1
Dementia
Dementia is an acquired global impairment of intellect, memory and personality, but
without impairment of consciousness.
It is usually but not always progressive
Although dementia is global or generalized disorder, it often begins with focal cognitive or
behavioral disturbances
Most common causes: Alzheimer’s disease (50-60%), vascular dementia (20-25%), and
dementia with Lewy bodies (15-20%)
Both DSM-IV and ICD-10 definitions require impairment in two or more cognitive
domains (memory, language, abstract thinking and judgment, praxis, visuoperceptual
skills, personality, and social conduct) sufficient to interfere with social or occupational
functioning.
Deficits may initially be too mild or circumscribed to fulfill this definition.
The fluctuation in alertness which characterize delirium is usually absent, except in
dementia with Lewy bodies.
Causes of dementia
1. Primary neurodegenerative disorders: Alzheimer’s, Lewy bodies, Pick’s, Parkinson’s,
Prion diseses, Huntington’s disease.
2. Vascular: vascular dementia, multiple strokes, focal thalamic and basal ganglia strokes,
subdural hematoma
3. Inflammatory and autoimmune: SLE, Bahcet’s, MS, neurosarcoidosis
4. Traumatic : head injury
5. Infections and related conditions: HIV, neurosyphilis
6. Metabolic and endocrine : uremia, dialysis, hypothyroidism, hypoglycemia,
hypopituitarism, Cushing’s disease
7. Neoplastic
8. Post-radiation
9. Post- anoxic
Psychiatry
Organic disorders 2
Lecture
17
مشتاق .د
Al-Madena
Copy
2
10. Vitamin and other nutritional deficiencies : B12, folate
11. Toxic: alcohol , heavy metals, organic solvents
12. Other causes: normal pressure hydrocephalus
Clinical features
The presenting complaint is usually of poor memory
Other features include disturbances of behavior, language , personality, mood ,or
perception
Dementia is often exposed by a change in social circumstances or an intercurrent illness;
indeed,patients with dementia are especially susceptible for superimposed delirium.
Forgetfulness is usually early and prominent
Impaired attention and concentration are common and non-specific features
Difficulty in new learning is usually the most conspicuous feature.
Memory loss is more evident for recent than for more remote material
Loss is more in episodic memory (day-day events) while there is relative preservation of
procedural memory
Loss of flexibility and adaptability for new situations with the appearance of rigid and
stereotyped routines
As dementia progress patients became unable to care for themselves and they neglect
social conventions.
Disorientation for time and later for place and person is common
Behavior become aimless
Thinking slows and become impoverished in content and perseverative
False ideas often with persecutory kind appear and in later stages the thinking becomes
grossly fragmented and incoherent
Eventually patient may become mute
Behavioral , affective, and psychotic features accompany the cognitive deficits during
dementia.
Mortality is increased with death often following bronchopneumonia and a terminal coma
3
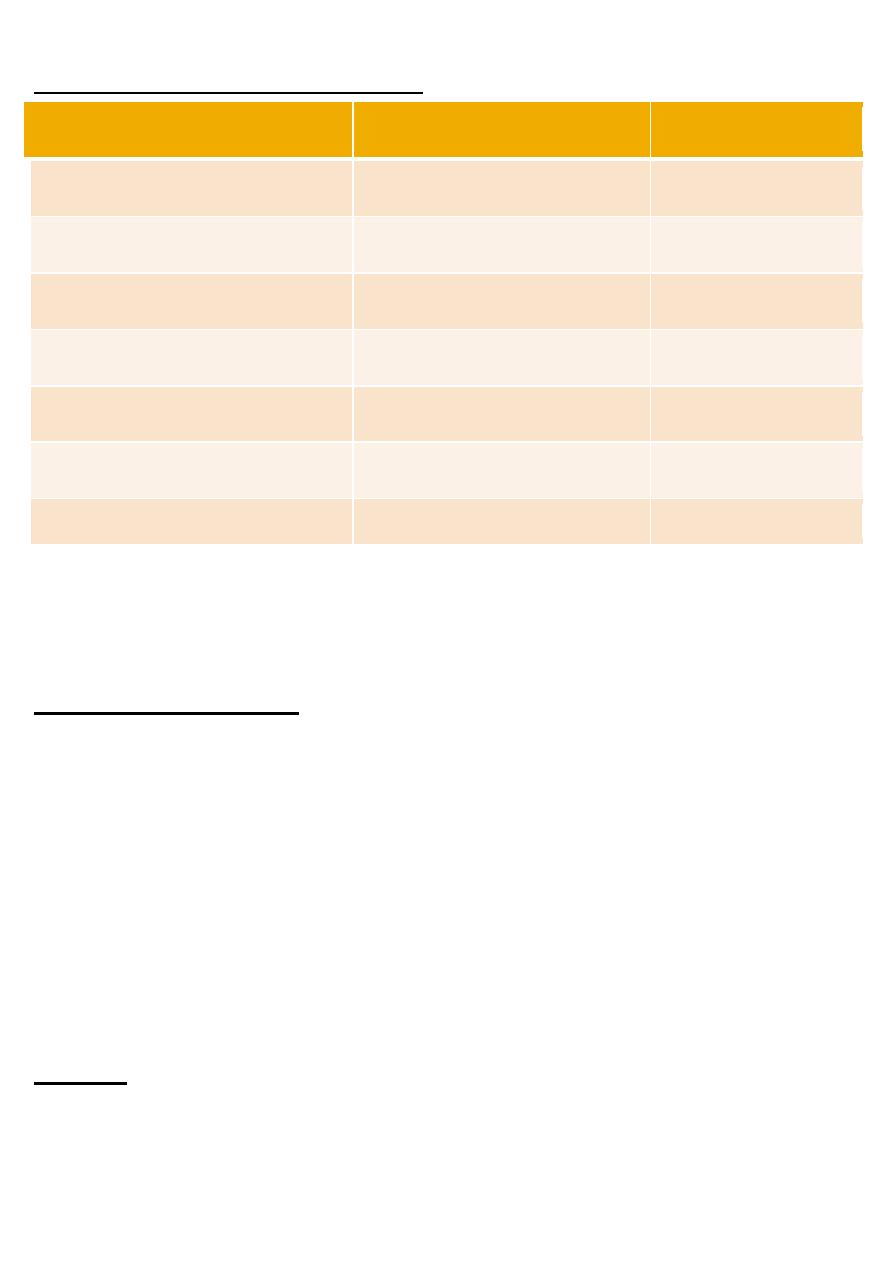
Subcortical and cortical dementia
subcortical
cortical
memory
moderate
Severe , early
language
normal
Dysphasias , early
personality
Apathetic, inert
indifferent
mood
Flat, depressed
normal
coordination
impaired
normal
Cognitive and motor speed
slowed
normal
Abnormal movements
Common, choreiform or tremor
rare
In all patients: full blood count, ESR, urea and electrolytes, liver function tests, calcium
and phosphate, thyroid function tests, syphilis serology, urinalysis, B12 and folate.
Worth considering: HIV status, chest radiograph , EEG, CT & MRI of brain, ECG,
neuropsychological assessment
Treatment of dementia
A-Drug therapy for cognitive deficits:
1. Cholinesterase inhibitors: can decrease the cognitive defects in 60%of patients like tacrine(
risk of liver damage is high) which lead to incompliance ,and donepezil( aricept) which has
less severe side effects.
2. Vitamin E :which can decrease the rate of functional decline.
3. Selegiline:MAO B inhibitor which delays cognitive deterioration . Its major defect is
orthostatic hypotension .No need for dietary restriction.
B – Drug therapy for psychosis and agitation : antipsychotic drugs like risperidone and
clozapine. Also benzodiazepines like lorazepam for sleep disorders.
Anticonvulsant agents, antiandrogens( medroxyprogesterone) for disinhibited sexual
behavior.
C -antidepressants
epilepsy
Epilepsy is the tendency to recurrent seizures
4
A seizure is consisting of a paroxysmal electrical discharge in the brain and its clinical
sequelae.
The tendency to recurrent seizures in epilepsy should be distinguished from isolated
seizures due to : drugs, hypoglycemia, and intercurrent illness.
Psychiatric problems of epilepsy
Psychiatric co-morbidity is common in people with epilepsy, with overall rates increased at
least two folds.
Many different types of psychiatric disorders are associated with epilepsy, including
cognitive ,affective ,emotional and behavioral disturbances.
These can occur before, during, after, and in between seizures.
The relationship between epilepsy and psychiatric disorders can be reflected in : a shared
etiology (temporal lobe pathology can cause both epilepsy and psychosis), the effects of
stigma, and the side effects of antiepileptic drugs that might cause psychiatric problems.
Pre-ictal psychiatric disturbances
Called prodromal states
Mood disturbances
Increasing tension , irritability
Anxiety and depression
Usually occur several hours or even days before a seizure ,and usually increasing in
severity as the seizure approaches.
Ictal psychiatric disturbances
In complex partial seizures there might be affective disturbances, hallucinations, anxiety
,automatism
Absence seizures : altered awareness and automatism
Post- ictal disturbances
Impaired consciousness
Delirium
Psychosis
Inter-ictal disorders
Not related to the occurrence of fits
Cognitive problems
Psychosis
Sexual problems
Depression
Suicide and deliberate self harm
Personality change
5
Head injury
There are two main groups of patients who have suffered head injury:
1. The relatively small group with persistent serious cognitive and behavioral sequele
2. A larger group with emotional symptoms and personality change
Acute psychological effects
Occur after recovery from coma
Delirium
Delusional misidentification
Agitation and disinhibition
Inappropriate sexual behavior
Chronic psychological effects
Post-concussional syndrome: a group of symptoms include anxiety, depression and
irritability, accompanied by headache, dizziness, fatigue , poor concentration, and
insomnia. It might be psychologically based and usually resolve spontaneously.
Lasting cognitive impairment: deficits in memory and executive functions ( planning,
problem solving, organizing, etc…)
Personality change: irritability , apathy, loss of spontaneity and drive, disinhibition, and
decreased control of aggressive impulses.
Emotional disorder: depression , anxiety, and emotional lability.
Psychosis: may be transient or chronic
Boxing and head injury: 10-20% of professional boxers develop what is called punch
drunk syndrome or dementia pugilistica.
This case is added by the student and not included in the lecture
A 74-year-old woman is brought to the clinic by her daughter-in-law. The woman is a regular
patient and has
A long history of hypertension and ischemic heart disease. She lives with her son and daughter-
in-law, who
Are concerned that she has become increasingly forgetful over the past year. Initially, they
attributed her
Forgetfulness to normal aging but her memory impairment has progressively worsened over the
past several
Months. Of late, she has also developed some difficulty performing activities of daily living, and
is no longer
Able to cook. Which one of the following is the most likely diagnosis?
A. Alzheimer's dementia
B. Multi-infarct dementia

6
C. Normal pressure hydrocephalus
D. Pick's disease
E. Pseudodementia
F. Age-related changes
Explanation
Alzheimer's dementia causes a gradually progressive cognitive decline that presents with memory
Impairment and one or more of the following: apraxia (difficulty in carrying out activities),
aphasia (language
dysfunction), agnosia (difficulty in recognizing objects), or disturbed executive functioning
(organizing,
planning, abstraction). Before making a definitive diagnosis of Alzheimer's disease, potential
medical causes
of cognitive decline should be ruled out first
the correct answer is A