Nephrology
Dr.
ALI Al-Saedi
Medicine
“The kidney and
hypertension
”
Dr.Ali
Lecture
#2
Total Lec: 46
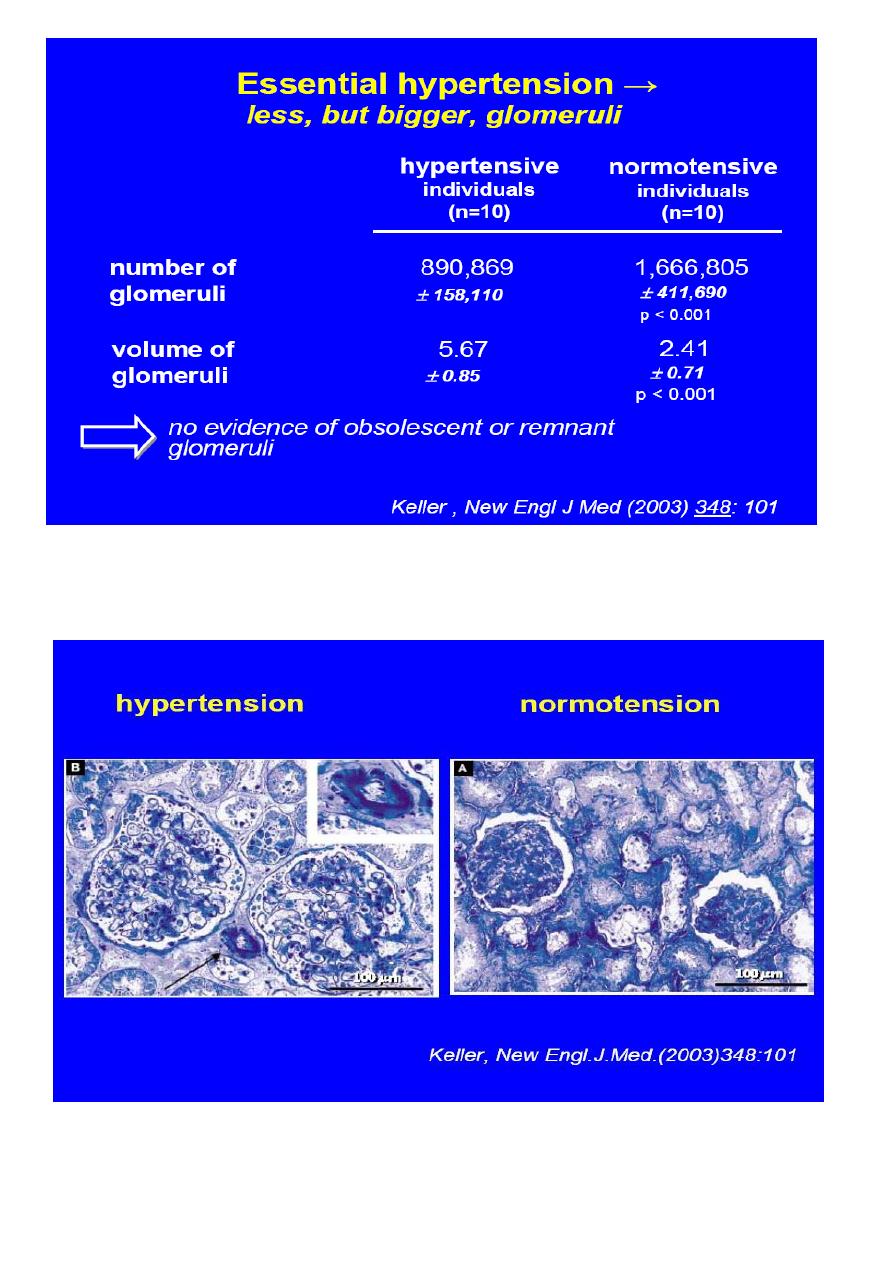
• The kidney as the cause of hypertension
• The kidney as the victim of hypertension
– role of hypertension in CKD patients
• progression
• cardiovascular risk
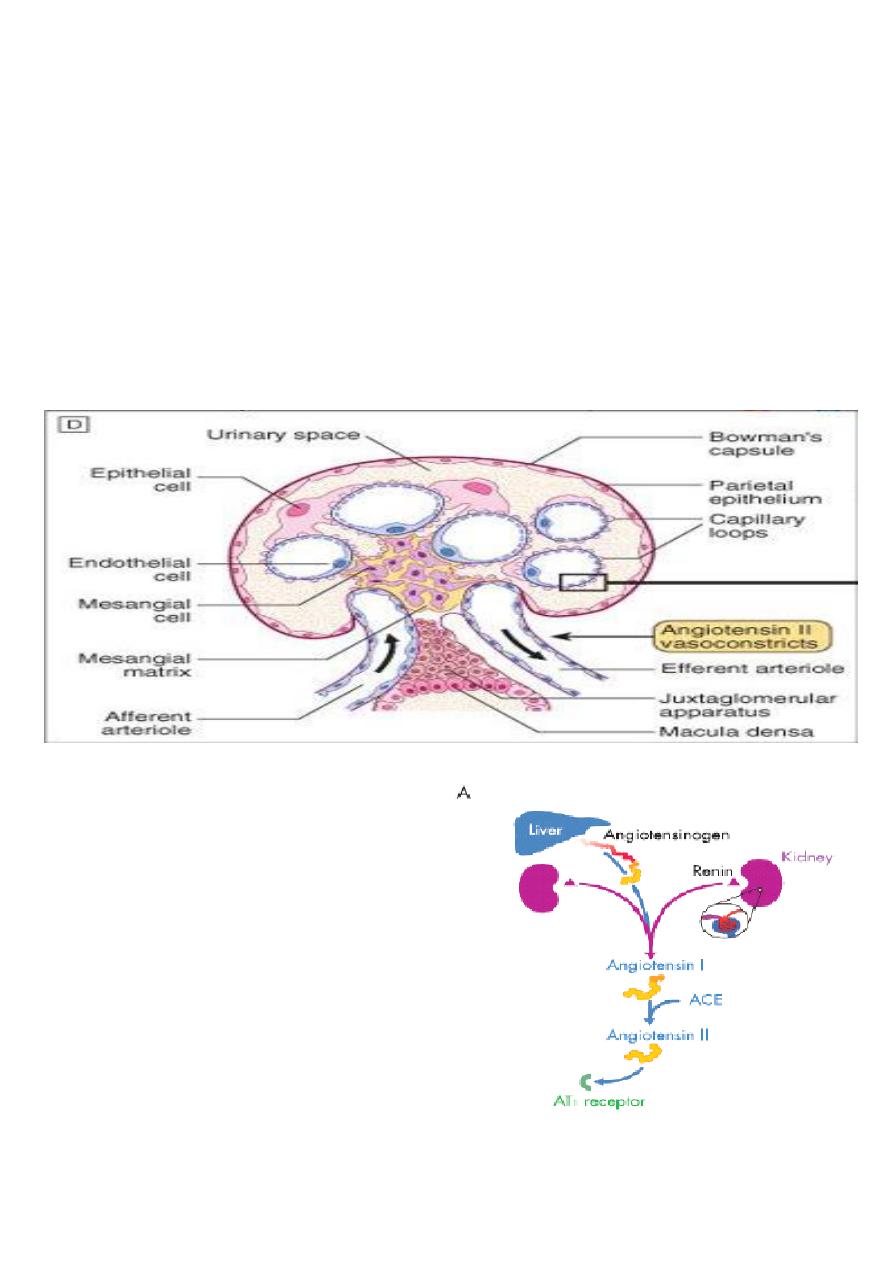
• Components of hypertension: Renin
Sodium
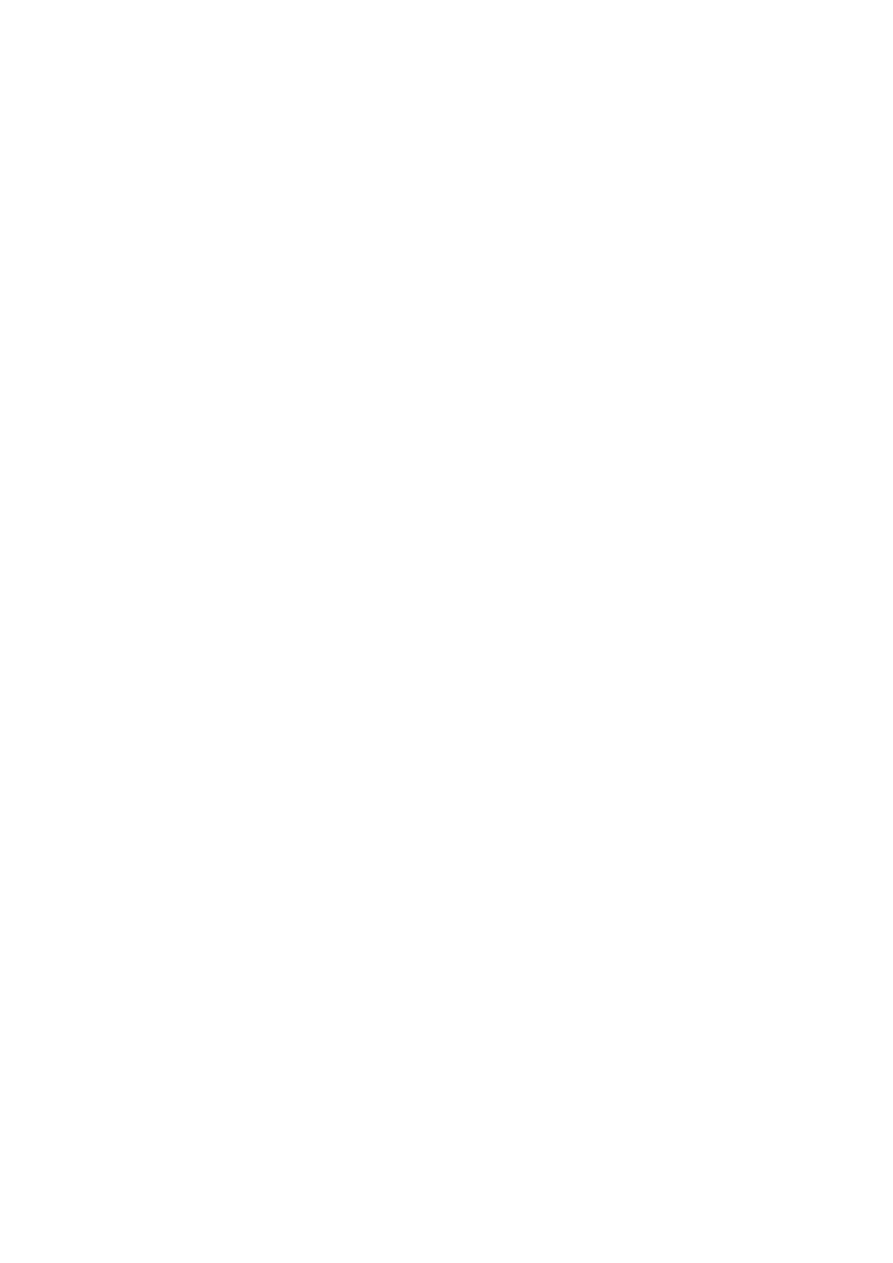
• Renin
• Is an enzyme secreted from specialized cells in the efferent arteriole of the glomerulus
(JGA).
• Maintains blood pressure through vasoconstriction when there is inadequate salt to
maintain volume.
• RAS
• Has a central role in acute and chronic
regulation of BP
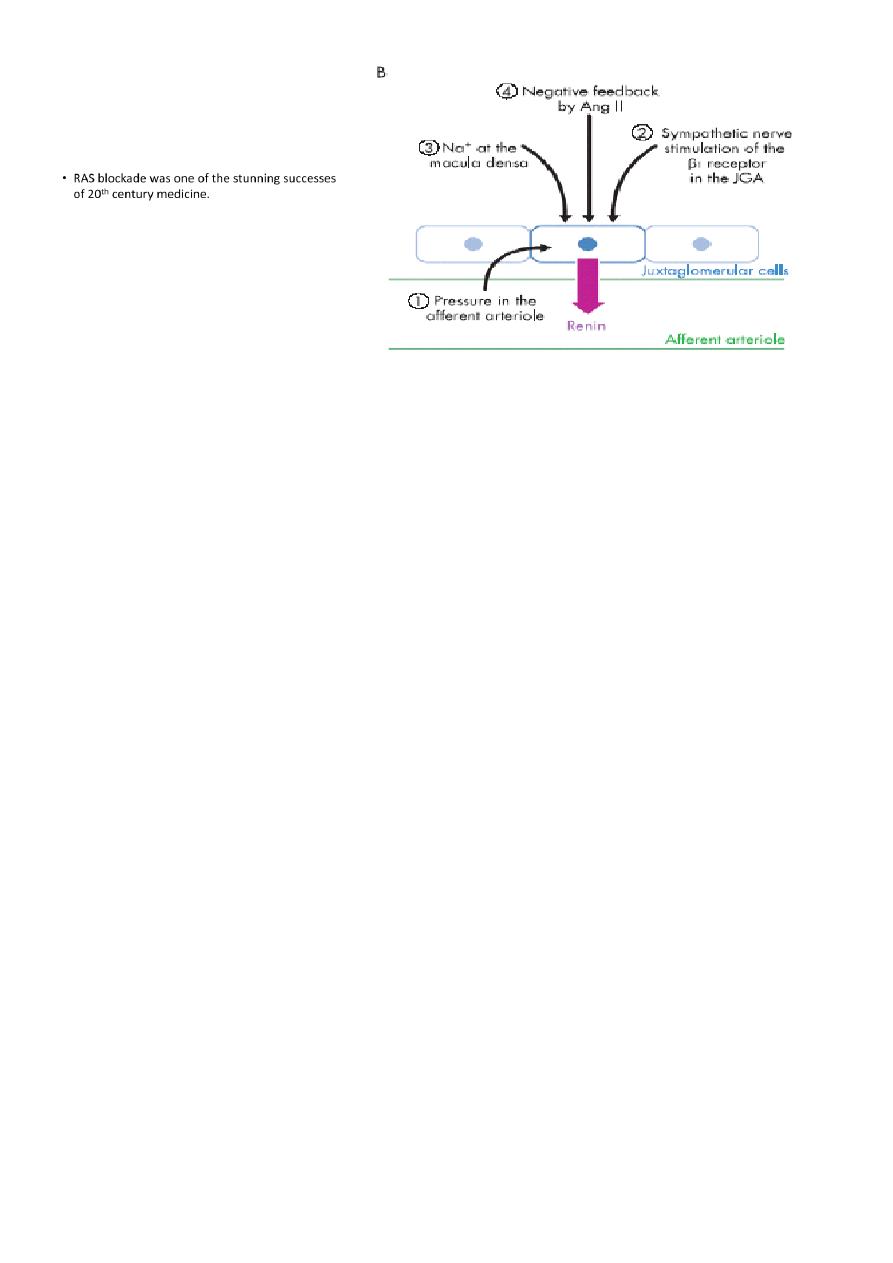
Factors controlling Renin release:
• Hypertension is a frequent finding in both acute and chronic renal disease,
• Depends on type of renal disease and its duration.
– Glomerular
– Vascular
–
Acute glomerular disease
• Patients with acute glomerular disease, such as poststreptococcal glomerulonephritis or
membranous nephropathy, tend to be volume expanded and edematous due to sodium
retention.
Vascular disease
• Hypertension is also common in acute vascular diseases, such as vasculitis or scleroderma.
• In these settings, the elevation in blood pressure results from ischemia-induced activation
of the renin-angiotensin system rather than volume expansion.
• A patient presenting with acute renal failure, hypertension, and red cells and red cell casts
in the urine sediment almost certainly has either glomerulonephritis or vasculitis.
• The absence of edema in this setting would point strongly toward a primary vascular
disease.
Chronic renal failure
• Hypertension is present in approximately 80 to 85 percent of patients with chronic renal
failure.
• Data from the Modification of Diet in Renal Disease Study, showed that the prevalence of
hypertension rose progressively from 65 to 95 percent as the GFR fell from 85 to 15 mL/min
per 1.73 m
2
• Hypertension may occur or be exacerbated in patients with advanced chronic renal failure
treated with erythropoietin.
• Patients with end-stage renal disease are more likely to have an increase in pulse pressure
and isolated systolic hypertension (? increased aortic stiffness).
• Targets of antihypertensive treatment in patients with renal disease
• 130/80 mmHg
• if proteinuria > 1g/day lower target values lowering proteinuria to values as near to normal
as possible
• to reduce proteinuria ACEi,ARB or combination are required
• Guidelines for the management of arterial hypertension J.Hypertens. (2007) 25:1105
• The desired degree of blood pressure control can usually be safely achieved with combined
therapy:
– ACE inhibitor or angiotensin II receptor blocker
– a diuretic,
– a calcium channel blocker,
– and, a beta blocker.
- THE KIDNEY IS AT HEART OF HYPERTENSION
- SAVE YOUR HEART BY PROTECTING YOUR KIDNEY
- DEPATMENT OF NEPHROLOGY AND HYPERTENSION
- HYPERTENSION CLINIC MOUSEL : PROFESSOR KHALID ABDULALLA 1970
- HEART – KIDNEY INTERACTION : THE CARDIO-RENAL SYNDROME
- PATIENTS WITH CKD HAVE HYPERTENSION AND ARE MORE PREDISPOSED
TO HEART ATTACKS , STROKES , AND CV MORBIDITY AND MORTALITY
THAN DEVELOPING ESRD
-ROBERT SCHRIER
-ISN LEADER
- KIDNEY DISEASE AND HIGH BLOOD PRESSURE ARE LINKED SO A COLLABORATION
BETWEEN ISN AND ISH –INTERNATIONAL SOCIETY OF HYPERTENSION – SEEMED NATURAL
Medicine is a social science and politics is nothing but medicine on a larger scale
RUDOLF VIRCHOW
(1821-1902
Aya