THE HEAD
The scalp:
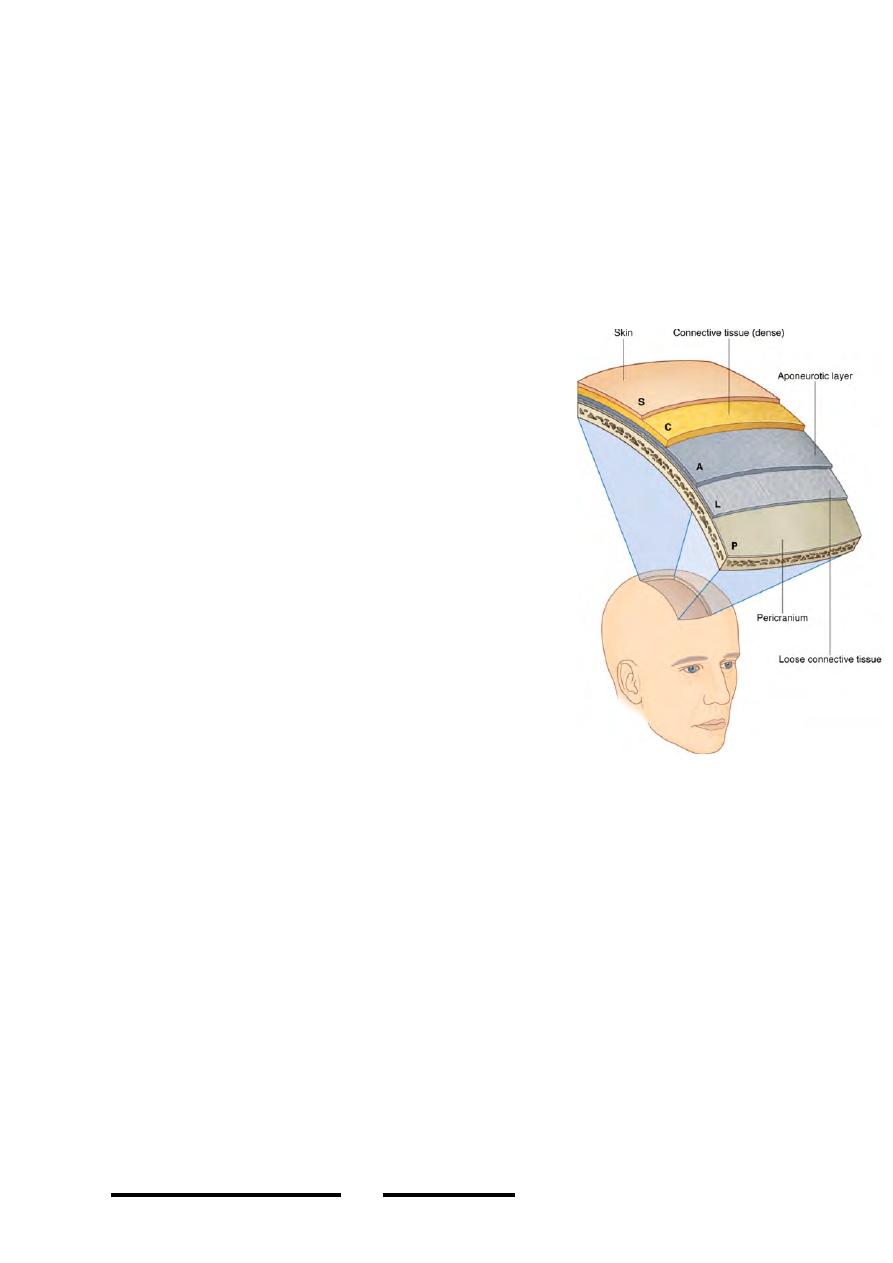
Is a five-layered structure covering the vault of skull & bears the hair of the head, its
name is derived from its 5 layers which are:
o
Skin
o
Connective tissue (subcutaneous connective
tissue)
o
Aponeurosis ( galea aponeurotica of occipito-
frontalis muscle)
o
Loose areolar tissue (subaponeu. space
o
Periosteum (pericraneum)
Skin:
•
Thin, hairy with generous amount of sweat &
sebaceous glands
•
Firmly adherent to the next layer
Subcutaneous connective tissue:
•
Thick layer made of connective tissue septa in all
directions to form a dense network enclosing
fatty loculi
•
Hair follicles pierce this layer
•
Arteries, veins & nerves of the scalp lie in this
layer and are held in position by the firm fibrous
network
•
Adheres to the layer deep & superficial to it, so the three layers could not be
separated from each other & move together when moving the scalp
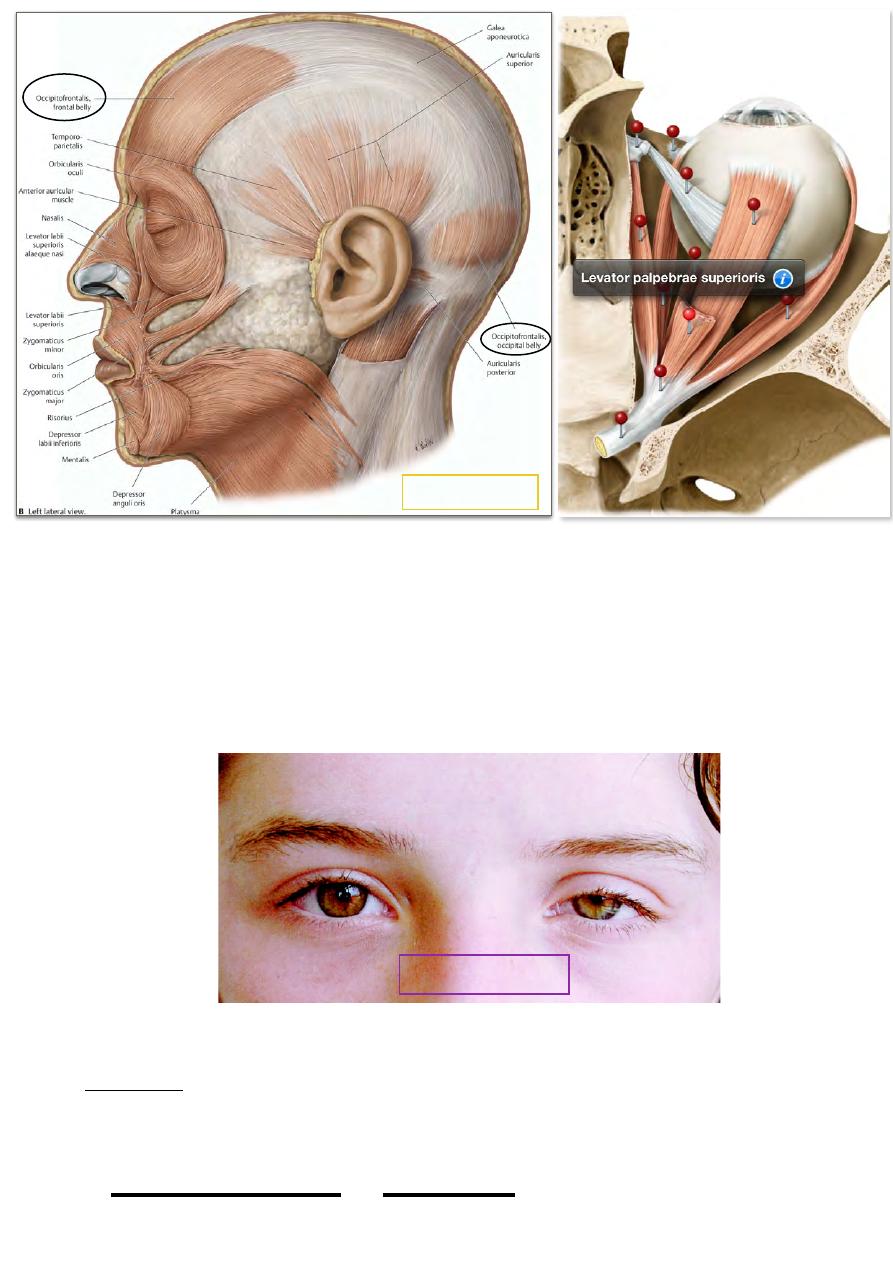
Epicranial aponeurosis:
•
A musculo-aponeurotic layer formed by the 4 bellies of occipito-frontalis
muscle connected by their galea aponeurotica
•
Occipito-frontalis:
-
The muscle arises by two bellies from the highest nuchal lines posteriorly
-
The 2 bellies are inserted into the back of the aponeurosis which is formed of
sagittally running fibers. From the anterior end of the aponeurosis the two
frontal bellies arise and go forward to be inserted into the skin of eyebrows &
root of the nose
-
The muscle is innervated by facial nerve (posterior auricular branch to
occipitalis & temporal branch to frontalis)
-
It acts to pull the scalp backward & elevate the eyebrows as in surprise
expression.
!
24
Head & Neck Dr. Nawfal K. Al-Hadithi
Subaponeurotic space:
• Extensive space lies beneath the galea & contains loose areolar tissue
• Movements of the superficial three layers take place in this plane
• It is only limited by the attachment of the galea
• anteriorly it is continuous with the eyelids & eyebrows
• Fluid accumulation in this space tend to go to the dependent areas, i.e; over the
occipital bone posteriorly & in the eyelids anteriorly (if blood causes black
eye)
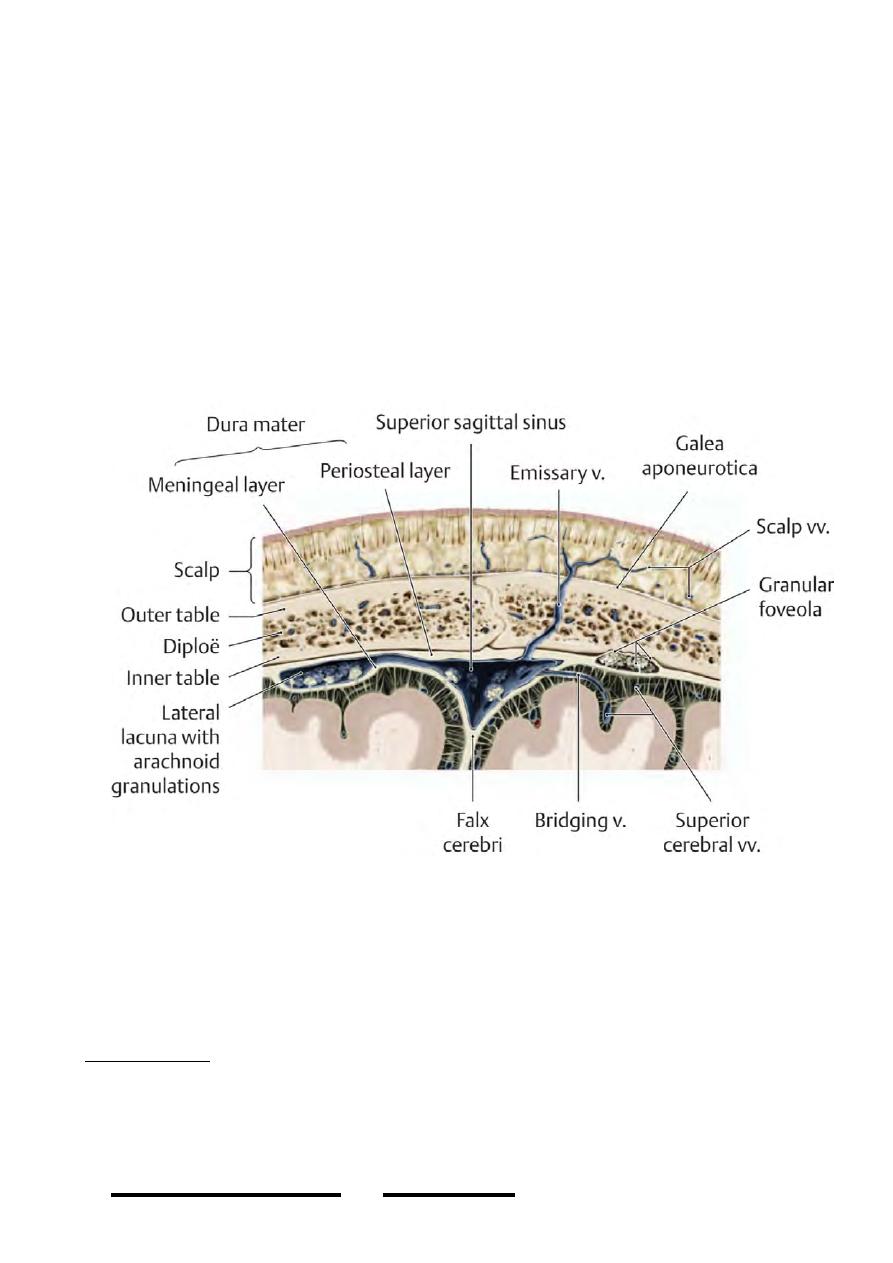
Pericraneum:
• Is the periosteum of skull bones
• Is firmly adherent to the sutures
• Bleeding deep to this layer takes the shape of underlying bone
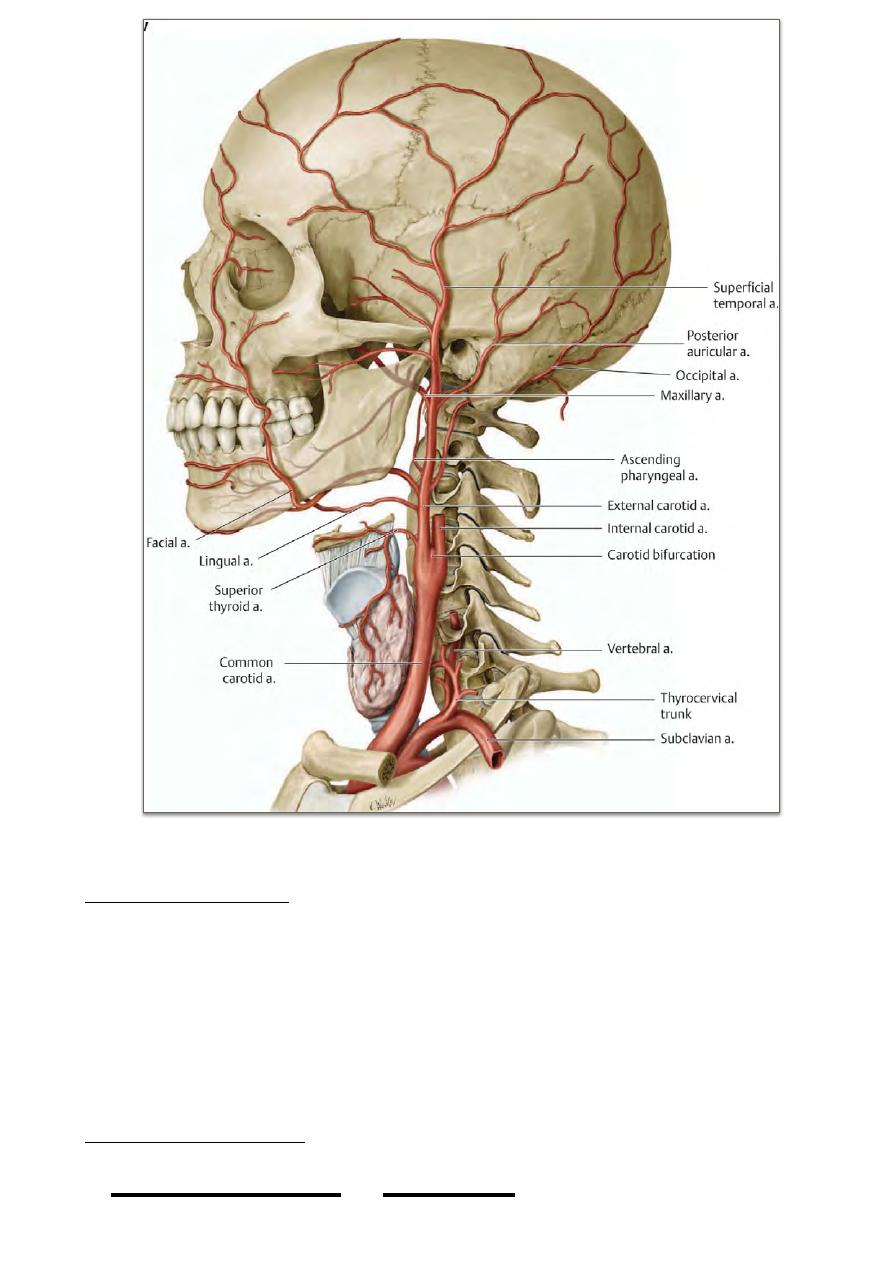
Arteries of the scalp:
- Branches from the ECA & ICA supply the scalp and anastomose freely with
each other & with those of the opposite side
- Arteries are held by the fibrous septa of the 2nd layer which pull them &
prevent their contraction when severed.
Branches of ECA:
1- Occipital a.;
- From the back of ECA goes deep to the posterior belly of digastric then in the
apex of the posterior triangle grooving the occipito-mastoid suture on the skull
then in the roof of the suboccipital triangle where it accompanies the greater
occipital nerve to reach the scalp
!
25
Head & Neck Dr. Nawfal K. Al-Hadithi
- It divides into medial & lateral terminal branches which supply the scalp up to
the vertex.
2- Posterior auricular a.;
- From the back of the ECA just above the posterior belly of digastric
- It passes superficial to the styloid process to lie in the groove between the
mastoid process & the external auditory meatus
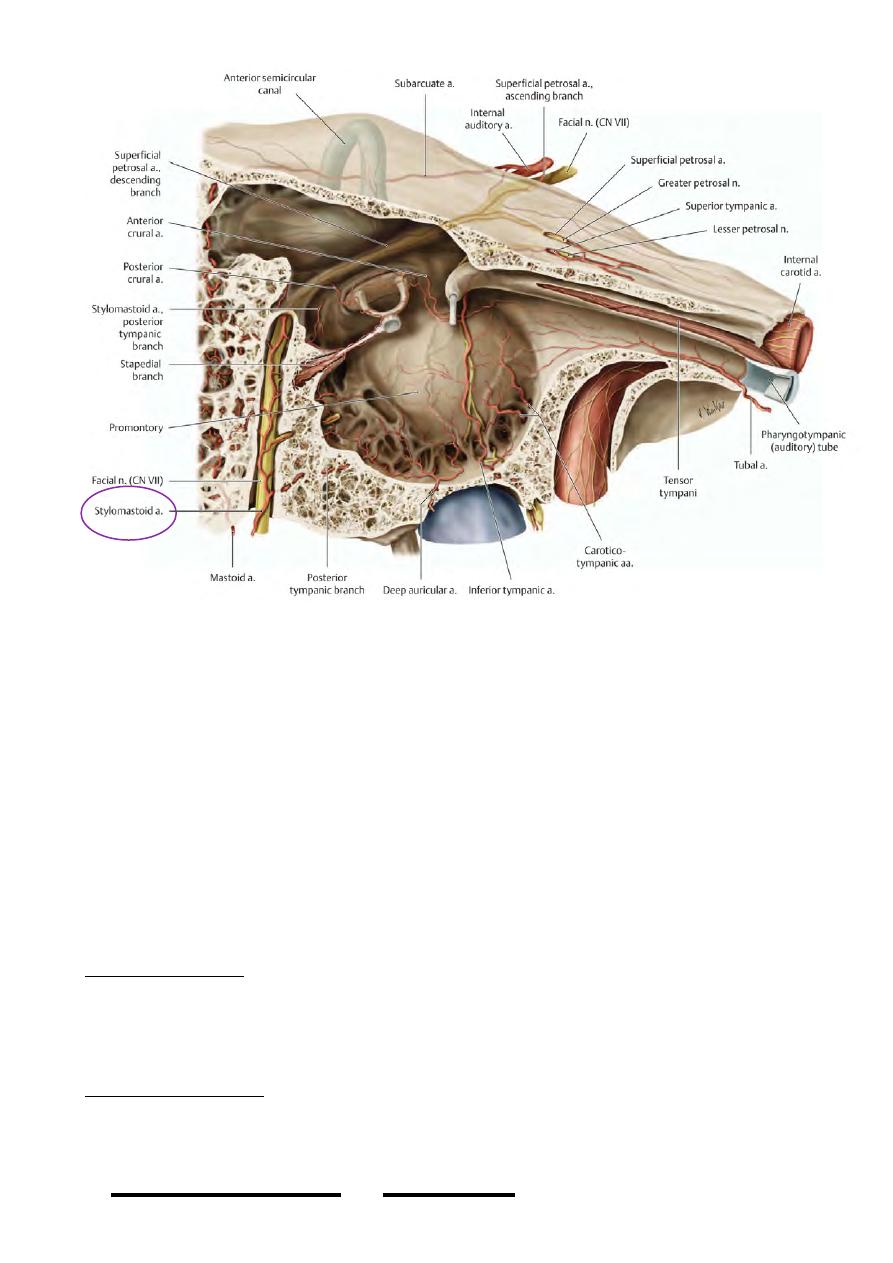
- Its branches are:
- Stylomastoid: enters the stylomastoid foramen & supplies the tympanic cavity,
antrum & mastoid cavities.
- Auricular: supplies the auricle, posterior part of temporal area.
- Occipital: supplies the skin over the mastoid process & occipitalis.
3- Superficial temporal a.;
!
26
Head & Neck Dr. Nawfal K. Al-Hadithi
- The smallest of the 2 terminal branches of ECA
- From behind the neck of mandible the artery grooves the root of the zygomatic
arch with the auriculotemporal nerve
- Ascends in the temporal fossa to end 5 cm above the zygomatic arch by
dividing into frontal & parietal branches. Its branches are:
- Transverse facial: from its anterior aspect this artery passes over masseter between
the parotid duct & zygomatic arch supplying all structures in the region.
- Middle temporal: arises above the root of the zygomatic arch & perforates the
temporal fascia & muscle to lie directly on the squamous temporal bone grooving it
with its accompanying vein.
- Zygomatico-orbital, anterior auricular & terminal branches supply muscles & skin
in their regions.
Branches of ICA:
1- Supra-orbital a.;
- from the ophthalmic artery this branch leaves the supra-orbital notch to supply
the scalp up to the vertex
- It anastomose with the termination of facial artery (angular a.) & the frontal
branch of superficial temporal artery.
2- Supra-trochlear a.;
- From the ophthalmic artery this branch leaves the supra-orbital notch with the nerve
of its name to supply the middle of the forehead.
!
27
Head & Neck Dr. Nawfal K. Al-Hadithi

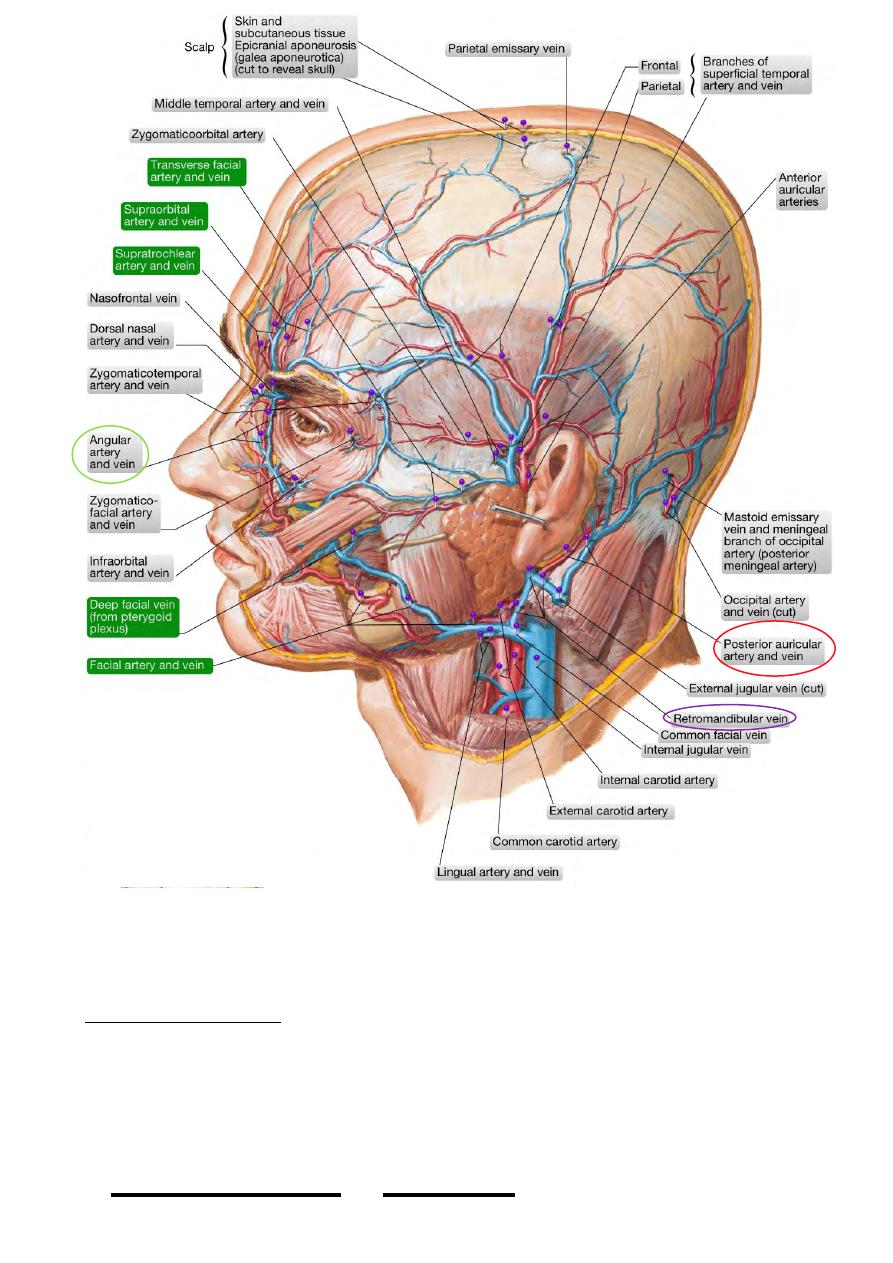
Veins of the scalp:
- Accompany the corresponding arteries
- Anastomose freely with their
adjacent veins of the same side & of
the opposite side.
1- Supratrochlear v.; unite at the medial
canthus with the supra-orbital v. of its same
side to form the angular v. which descends
in the face as the facial vein.
2- Supra-orbital v.; is connected (before
forming the angular v.) to the superior
ophthalmic vein in the orbit which drains to
the cavernous sinus
3- Superficial temporal v.;
- Accompanies the artery & receives
branches similar to those of the
artery.
- Behind the neck of the mandible it
receives the two maxillary veins to
form the retromandibular v. which enters the parotid gland.
4- Posterior auricular v.; larger than the corresponding artery, it descends to meet the
posterior division of retromandibular v. forming the EJV.
!
28
Head & Neck Dr. Nawfal K. Al-Hadithi
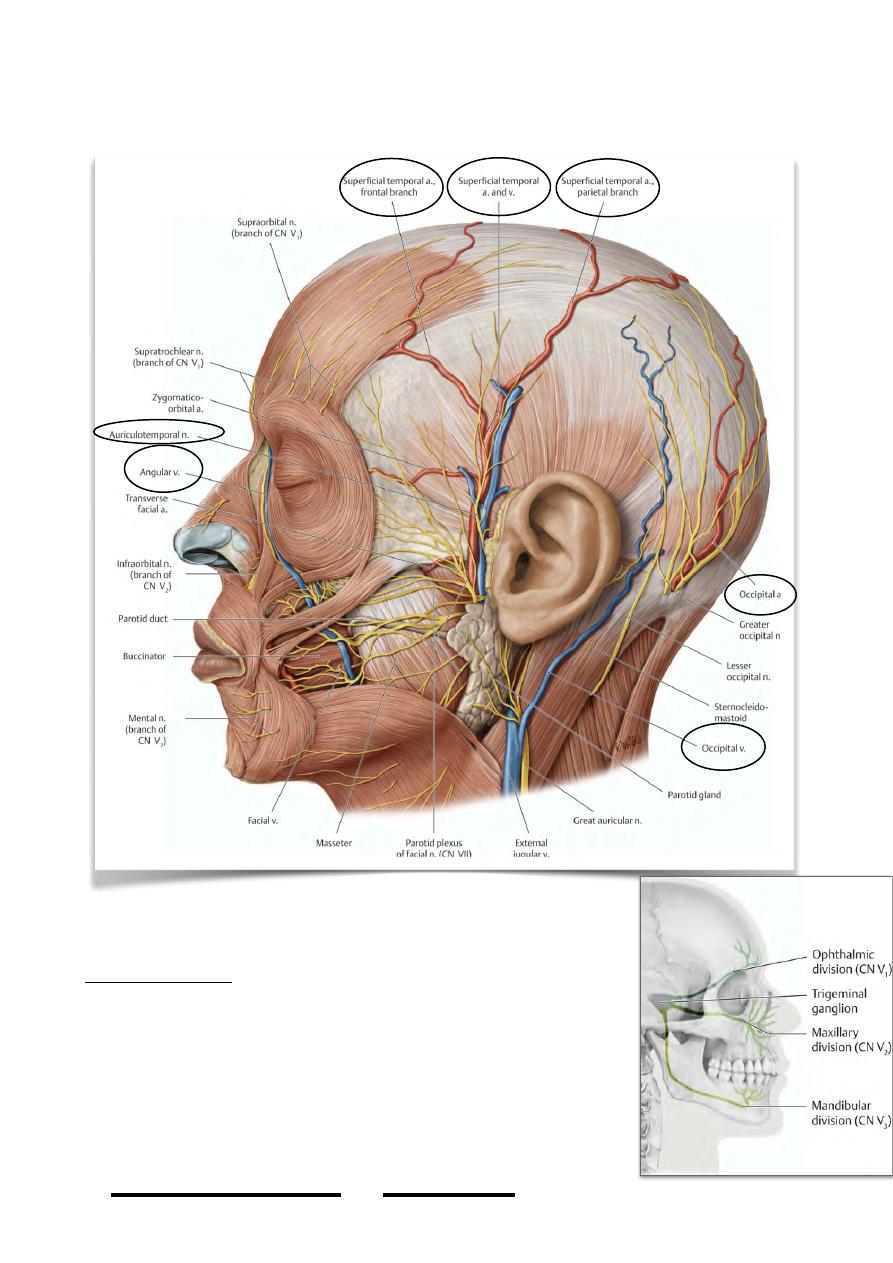
5- Occipital v.; accompanies the artery an ends in the deep cervical & vertebral
venous plexus. Occasionally it ends in the IJV.
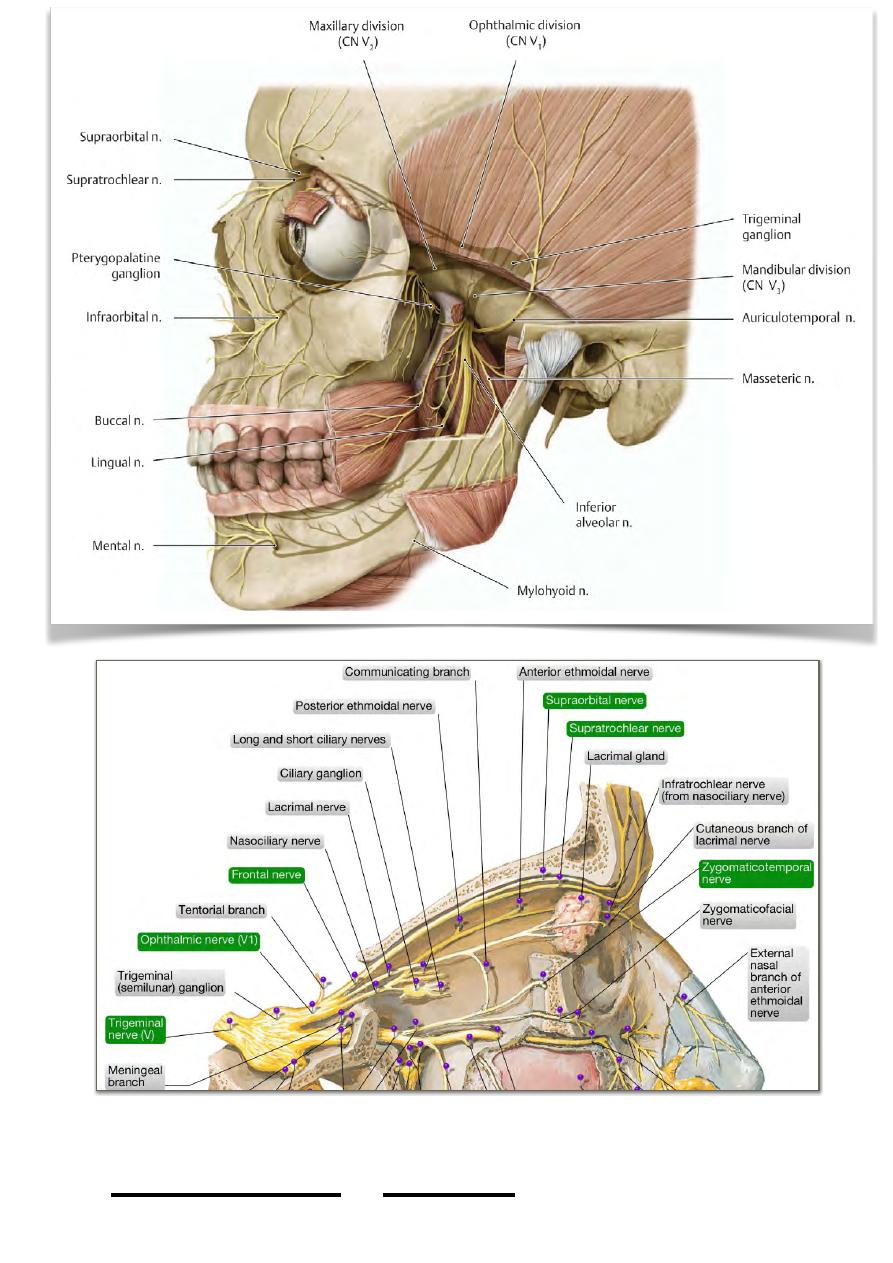
Nerves of the scalp:
Trigeminal nerve supplies the anterior part of the scalp up to
the vertex by branches derived from its three divisions:
1- Ophthalmic division :
- Supratrochlear n.; supplies the middle of the forehead up
to the hairline.
- Supra-orbital n.; supplies the lateral part of the forehead
& meets its opposite fellow above the distribution of the
supratrochlear n. to supply the scalp up to the vertex.
!
29
Head & Neck Dr. Nawfal K. Al-Hadithi
!
30
Head & Neck Dr. Nawfal K. Al-Hadithi
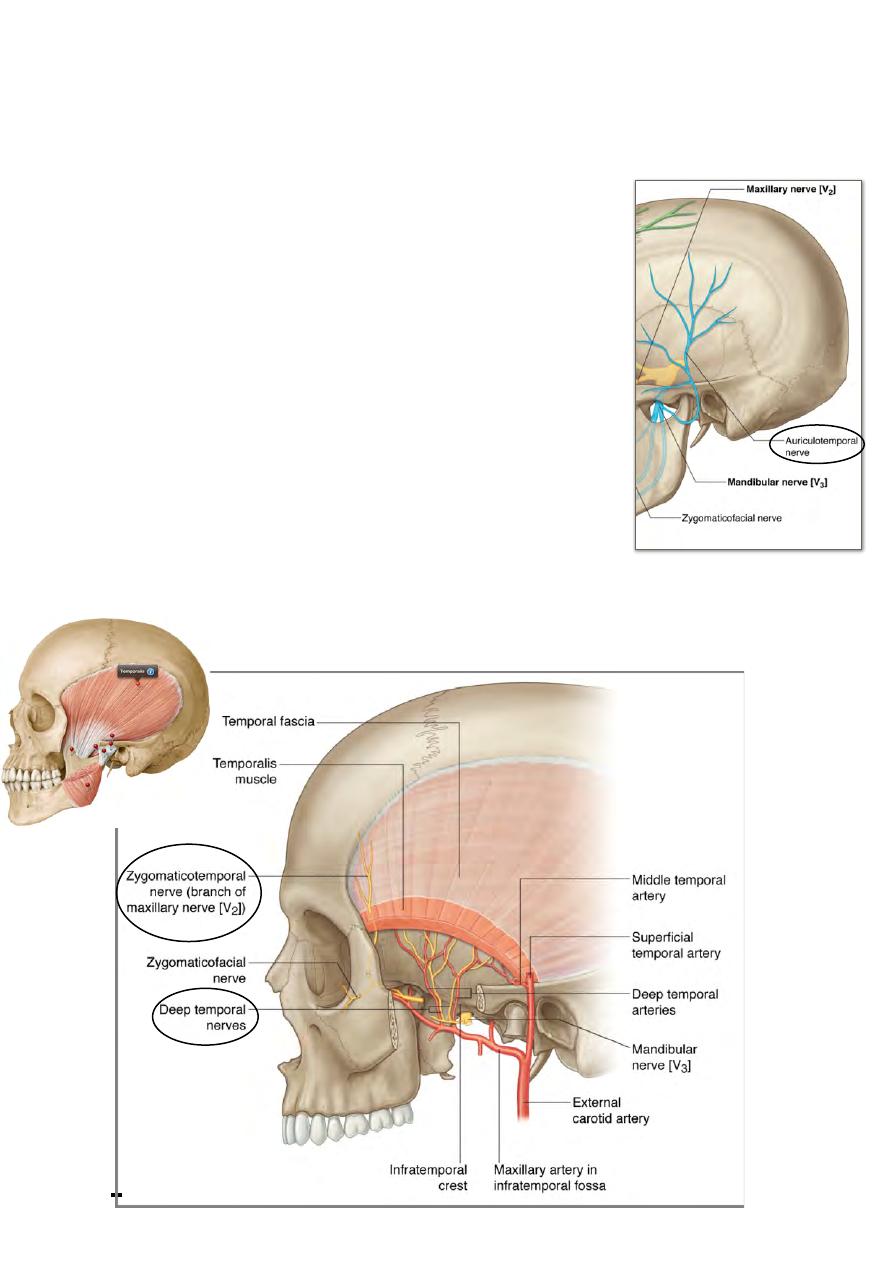
2- Maxillary division:
Zygomatico-temporal n.; supplies the non hairy part of the temple.
3- Mandibular division:
Auriculotemporal n.; from the infratemporal fossa this nerve accompanies the
superficial temporal a. & crosses the root of the zygomatic arch to ascend in the
temple. It supplies the upper half of the auricle externally, parotid gland & the hairy
temple.
Posterior primary rami of C2 (greater occipital n.) and “to lesser amount” C3 supply
the back of the scalp up to the vertex.
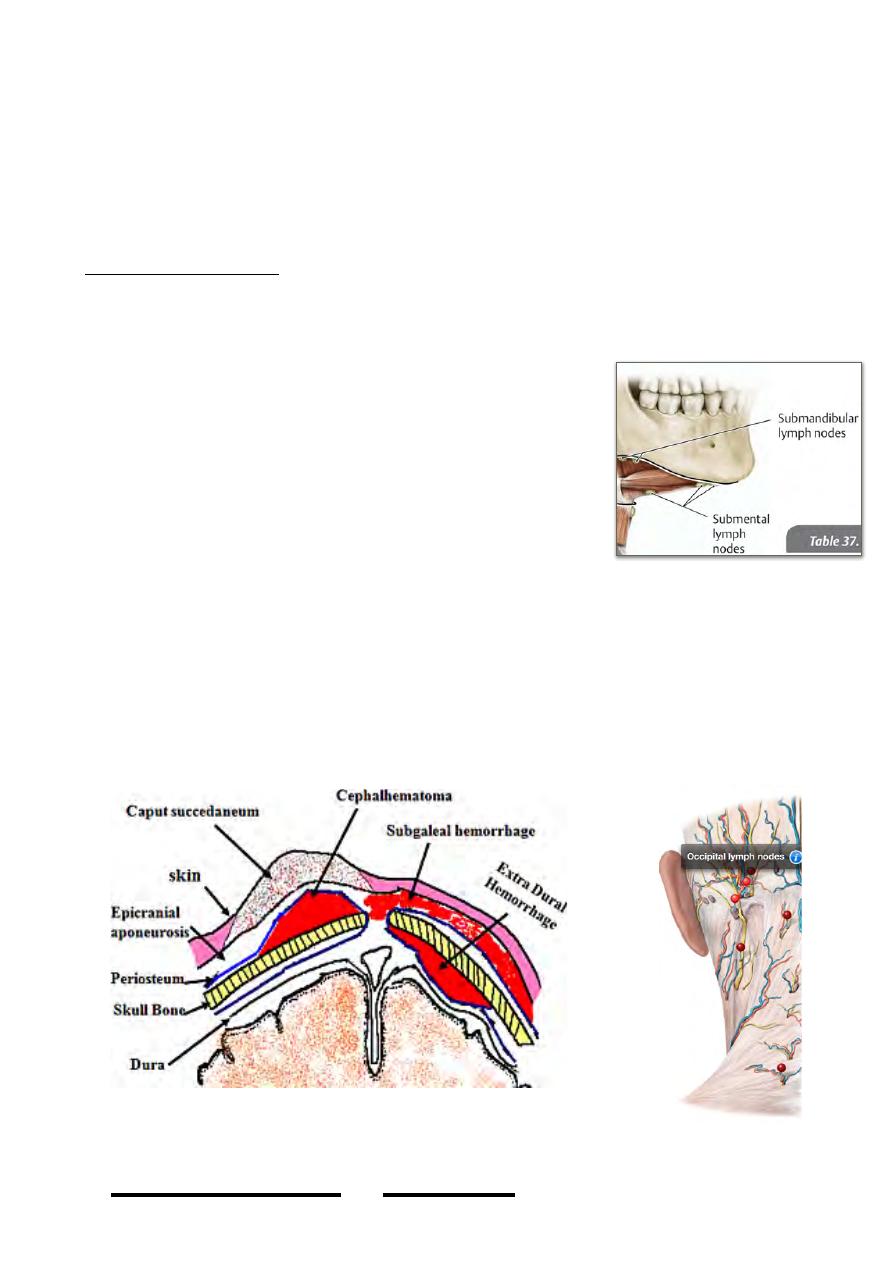
Lymph of the scalp:
- Anterior & lateral parts to the submandibular L.N
- Posterior part to the occipital L.N
Applied anatomy:
• Wounds of the scalp opens the 3 superficial layers
therefore they have two main characteristics:
1- Open widely, due to the stretch effect of the aponeurosis.
2- Bleeds profusely, because the scalp is rich in blood
vessels which lie in the second layer & this layer is stretches
by the aponeurosis so the vessels tear more & hemostasis
will be difficult.
• Because the scalp moves freely on the bone, the superficial injuries may not
coincide with deep ones.
• Subaponeurotic hematoma will descend in the dependent areas leading to black
eyes & posterior hematomas
• Subperiosteal hematomas take the shape of the underlying bone.
• Anastomosis between the ECA & ICA in the scalp is at a sagittal line which
lies above the lateral end of the eyebrow, bleeding here is very profuse.
!
31
Head & Neck Dr. Nawfal K. Al-Hadithi

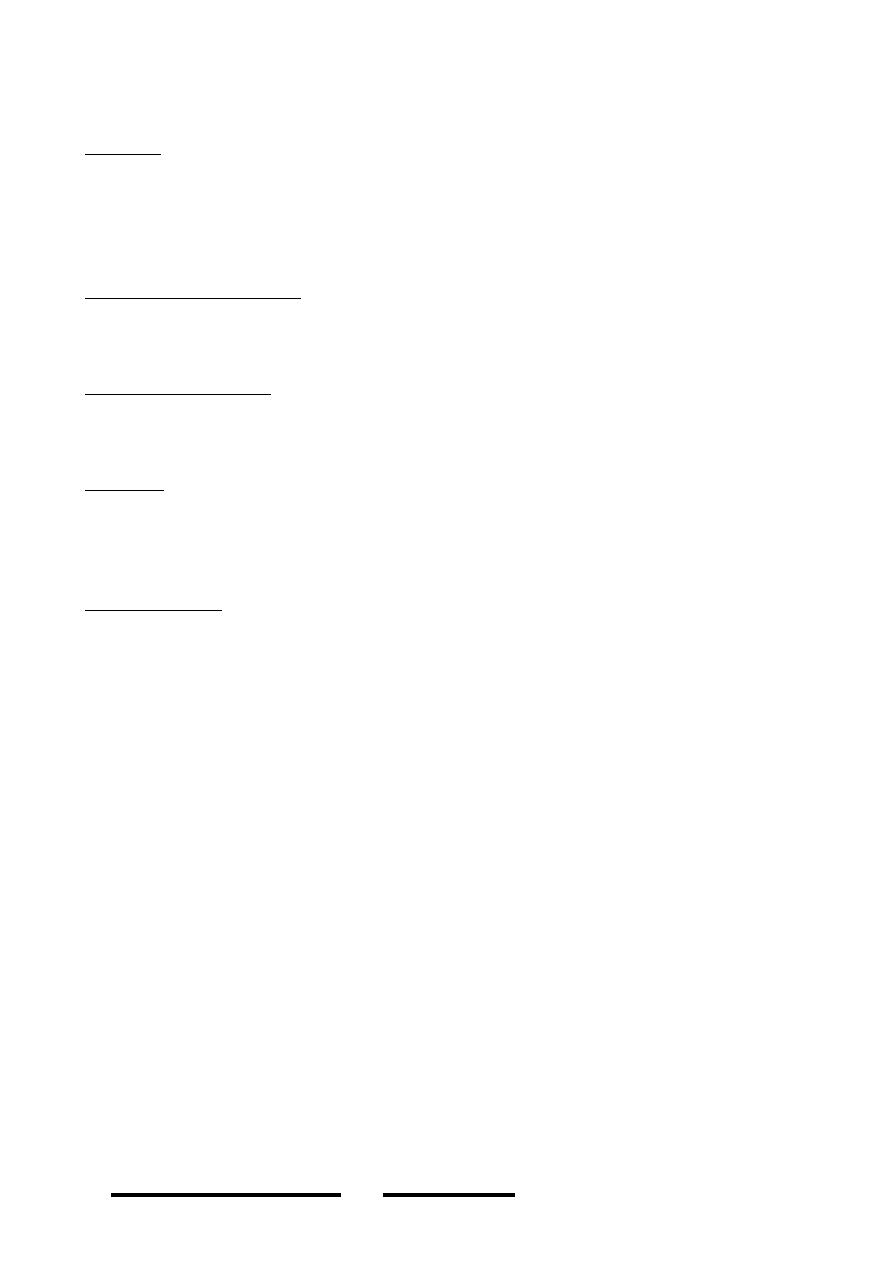
• The face:
• Muscles of Facial Expression:
- The face lacks deep fascia & its superficial fascia is modified
into muscles whose one end is attached to bone “usually” & the
other to the facial skin which they move producing various
movements.
- The superficial muscles of the face are arranged around facial
orifices (palpebral fissure, nostrils & oral fissure) as two groups
around each orifice, dilator & constrictor.
- Man has trained himself to express & understand some facial
movements produced by some of these muscles
- Many facial muscles produce no expression like buccinator,
indeed a very meaningful expressions are produced by
muscles not belonging to the face like genioglossus!!
I) Muscles of the palpebral fissure:
SPHINCTERS:
Orbicularis oculi:
- This muscle is formed of concentric fibers
which are arranged circumferentially
around the opening of the eyelid
- It is formed of three parts:
1- The orbital part:
- Arises from the medial orbital margin &
the medial palpebral ligament
- Spreads onto the forehead & cheeks
- It is the most peripheral part of the
muscle.
2- The palpebral part:
- Arises from the lateral end of the medial
palpebral ligament
- Course in the subcutaneous connective
tissue of the eyelids
- Interdigitate laterally forming the lateral
palpebral raphe.
3- The lacrimal part:
- From the posterior part of the medial palperal lig. & psterior lacrimal crest
- These fine fibers are inserted into the lacrimal sac & tarsal plates
* The medial palpebral ligament:
- Is a strong band , 5 mm long
- Arises from the frontal process of the maxilla & extends laterally to divide into
2 slips each one is continuous with its corresponding tarsal plate
Nerve supply:
- Facial nerve supplies the muscle by its temporal & zygomatic branches
Action:
!
32
Head & Neck Dr. Nawfal K. Al-Hadithi
Facial
expression of
genioglossus

- Orbital part; depresses the eyebrows & protects from light as in looking from
distance
- Palpebral part; closes the eyelids gently as in blinking
- Lacrimal part; squeezes the lacrimal sac
- ALL the parts; close the eyes forcibly as in protection from accidents
- DILATORS:
- Frontalis:
- Discussed. It is the opponent of the orbital part of O. oculi.( raise the
eyebrows)
- Levator palpebrae superioris:
- This muscle is the opponent of the palpebral part of O. oculi.(open the eyelids)
- Origin; From the back of the orbit in front of the optic canal
- Insertion;
- The muscle broadens as it traverses the uppermost part of the orbit forward to
enter the upper eyelid
!
33
Head & Neck Dr. Nawfal K. Al-Hadithi
=lateral
palpebral raphe
- It is inserted into the upper part of the orbital septum & O. oculi.
This muscle is formed of skeletal (voluntary component) & smooth muscle fibers
(involuntary component), the latter is responsible for its unconscious prolonged &
sustained contraction in opening the eyes for long time without fatigue.
Nerve supply:
- Skeletal part: superior division of oculomotor nerve
- Smooth muscle part: superior thoracic sympathetic ganglion (T1) whose injury
in “Horner’s syndrome” is responsible for ptosis in this condition.
II) Muscles of the nose:
DILATORS:
Corrugator:
Origin; the superciliary arch
Insertion; medial half of the eyebrow skin
Action; pulls the eyebrows medially producing vertical wrinkles
!
34
Head & Neck Dr. Nawfal K. Al-Hadithi
Frontalis muscle
Horner's syndrome

Procerus:
Origin; lower part of nasal bone & alar cartilage
Insertion; skin between the eyebrows
Action; pulls the skin overlying the root of the nose
downward
Alar part of nasalis:
Origin; canine eminence
Insertion; fibers ascend superomedially to meet its fellow
on the nose
Action; depresses & dilate nostrils
SPHINCTERS:
Septal part of nasalis (depressor septi):
Origin; maxilla, near the anterior nasal spine
Insertion; lower part of the septum
Action; pulls the septum down & diminishes the openings
of the nostrils
Nerve supply of nasal muscles:
Upper fibers: temporal branch of facial n.
Lower fibers: zygomatic & buccal branches of facial n.
III) Muscles of the oral fissure:
DILATORS:
Elevators of the upper lip:
Levator labii superioris alaeque nasi:
Origin; frontal process of maxilla
Insertion; partly in alar cartilage & partly in the
lateral half of the upper lip
Action; elevates the angle of the mouth & dilates
the nostril
Levator labii superioris:
Origin; inferior orbital margin above the infra-
orbital foramen
Insertion; lateral half of the upper lip
Action; elevates the upper lip
Zygomaticus major:
Origin; zygomatic bone anterior to the zygomatico-
temporal suture
Insertion; skin on the lateral side of the mouth & O.
oris
Action; draws the mouth superolaterally
Zygomaticus minor:
Origin; lower part of zygomatic bone
Insertion; upper lip, medial to the mouth angle
Action; elevates the upper lip
Levator anguli oris:
Origin; from the canine fossa
!
35
Head & Neck Dr. Nawfal K. Al-Hadithi
Insertion; the muscle lies deep to LLS ends in the mouth angle
Action; elevates the angle of the mouth
Risorius:
Origin; parotid fascia
Insertion; skin of the angle of the mouth
The muscle is a contribution of many muscles& it is an important landmark for
dentists.
Depressors of the lower lip:
Depressor labii inferioris:
Origin; mandible, medial to the mental foramen
Insertion; lateral side of the lower lip
Action; draws the lower lip downward & laterally
Depressor anguli oris:
Origin; oblique line of the mandible
Insertion; angle of the mouth
Action:depresses the mouth angle
Mentalis:
Origin; mandible, below the incisor teeth
Insertion; skin of the chin
Action; modifies the oral aperture indirectly by dimpling the skin of the chin.
SPHINCTERS:
Orbicularis oris:
Intrinsic part of O. oris (superficial part):
• Upper (maxillary) fibers from the alveolar process of the maxilla above the
incisor teeth, these fibers go laterally & wind around the angle of the mouth to
dip in the lower lip
• Lower (mandibular) fibers from the alveolar process of the mandible below the
incisor teeth, these fibers go laterally to wind around the mouth angle & ascend
in the upper lip
Extrinsic part of O. oris (deep part):
Formed by contributions from the dilators & buccinator
Action:
- Sphincter of the mouth
- Flattens the lip
- Protrudes the lip
Nerve supply of oral muscles:
- Above the mouth angle: zygomatic & buccal br. of VII
- Below the mouth angle: mandibular br. of VII
!
36
Head & Neck Dr. Nawfal K. Al-Hadithi
!
37
Head & Neck Dr. Nawfal K. Al-Hadithi
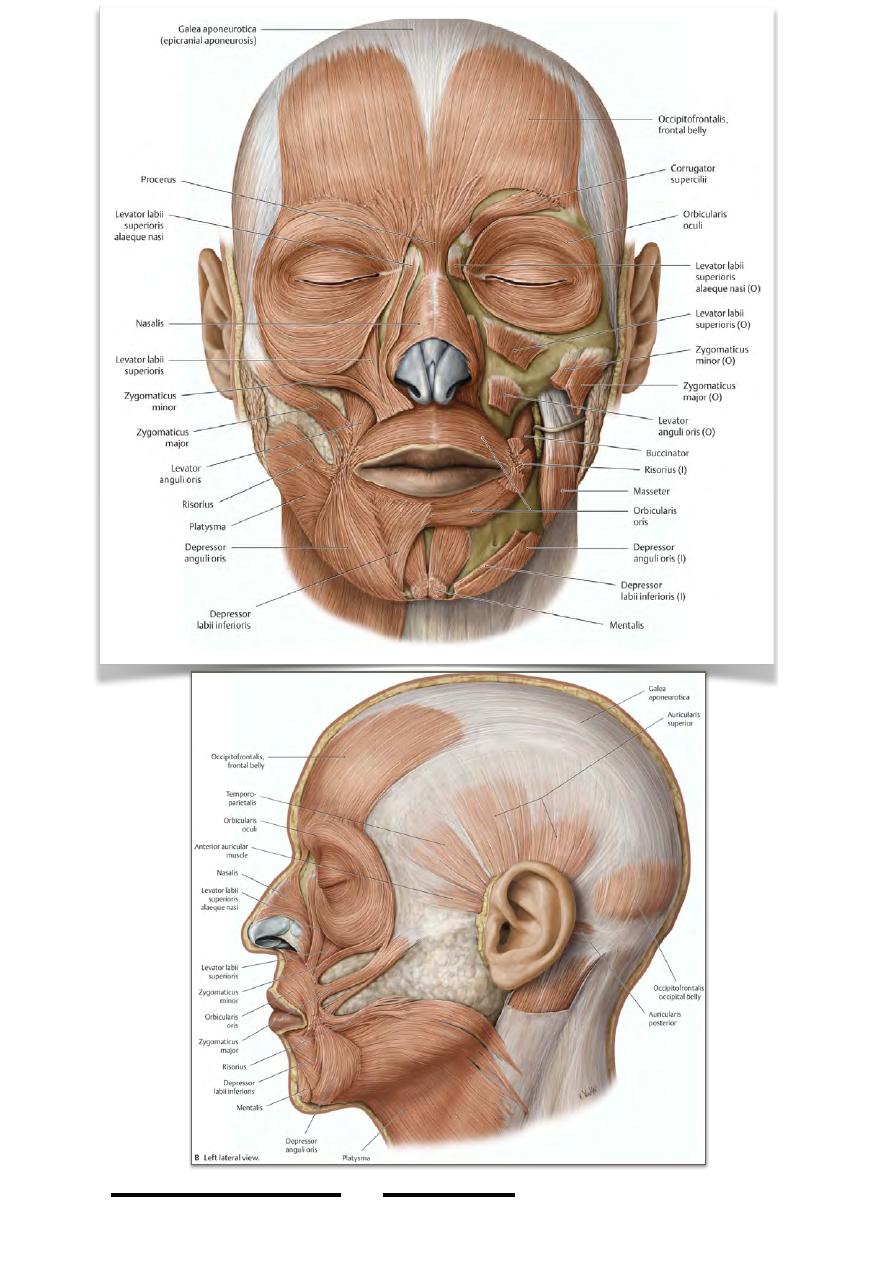
Buccinator:
This quadrilateral muscle lies in a deeper stratum than other muscles of the face &
forms the main bulk of the cheeks.
Origin; from 3 lines forming & C-shape origin:
• Alveolar process of maxilla in a line which overlies the upper molar teeth
(upper fibers)
• Alveolar process of the mandible in a line which lies parallel to the lower
molar teeth (lower fibers)
• Pterygomandibular raphe which extends from the pterygoid hamulus to the
deep surface of the mandibular angle (middle fibers) sharing this origin with
the superior pharyngeal constrictor muscle
Insertion; the most peripheral fibers of buccinator (upper & lower) pass directly into
the corresponding lip, while the middle fibers interlace at the angle of the mouth, the
upper go to the lower lip & the lower to the upper lip.
Nerve supply; buccal branch of facial nerve
Action; compresses the cheek & increases the intra-oral pressure, its paralysis tend to
accumulate food in the vestibule of the mouth.
• It is pierced by the parotid duct to which it gives a sphincter-like action
• The buccal branch of mandibular nerve is sensory to the muscle & ends in the
skin overlying it
All facial muscles are supplied by proprioception from the sensory nerves supplying
the overlying skin
!
38
Head & Neck Dr. Nawfal K. Al-Hadithi
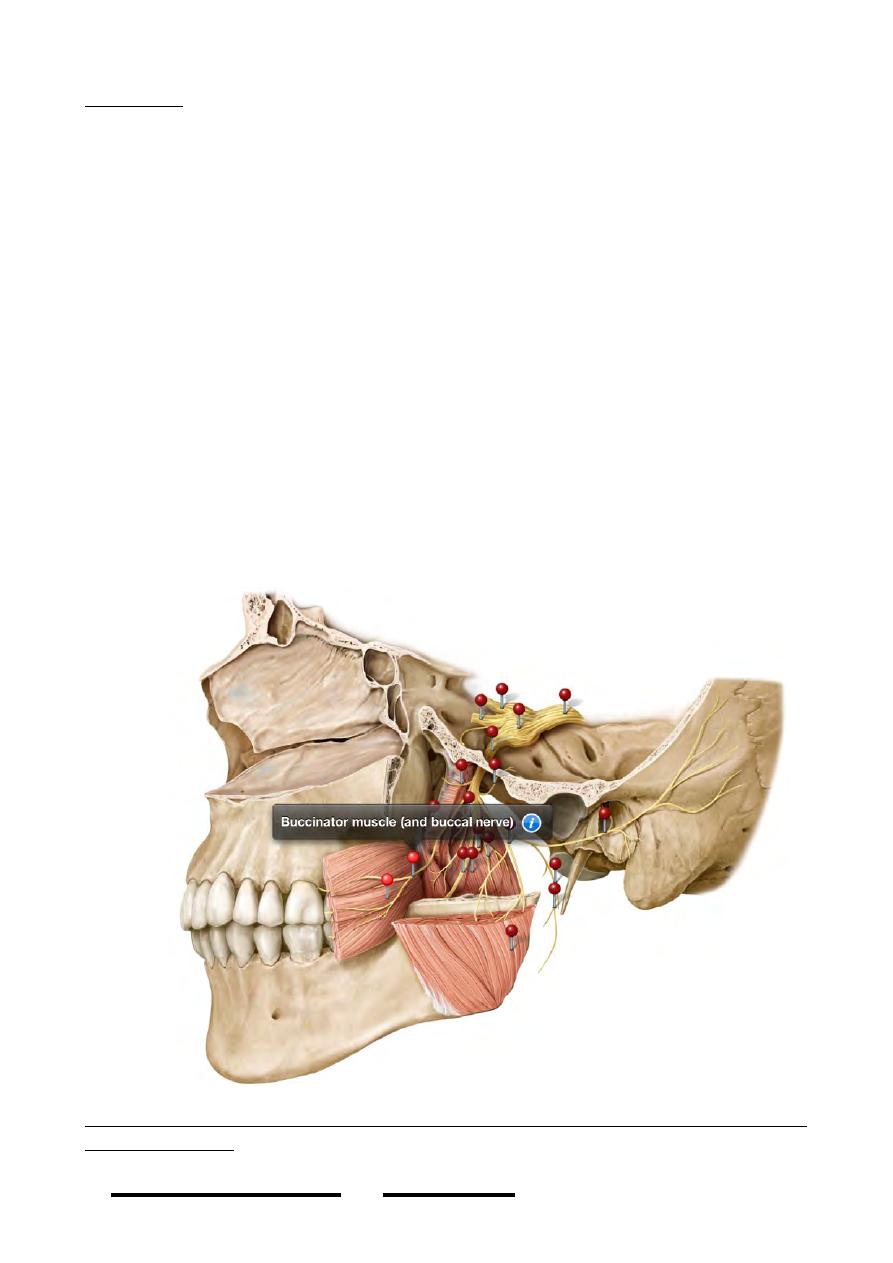
Arteries of the face:
Arteries of the face lie in the subcutaneous tissue . The main artery of the face is the
facial artery, other arteries which share in the supply of the face are:
1- Transverse facial artery.
2- Infraorbital artery.
3- Mental artery.
4- Buccal artery.
1- Facial artery:
• An anterior branch of the ECA leaving it deep to the posterior belly of digastric
muscle & passes in the submandibular triangle to reach the lower border of the
mandible where it curves up to the face.
• In the face the artery is superficial at its beginning
being covered only by skin & platysma.
• The artery ascends in a very tortuous course towards
the medial angle of the eye, its relation to the face
muscles is variable but usually it is superficial to
buccinator & levator anguli oris & deep to the
zygomatic muscles.
• The facial vein lies lateral to the artery & its course is
less tortuous.
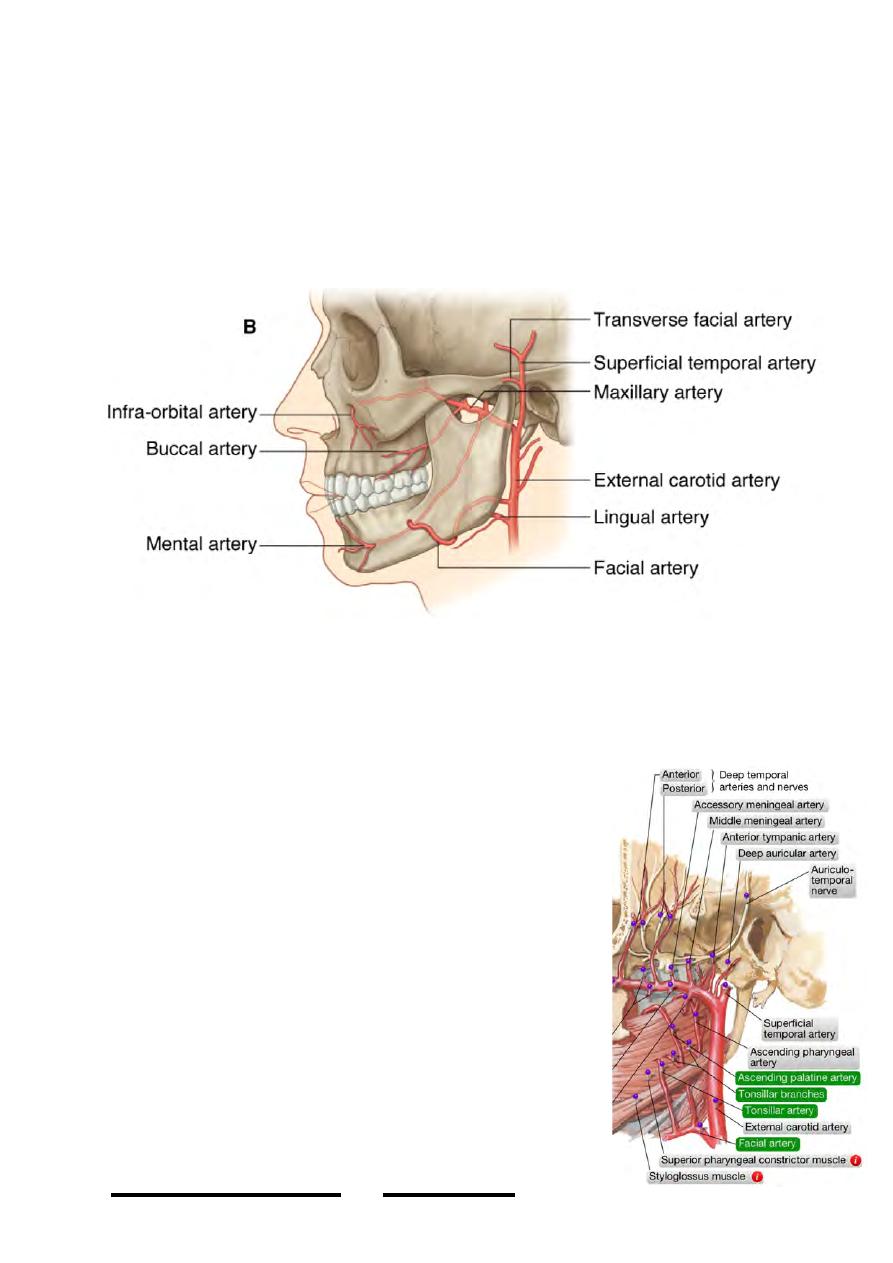
Branches of the facial artery:
I ) In the neck (do not reach the face):
a- Ascending palatine a.
b- Tonsillar a.
c- Muscular branches
d- Glandular branches to the submandibular gland
e- Submental a.
II ) In the face:
!
39
Head & Neck Dr. Nawfal K. Al-Hadithi
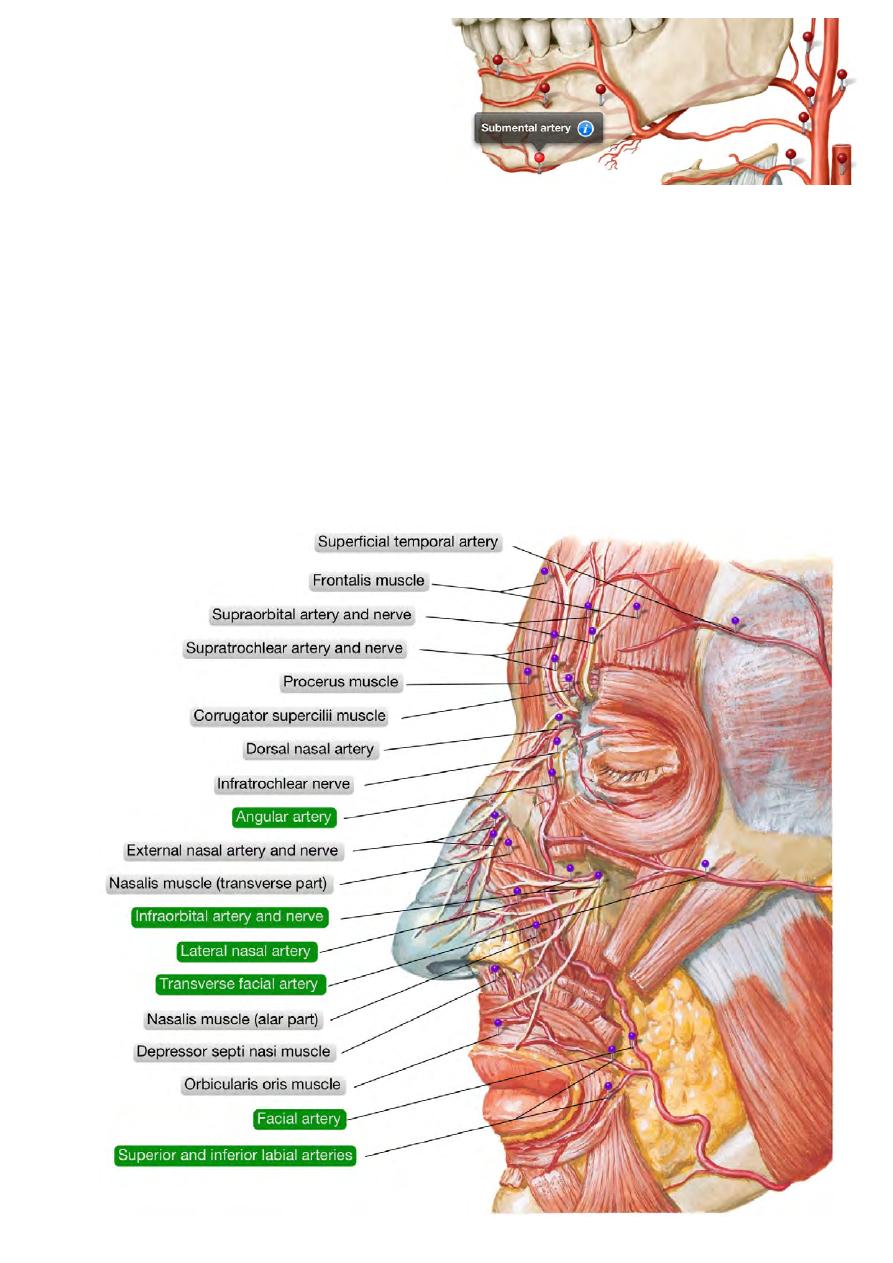
a- Inferior labial a.
b- Superior labial a.
c- Lateral nasal a.
d- Angular a.
- The labial branches:
• Arise opposite to the angle of the mouth & enter the corresponding lips
between O. oris & the mucous membrane
• Supply muscles, glands & mucous membranes of the lips
• Anastomose with labial branches of the opposite side
- Lateral nasal branch:
Arises alongside the nose
Supplies the ala & dorsum of the nose
Anastomose with the opposite artery, infraorbital a.
- Angular artery:
The terminal part of facial artery lies at the medial canthus
Supplies O. oculi & the lacrimal sac
Anastomoses with the infraorbital a.
!
40
Head & Neck Dr. Nawfal K. Al-Hadithi

2- Transverse facial artery. “discussed”
3- Infraorbital artery:
• One of the terminal branches of maxillary artery
• Leaves the infraorbital foramen & lies deep to
lavator labii superioris
• Gives palpebral, nasal & labial branches
4- Mental artery:
• Is the terminal branch of the inferior alveolar
artey
• Appears in the face from the mental foramen
deep to depressor anguli oris
•Supplies the chin
5- Buccal artery:
•A branch of maxillary
artery
•Accompanies its vein
& the buccal branch of
mandibular nerve to
r e a c h t h e a r e a o f
buccinator
•Supplies buccinator &
skin & m.m. of the
cheek
!
41
Head & Neck Dr. Nawfal K. Al-Hadithi

Veins of the face:
1- Anterior facial vein:
• Begins at the medial canthus as the angular vein by confluence of supraorbital
& supratrochlear veins
• Connected to the superior ophthalmic vein which joins it to the cavernous sinus
• Descends on the lateral side of the artery receiving corresponding tributaries
• Contains no valves so blood can go up to the cavernous sinus or down to the
IJV
• At the angle of the mouth near buccinator, the anterior facial v. is connected to
the pterygoid plexus (which is connected to the cavernous sinus) by the deep
facial v.
• Dangerous zone: between the angular & the deep facial veins where facial
venous blood can easily drains to the cavernous sinus transmitting infections
resulting in sinus thrombosis
• In the submandibular triangle the vein lies superficial to the gland just deep to
the roof of the triangle & receives veins from the gland
• It meets the anterior division of retromandibular v. forming the common facial
v. which drains to the IJV
2- Transverse facial vein.
3- Infraorbital vein.
4- Mental vein.
5- Buccal vein.
Nerves of the face:
MOTOR:
Facial nerve:
- After leaving the stylomastoid foramen it gives muscular branches to
occipitalis & to the posterior belly of digastric &stylohyoid
- In its way to the face this nerve enters the posterior surface of the parotid gland
medially then passes very superficial in the gland dividing into:
- Temporofacial branch; the upper division which gives the temporal &
zygomatic branches.
- Cervicofacial branch; the lower one which gives the buccal, mandibular &
cervical branches
- Temporal br supplies muscles above the palpebral fissure
- Zygomatic br supplies muscles between the palpebral & oral fissures
- Buccal br is for buccinator
- Marginal mandibular br. supplies muscles of the lower lip
- Cervical br. is for platysma
!
42
Head & Neck Dr. Nawfal K. Al-Hadithi
SENSORY:
1 ) Trigeminal nerve:
Terminal branches of the three divisions of trigeminal nerve supply the face as
follows:
I: Ophthalmic division:
Supraorbital n.: forehead up to the vertex
Supratrochlear n.: middle part of forehead up to hairline
Infratrochlear n.: medial ½ of the upper lid & bridge of the nose
Lacrimal n.: lateral ½ of the upper lid
External nasal n.: middle of external nose down to the tip
!
43
Head & Neck Dr. Nawfal K. Al-Hadithi
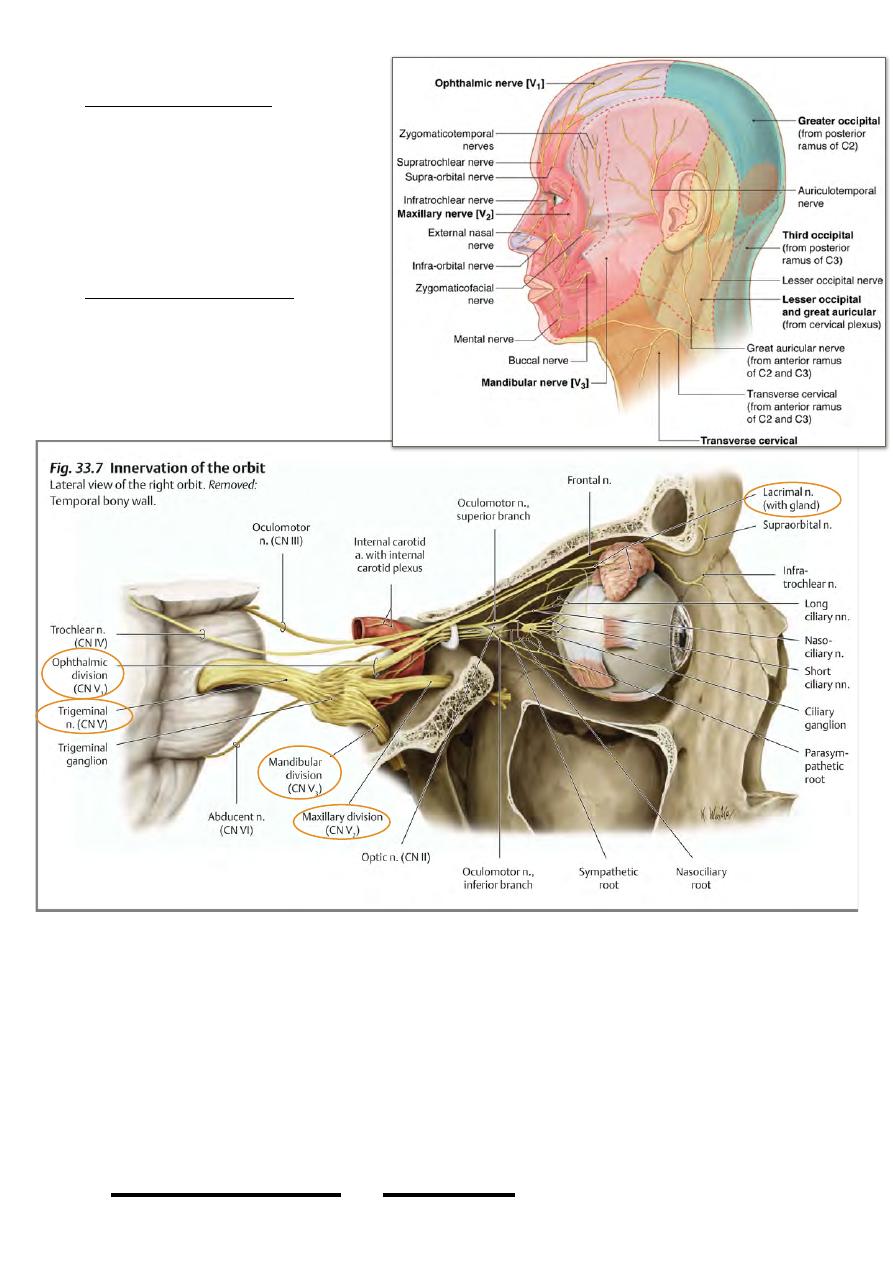
II: Maxillary division:
Zygomaticofacial n.: prominence
of the cheek
Infraorbital n.:
Palpebral br.: lower lid
Nasal br.: lateral side of the
external nose
Labial br.: upper lip
III: Mandibular division:
Buccal n.: skin over buccinator
Mental n.: chin & lower lip
2 ) Great auricular nerve:
Supplies skin over the angle of
the mandible.
Applied anatomy of the face:
1- Cavernous sinus thrombosis could follow face infections especially with force
manipulations, with the resultant ophthalmoplegia & high mortality rate.
2- Three branches of facial nerve could be easily injured in the face, the temporal &
zygomatic as they pass over the z. arch could be injured in fractures of the arch
producing dry eye & partial ptosis, the 3rd is the marginal nerve at the lower border
of the mandible could be injured in abscess drainage producing drop lip.
3- Complete facial palsy is of two types:
a. Upper motor neuron; especially evident in the upper muscles
!
44
Head & Neck Dr. Nawfal K. Al-Hadithi
b. Lower motor neuron; clear paralysis seen affecting all ipsilateral facial muscles
with its characteristic appearance.
The temporal fossa:
- Lies at the side of the head, being bounded by the
temporal lines above, anteriorly & posteriorly and by the
infratemporal crest of the sphenoid below.
- The floor of the fossa is formed by frontal, parietal,
squamous temporal bones & greater wing of sphenoid.
Temporal fascia:
A strong membrane that arises from the area between the
superior & inferior temporal lines and descends down covering
temporalis muscle to be attaches to the upper border of the
zygomatic arch & posterior border of the zygomatic bone.
Temporalis:
Origin; floor of the temporal fossa & temporal fascia.
Insertion; Fibers of this fan-shape muscle converge from this
wide origin into a tringular tendon which slides in the gutter
between the posterior root of the z. arch & the squamous
temporal bone to be inserted in the coronoid process of the
mandible
Nerve supply; anterior & posterior deep temporal branches from the
anterior division of Vc.
!
45
Head & Neck Dr. Nawfal K. Al-Hadithi