AFTER MID
TOTAL LEC: 27
Gynaecology
Dr. Ishraq
Lec 27 - Uterovaginal Prolapse
DR. ISHRAQ - LEC 4+5
مكتب املدينة

1
Uterovaginal prolapse
Definition
: Protrusion of an organ or structure beyond its normal
confines.
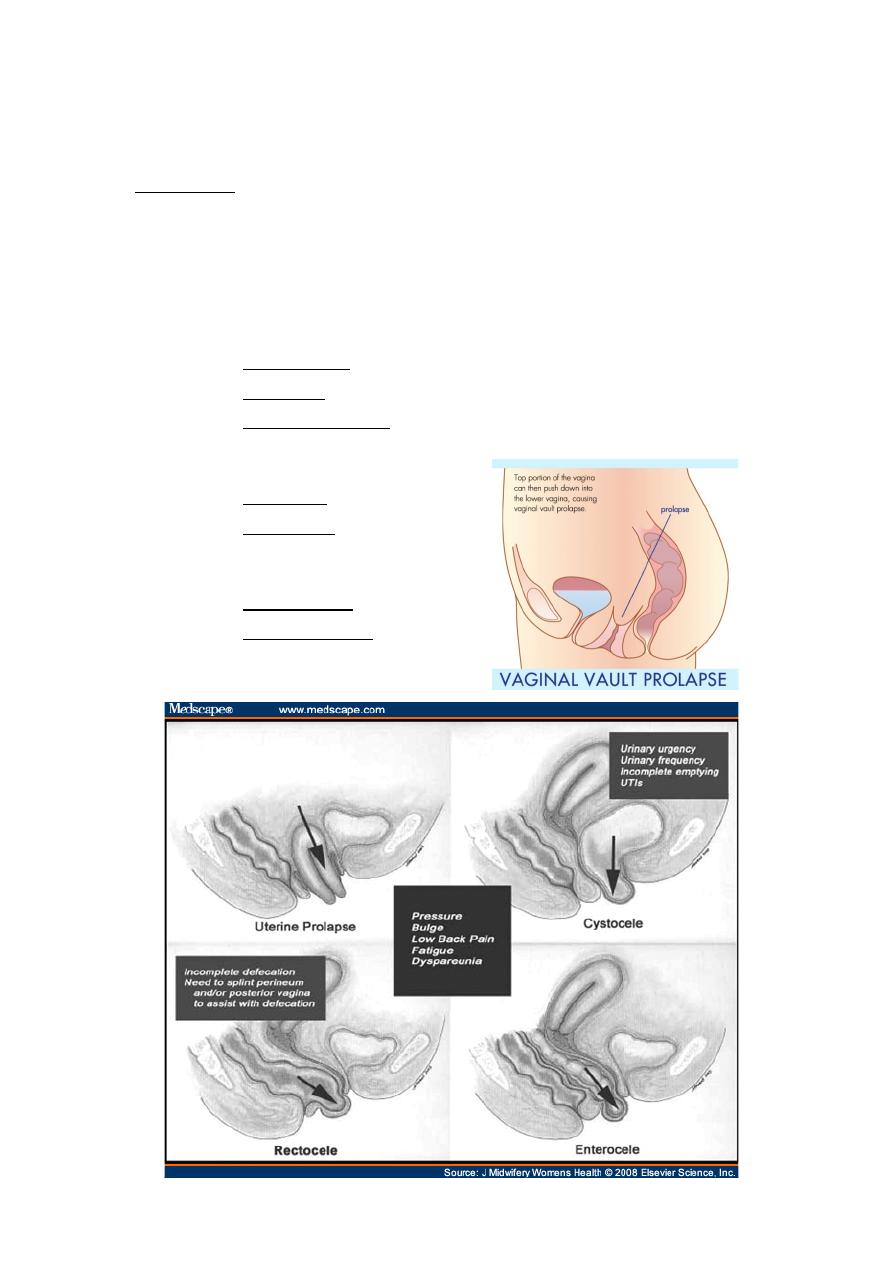
Uterovaginal prolapses are classified according to their location
and the organs contained within them into:
1) Anterior vaginal wall prolapse:
a. Urethrocele : urethral descent
b. Cystocele: bladder descent
c. Cystourethrocele: descent of bladder and urethra.
2) Posterior vaginal wall prolapse
a. Rectocele
b. Enterocele
3) Apical vaginal prolapse:
a. Uterovaginal
b. Vault prolapse: post
hysterectomy
2
Prevalence:
• 12-30% in multiparous.
• 2% in nulliparous.
• Three degrees of prolapse are described:
§
1
st
: descent within the vagina.
§
2
nd
: descent to the introitus.
§
3
rd
: descent outside the introitus.
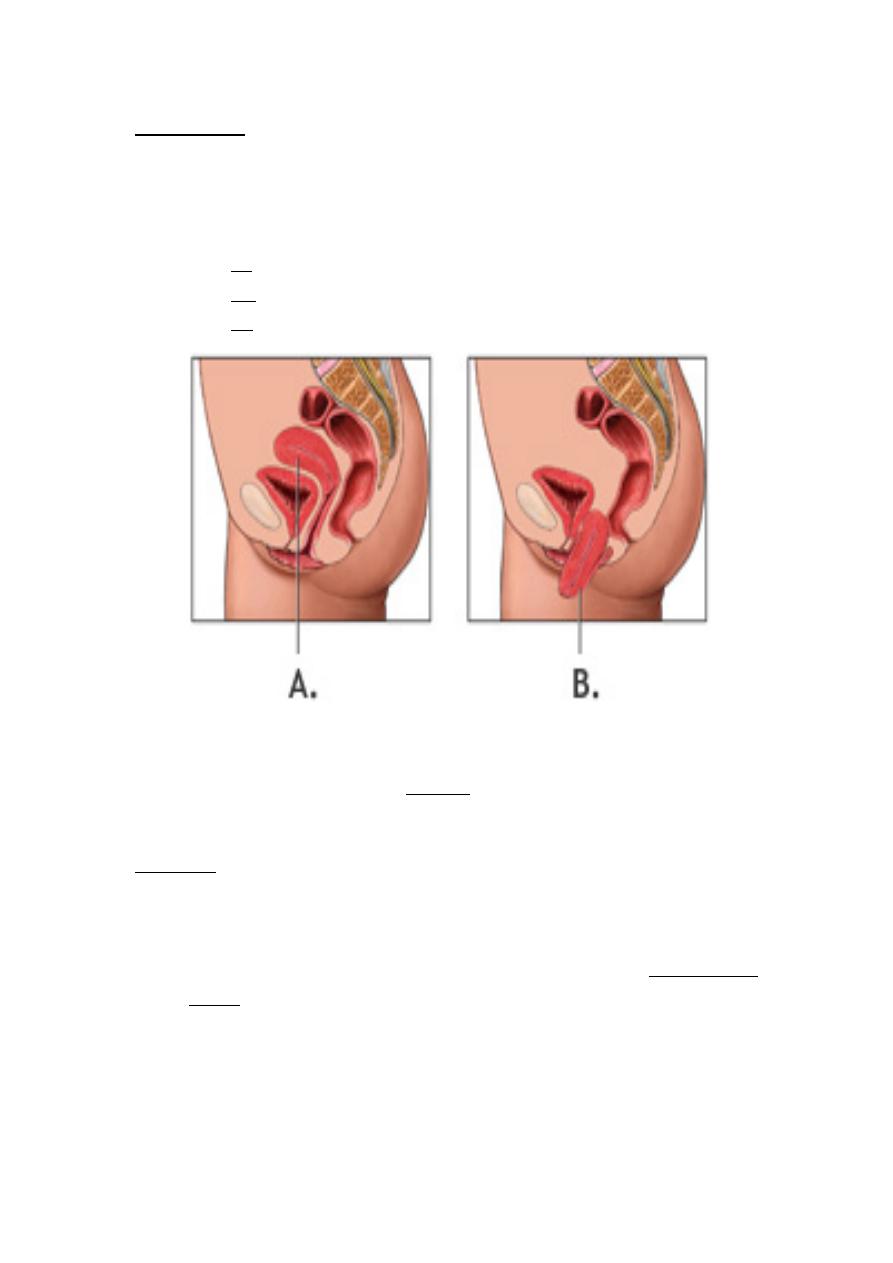
A: Normal position of uterus and cervix
B: Descent of cervix and uterus outside the introitus "procidentia" and is
usually accompanied by cystourethrocele and rectocele.
Etiology:
1) Congenital: congenital weakness of connective tissue especially
when it occurs in nulliparous women.
2) Child birth and raised intra abdominal pressure: single major
factor. Nerve and mechanical damage in women with prolapse
occurs as a result of vaginal delivery. (Prolonged second stage of
labor, instrumental delivery and macrosomic baby are all
associated risk factors).
3
Prolapse can occur during pregnancy but this is rare and it is
thought to be mediated by the effects of progesterone and relaxin.
In addition, raised intra-abdominal pressure during pregnancy will
put an added strain on the pelvic floor.
Raised intra-abdominal pressure outside of pregnancy (example:
chronic cough or constipation) is also a risk factor.
3) Aging: loss of collagen and weakness of fascia and connective
tissues are particularly noted post menopause as a consequence of
estrogen deficiency.
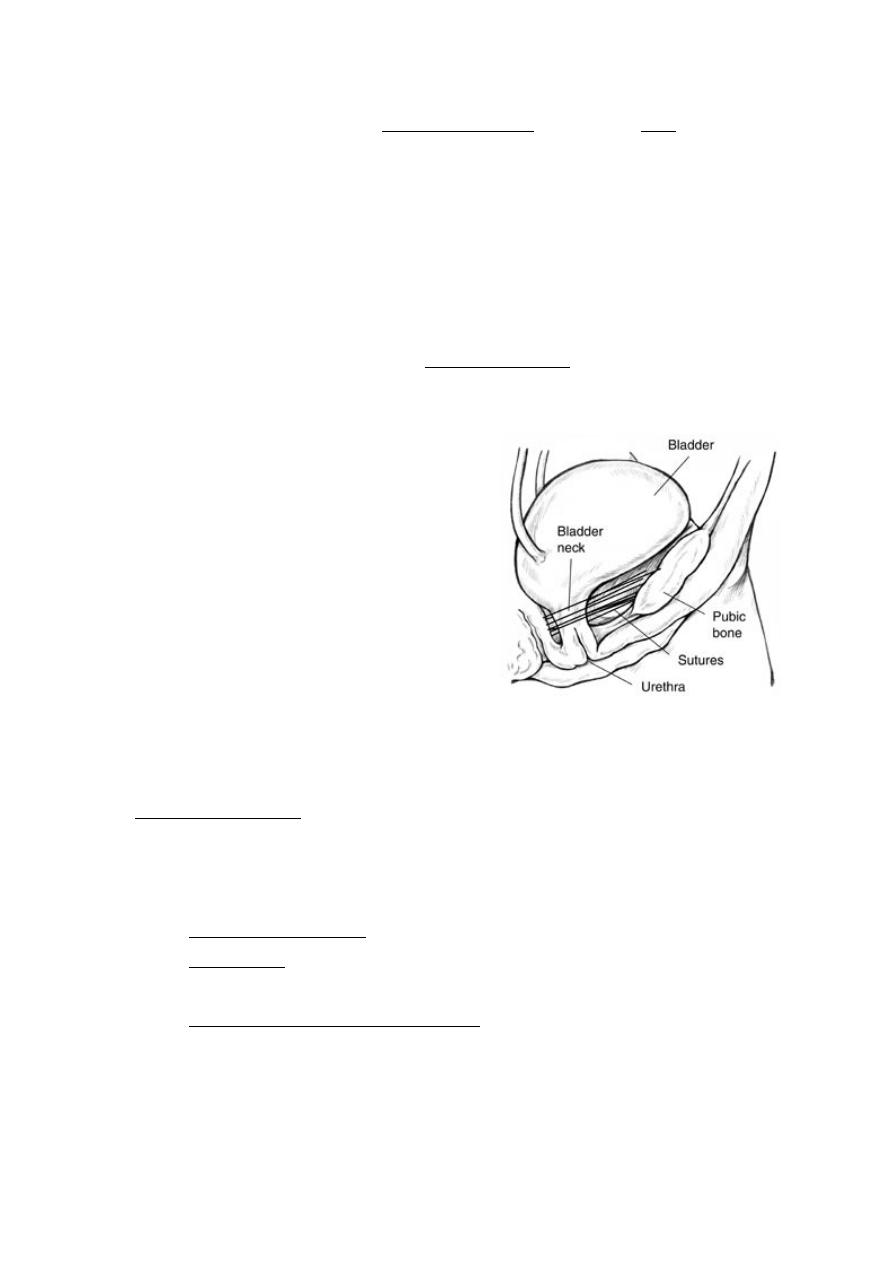
4) Post operative: poor attention to
vaginal vault support at the time of
hysterectomy leads to vault prolapse
in approximately 1% of cases.
For example: Rectocele or enterocele
can complicate colposuspension (a
surgery done in case of stress urinary
incontinence i.e. it strengthens the
compartment anterior to the vagina
but not that posterior to it).
Pathophysiology
:
There are 3 components that are responsible for supporting the
position of the uterus and vagina:
§
Ligaments and fascia by suspension from pelvic side walls.
§
Levator ani muscle by constricting and there by maintaining organ
position.
§
Posterior angulation of the vagina which is enhanced by the rise in
abdominal pressure causing closure of the flap valve.
4
Damage to any of these mechanisms will contribute to prolapse:
§
Uterosacral ligament.
§
Cardinal "transverse cervical ligament" (the most Important)
§
Rectovaginal fascia.
History
:
v
non specific symptoms: lump (most common), local discomfort,
backache, bleeding, infection if ulcerated, and dyspareunia.
Rarely, in severe cystourethrocele renal failure may occur as a result
of ureteric kinking.
v
Specific symptoms:
o Cystourethrocele: urinary frequency, urgency, voiding
difficulties, UTI, and stress incontinence.
o Rectocele: incomplete bowel emptying, digitation (the patient
presses on the rectocele with her fingers) and splinting (the
patient inserts her finger into the vagina to pushes the bulge
in) while defecating to aid passage of stool.
Vaginal examination:
Prolapse may be obvious, when examining the
patient in dorsal position, if it protrudes beyond the
introitus. Vaginal pelvic examination should be performed &
pelvic masses should be excluded.
The anterior & posterior vaginal wall & cervical
descent should be assessed with the patient straining in
the left lateral position using sim's speculum.
Combined rectal & vaginal digital examination can be aid to
differentiate rectocele from enterocele.
Differential diagnosis:
o Anterior: congenital or inclusion dermoid vaginal cyst, urethral
diverticulum.
o Uterovaginal prolapse: large uterine polyp.
5
Investigations:
v
Urinary symptoms: urine microscopy, cystometry, and cystoscopy. If
renal failure serum urea & creatinine, and renal ultrasound.
v
Women with symptoms of obstructed defecation: MR proctography
can help diagnose a rectocele.
Treatment:
Choices of treatment depend on patient wishes, level of fitness &
desire to preserve coital function.
Prior to specific treatment: correct obesity, chronic cough, and
constipation & if the prolapse is ulcerated, a 7 day course of topical
estrogen should be administered.
Prevention: shortening of the second stage of labor, reducing traumatic
delivery.
Episiotomy & HRT (no role in Rx)
Medical treatment:
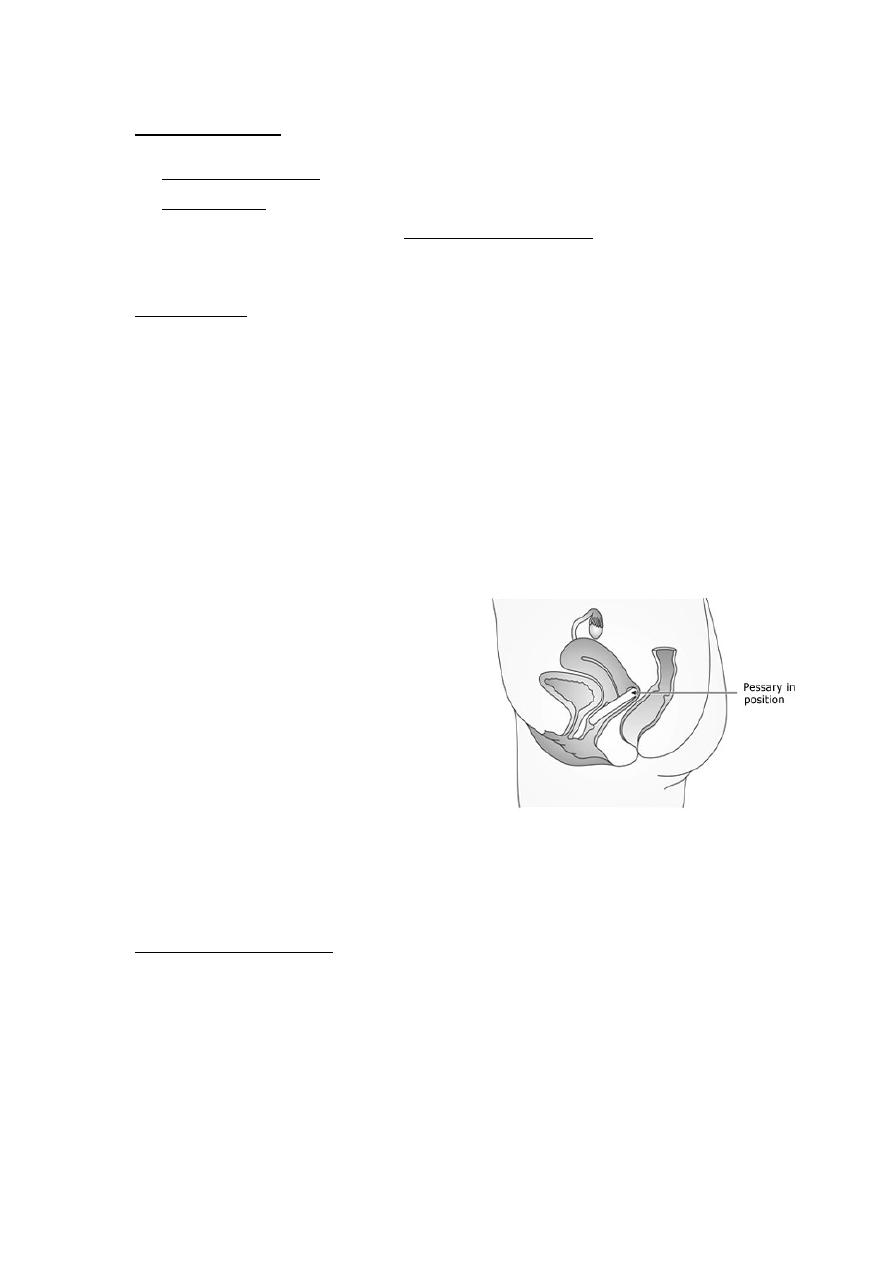
§
Silicon rubber based ring
pessary: Inserted into the
vagina in the same way as
vaginal diaphragm & need
replacement every 6 months.
§
Shelf pessary: rarely used but may be useful in women who
cannot retain a ring pessary (vaginal ulceration or infection). The
vagina should be inspected carefully at the time replacement.
Indications for pessary:
1. Patient's wish.
2. As a therapeutic test.
3. Child bearing not completed.
4. Medically unfit.
5. During & after pregnancy (awaiting involution).
6. While awaiting surgery.
6
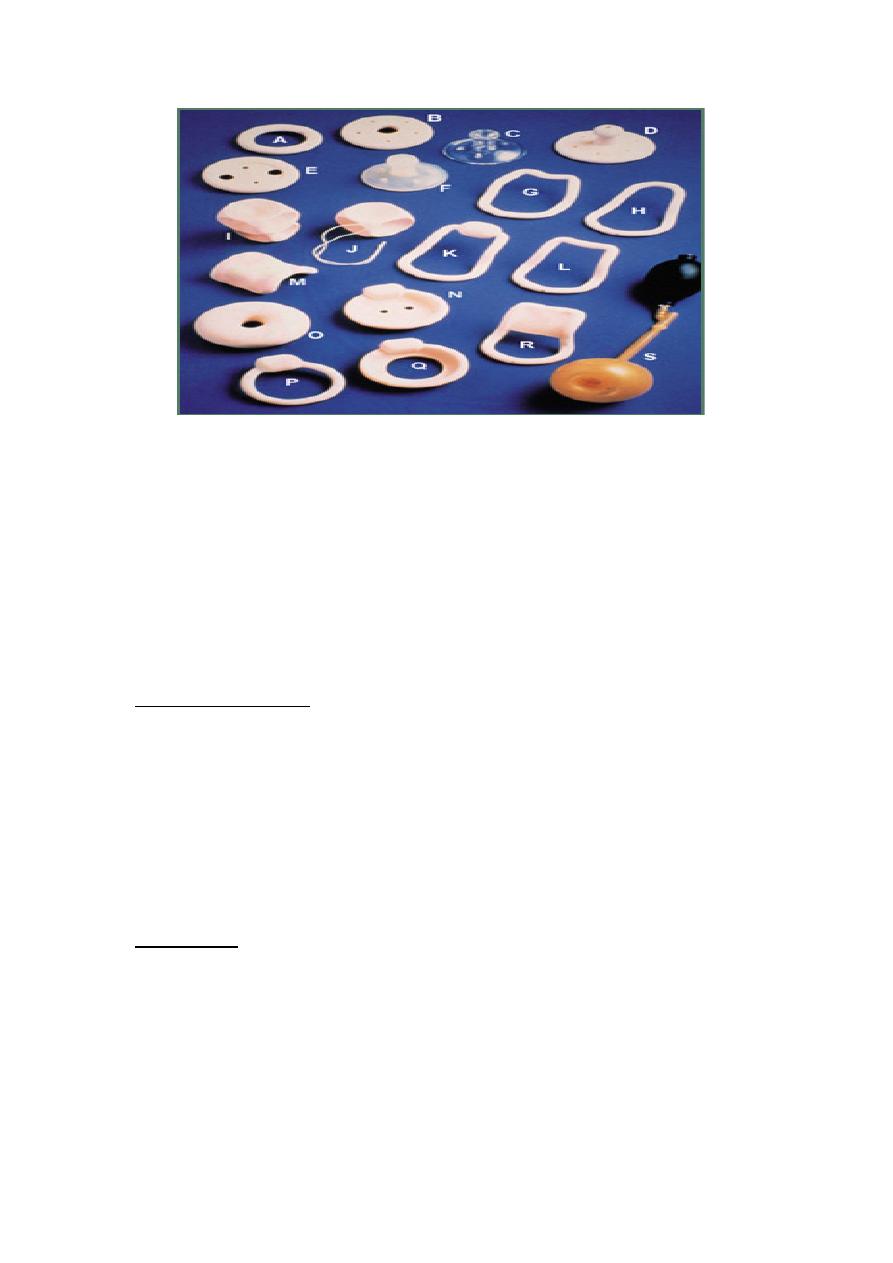
A: ring pessary (most commonly used) D: Shelf pessary
Surgical Treatment:
The aim of surgical repair is to restore anatomy & function. There
are vaginal & abdominal operations designed to correct prolapse & the
choice often depends on woman's wish to preserve coital function.
Cystourethrocele:
Anterior colporrhaphy (repair) is the most commonly performed
surgical procedure but should be avoided if there is concurrent stress
incontinence. An anterior vaginal wall incision is made & the facial
defect allowing the bladder to be herniated through is identified &
closed with the bladder position restored, any redundant vaginal
epithelium is excised & the incision is closed.
Rectocele:
Posterior repair (colporrhaphy) is the most commonly performed
procedure. The posterior vaginal wall incision is made & the facial defect
allowing the rectum to herniated through is identified & closed & the
redundant vaginal epithelium is excised & the incision closed.
7
Enterocele:
The surgical principle is similar to those of A&P repair but the
peritoneal sac containing the small bowel should be excised. In addition,
the pouch of Douglas is closed by approximating the peritoneum
&/uterosacral ligaments.
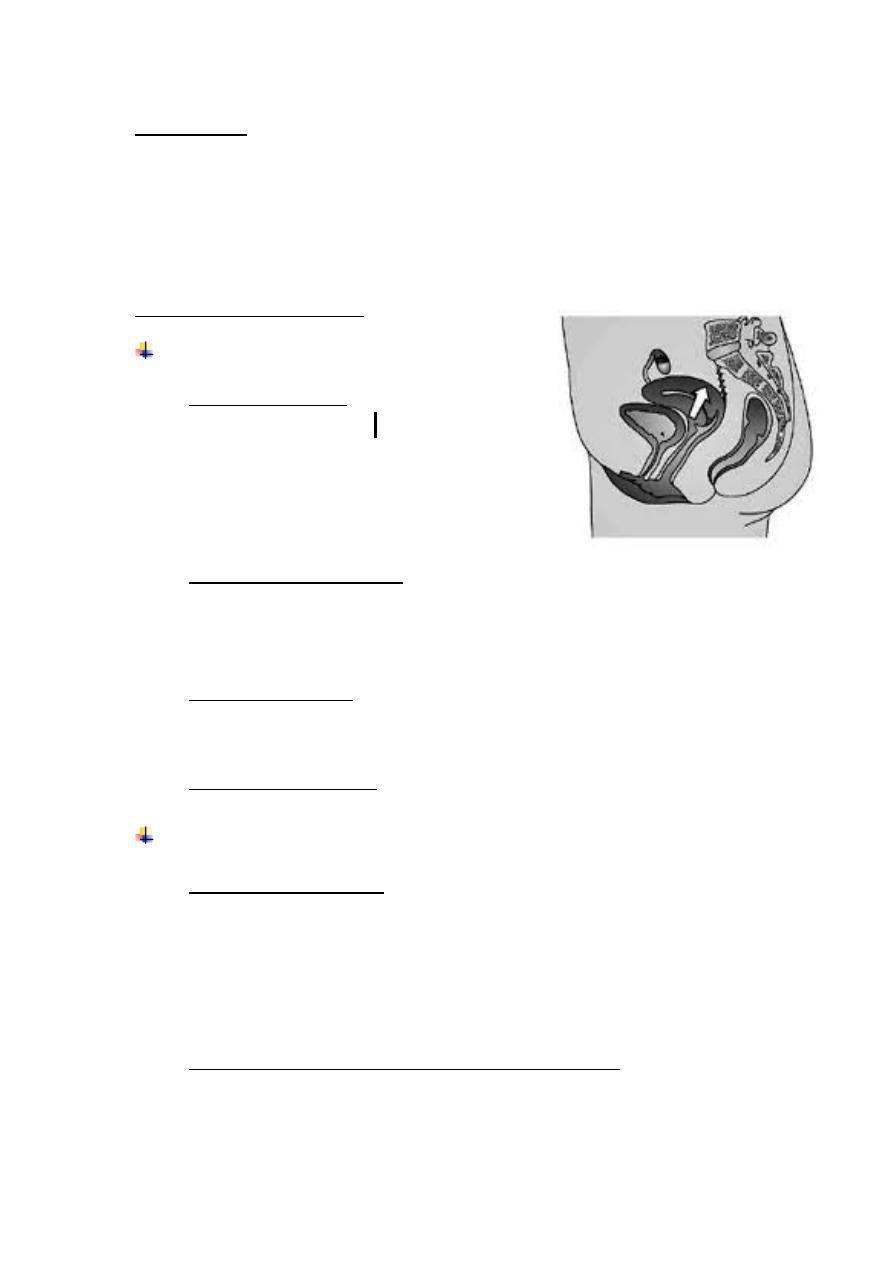
Uterovaginal prolapse:
Uterine preserving surgery:
§
Hysterosacropexy: open or laparoscopic
route & a mesh is
attached to the
isthmus of the cervix & the uterus is
suspended by attaching the other part of
mesh to the anterior longitudinal
ligament on the sacrum.
§
The Manchester repair: amputating the cervix & using the
uterosacral cardinal ligament complex to support the uterus. May
be complicated by cervical stenosis (causing infertility) or
incompetence (causing repeated abortions).
§
Le fort colpocliesis: if the patient is unfit for major surgery & is not
sexually active. It involves partial closure of vagina while
preserving the uterus. (however it has a low success rate)
§
Total mesh procedure using an introducer device.
Procedures involving Hysterectomy :
§
Vaginal hysterectomy: the operation involve making an incision
around the cervix & entering the peritoneal cavity from the
vaginal side ligating all major blood vessels & delivering the uterus
through the vagina. The standard procedure is to shorten the
stretched uterosacral cardinal ligaments complex & then re suture
into the vault of the vagina.
§
Total abdominal hysterectomy & sacrocolpopexy: risk of vaginal
erosion by the mesh.
8
§
Subtotal abdominal hysterectomy & sacrocervicopexy: (not very
much used)the cervix is used as an attachment point for the mesh
where there is negligible chance of erosion & the mesh is
suspended to the anterior longitudinal ligament on the sacrum.
If there is concomitant anterior prolapse at the time of vaginal
hysterectomy an anterior repair may be performed. If there is
concomitant anterior prolapse at the time of abdominal procedure a
paravaginal repair can be performed, avoiding the need for an incision
in the vagina.
Vault prolapse:
Sacrocolpopexy is done. The inverted vaginal vault is attached to
the sacrum using a mesh & the pouch of douglas is closed. Sacrospinous
ligament fixation is a vaginal procedure in which the vault is sutured to
one or other sacrospinous ligament.
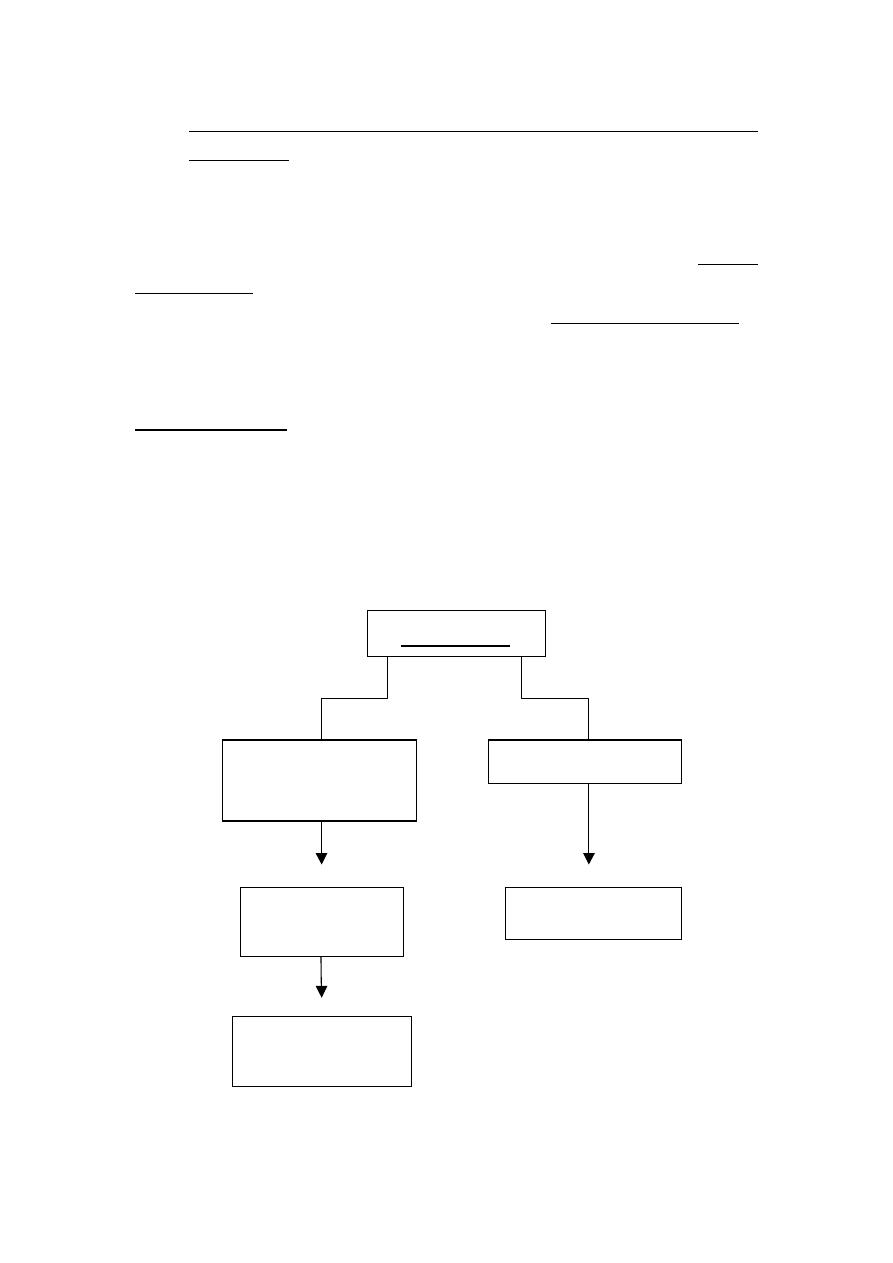
Rectocele
Soiling
Constipation
Anorectal
studies
Conservative
treatment
Lump
posterior repair
9
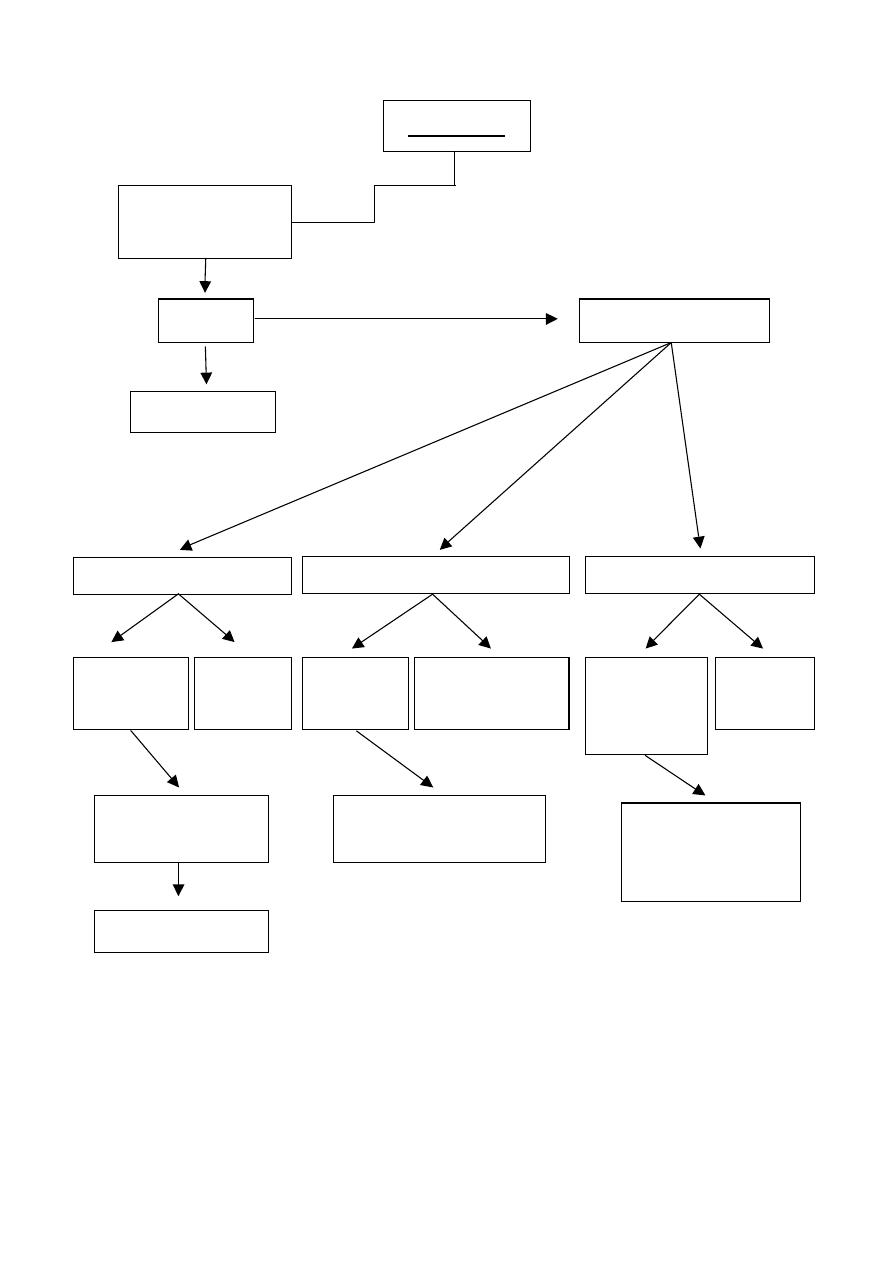
If failed
Prolapse
Conservative
Treatment
Pessary
Annual review
Surgical Treatment
Cystourethrocele
Uterovaginal prolapse
vault prolapse
Anterior
Repair
Urinary
symptoms
Urodynamic
Study
Colposuspension
Retain
Uterus
Vaginal
Hysterectomy
Reserve
vaginal
function
Vaginal
Repair
Sacrohysteropexy
Manchester Repair
Sacrocolpopexy &
Sacrospinous
Ligament fixation
