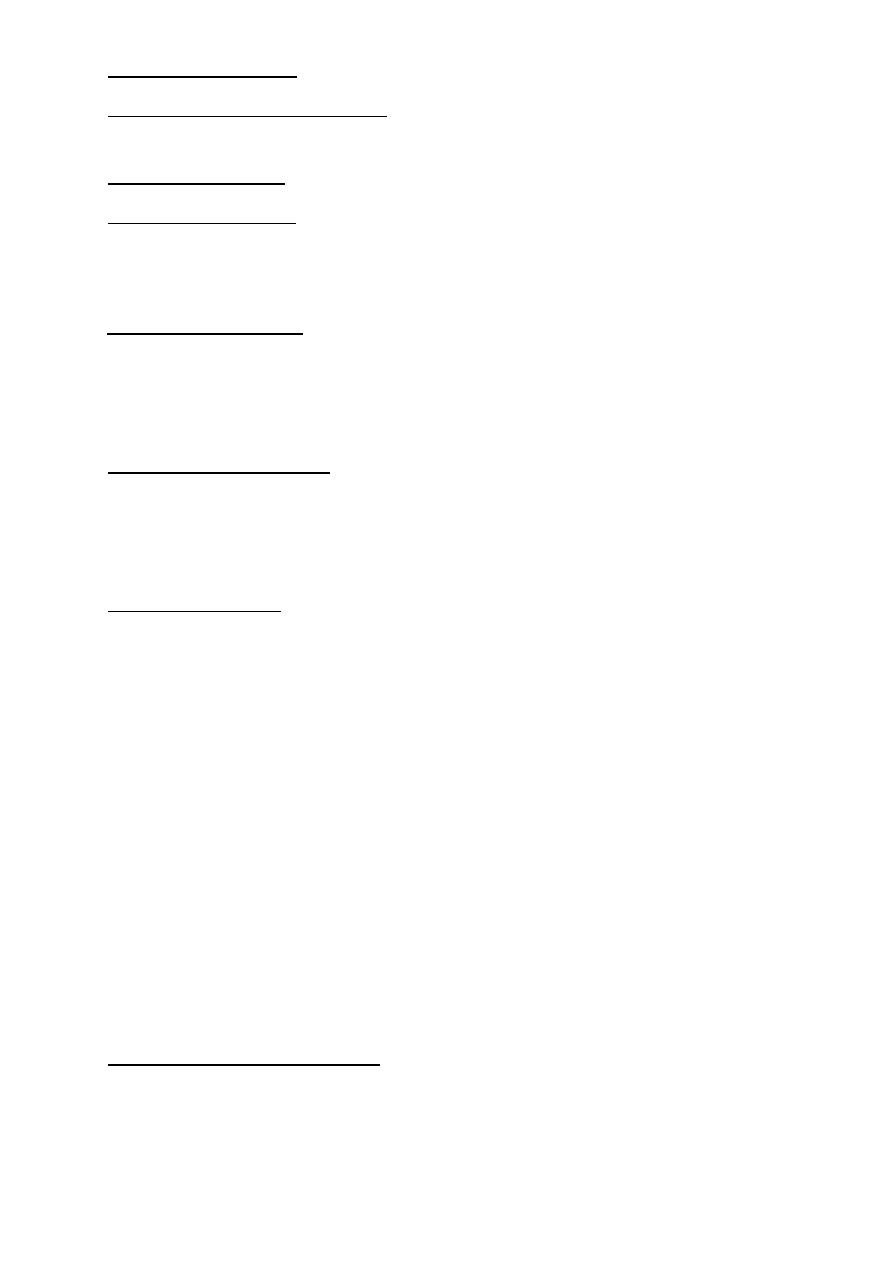
•
Left sided cancer
,resection and anastamosis,with proximal colostomy if leaking is a
possibility.But if facilities are present,an obstructing left sided lesion can be treated
with an expanding metal stent.This has the advantage of converting an emergency
operation with high chance of stoma to situation which can be managed semi
electively with a resection and anastamosis.
• PROGNOSIS:
• Five year survival 50%.
• Patients with Duke 's A ===>90% have disease free five years .( disease confined to
the bowel wall.)
• Spread of the disease out side the bowel wall reduces five year survival to60%.
• Patients with lymph nodes metastasis five year survival 30%.
• Colorectal cancer follow up
• Surveillance colonoscopy to detect synchronous and metachronous bowel tumours
• US,CT scan for liver metastasis
• CEA ( carcinoembryonic antigen
3
4th stage
Surgery
Lec-5
د.احمد ابراهيم
17/4/2016
RECTUM
Prolapse
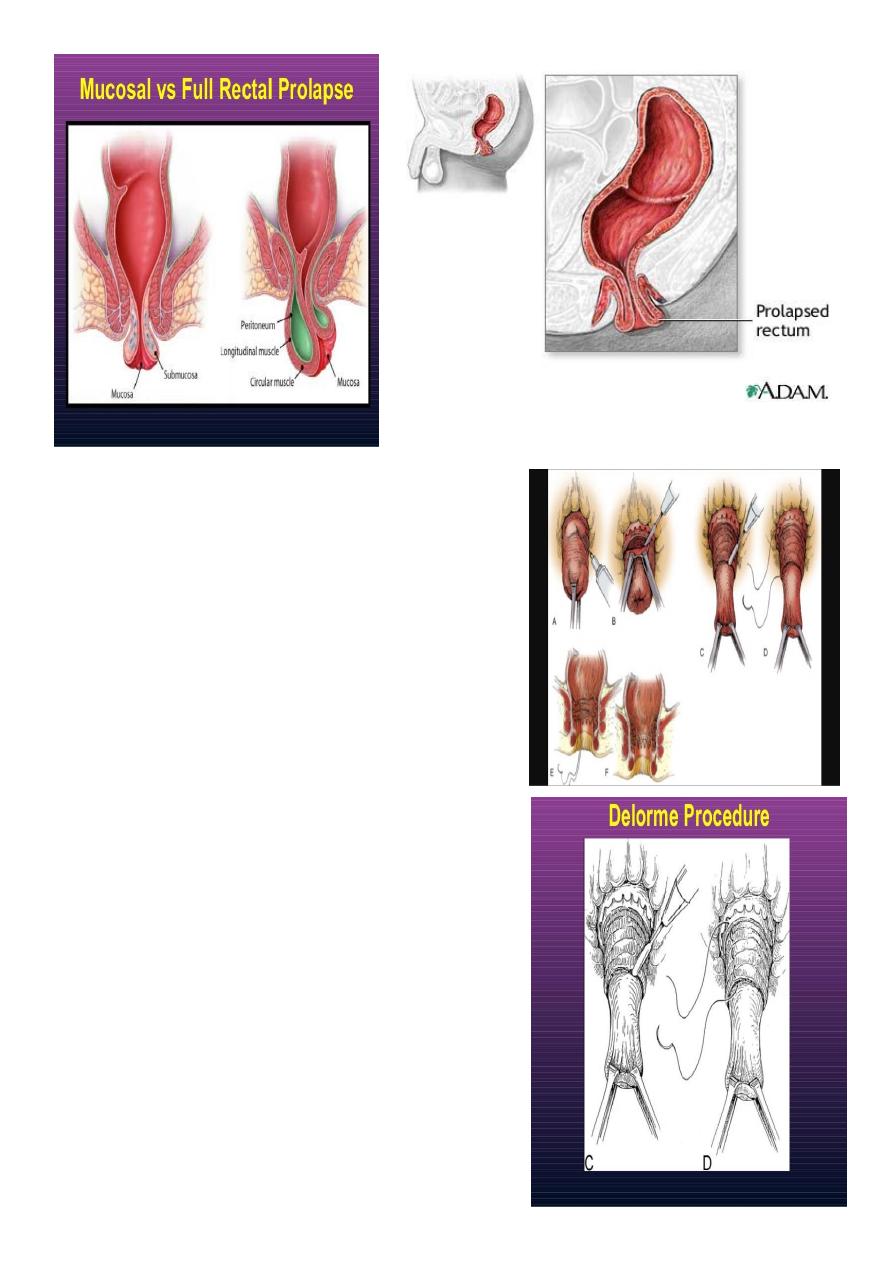
• Prolapse :two types ,
• Mucosal
• Full thickness ,whole layers .
• The mucosal ( partial thickness) can be palpated by finger and thumb ,in
children can be treated conservatively .
• While in adult, full thickness associated with incontinance
4
Surgery
is necessary. The operation is performed
either via the perineum,or the abdomen.
•
Delorme's operation
for rectal
prolapse,performed by removal of excessive
mucosa and inserting interrupted sutures in the
underlying muscle to be plicated.