
Nephrology
Dr. ALI
A.ALLAWI
Medicine
“ DRUGS AND THE
KIDNEY
”
Dr.Ali
Lecture
#2
Total Lec: 44

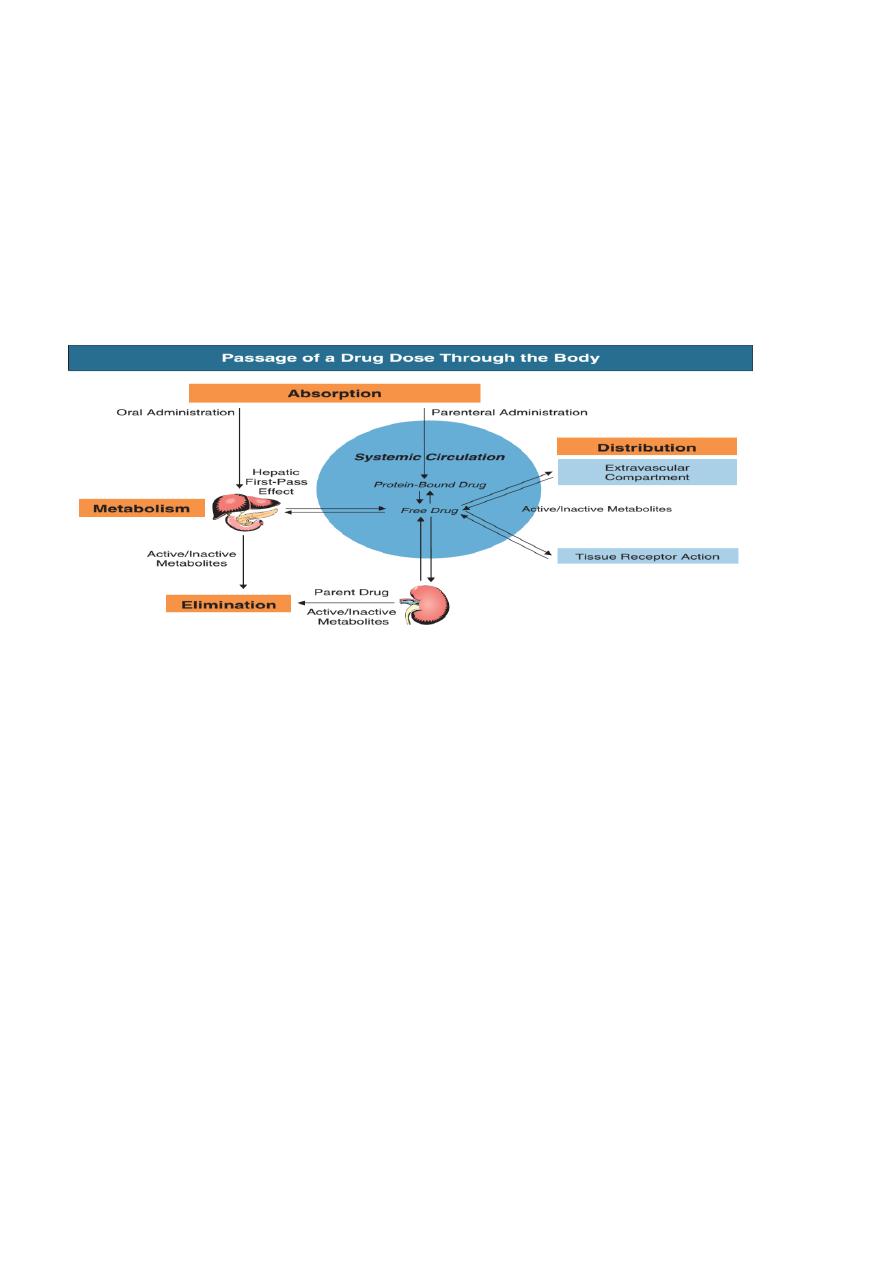
Drug-induced renal disease
-The kidney is susceptible to damage by drugs because it is the route of excretion of many watersoluble
compounds, including drugs and their metabolites .
-Some may reach high concentrations in the renal cortex as a result of proximal tubular transport
mechanisms .
-Others are concentrated in the medulla by the operation of the countercurrent system .The same applies
to certain toxins.
-Very commonly, drugs contribute to the development of acute tubular necrosis as one of multiple
insults .Numerically, reactions to NSAIDs and ACE inhibitors are the most important .
-Haemodynamic renal impairment, acute tubular necrosis and allergic reactions are usually reversible if
recognised early enough .Other types, however, especially those associated with extensive fibrosis, are
less likely to be reversible.
Pre-renal
Impaired perfusion of the kidneys can result from drugs that
cause :
Hypovolaemia ,e.g.
a - Potent loop diuretics such as furosemide, especially in elderly patients
b- Renal salt and water loss, such as from hypercalcaemia induced by vitamin D therapy since
hypercalcaemia adversely affects renal tubular salt and water conservation
Decrease in cardiac output, which impairs renal perfusion e.g .beta-blockers
Decreased renal blood flow (e.g .ACE inhibitors particularly in the presence of renovascular
disease
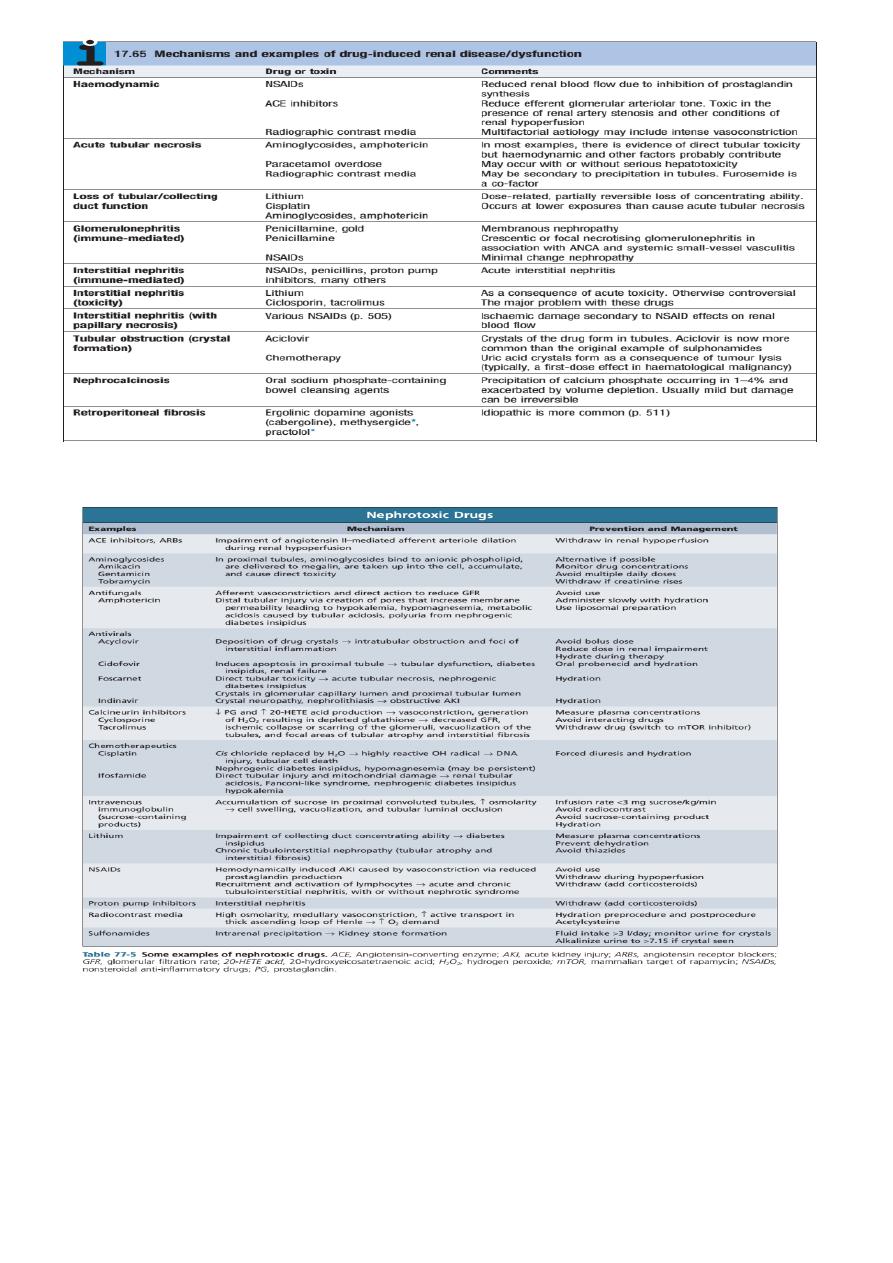
Renal
Several mechanisms of drug-induced renal damage exist and may co-exist .
Acute tubular necrosis produced by direct nephrotoxicity
Examples include prolonged or excessive treatment with aminoglycosides (e.g.
gentamicin ,streptomycin), amphotericin B, heavy metals or carbon tetrachloride .
The combination of aminoglycosides with furosemide is particularly nephrotoxic .
Acute
tubulointerstitial nephritis with interstitial oedema and inflmmatory cell infitration .This
cell-mediated hypersensitivity nephritis occurs with many drugs, including penicillins, sulphonamides
and NSAIDs
.
Chronic tubulointerstitial nephritis due to drugs .
Membranous glomerulonephritis ,e.g .penicillamine,
gold ,anti-TNF
Post-renal
Retroperitoneal fibrosis with urinary tract obstruction can result from the use of drugs (methysergide ,
lysergic acid, ergot derived dopamine receptor agonists (cabergoline, bromocriptine, pergolide),
ergotamine ,methyldopa, hydralazine ,
beta-blockers proctolol .
Tubular obstruction (crystal formation: )Aciclovir
, Crystals of the drug form in tubules .Aciclovir is
now more common than the original example of sulphonamides
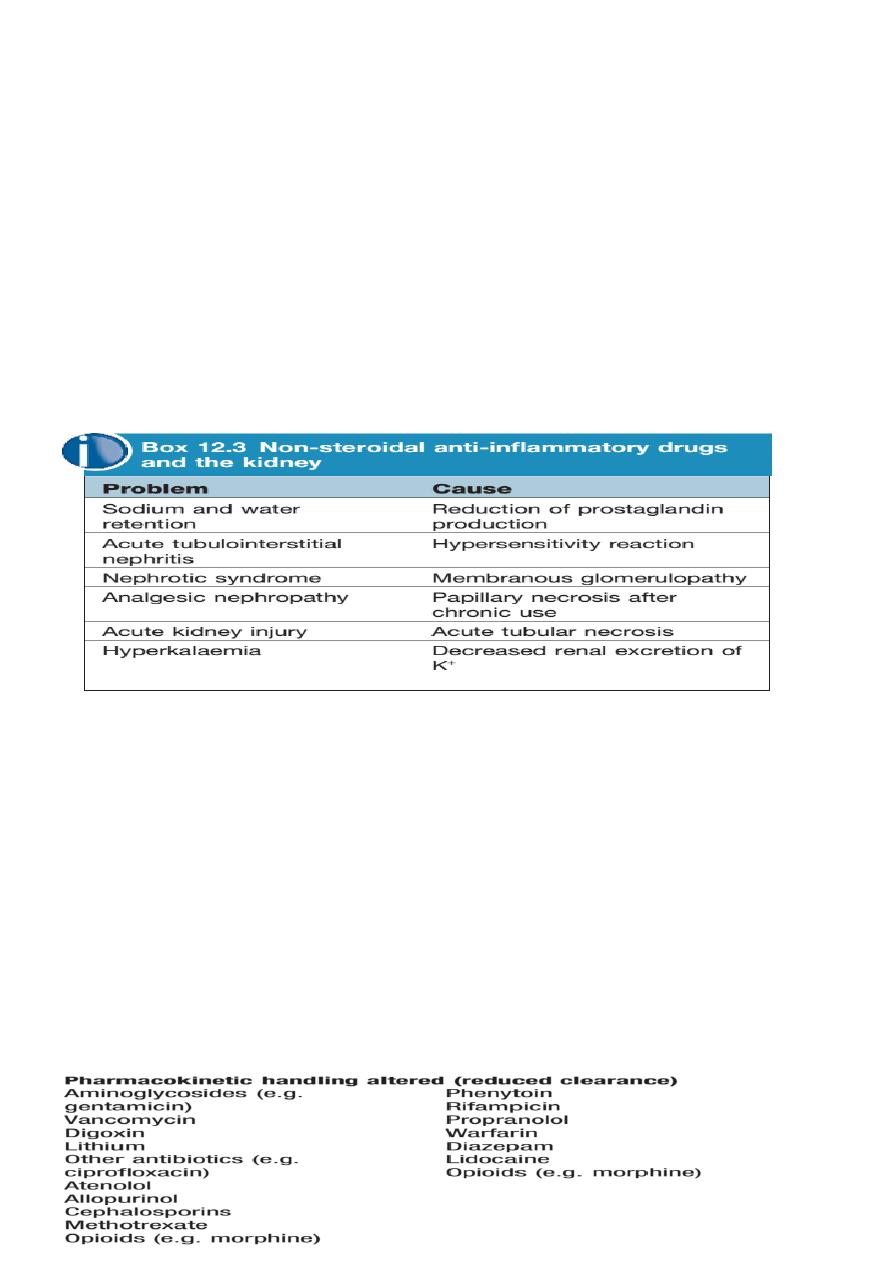
NSAIDs
Impairment of renal function may develop in patients on NSAID, since prostaglandins play an
important role in regulating renal blood flow .
This is particularly likely in patients with other disorders, such as heart failure ,cirrhosis, sepsis and
preexisting renal impairment .
In addition, idiosyncratic immune reactions may occur, causing minimal change nephrotic syndrome
and acute interstitial nephritis
.
Analgesic nephropathy is now a rare complication of longterm use.
ACE inhibitors
These abolish the compensatory angiotensin II mediated vasoconstriction of the glomerular efferent
arteriole that takes place in order to maintain glomerular perfusion pressure distal to a renal artery
stenosis and in renal hypoperfusion
.
Monitoring of renal function before and after initiation of therapy is essential.
Prescribing drugs for patients with renal disease
Patients with renal impairment are readily identified by having a low estimated glomerular fitration
rate GFR
<
06
mL/min) based on their serum creatinine,age, sex and ethnic group
.
This group includes a large proportion of elderly patients .
If a drug (or its active metabolites) is eliminated predominantly by the kidneys, it will tend to
accumulate and so the maintenance dose must be reduced .For some drugs, renal impairment makes
patients more sensitive to their adverse pharmacodynamic effects.
Some drugs that require extra caution in patients with renal disease
aya