Anatomy
Dr.Nawfal
Temporal fossa & Salivary Gland
b. Lower motor neuron; clear paralysis seen affecting all ipsilateral facial muscles
with its characteristic appearance.
The temporal fossa:
-
Lies at the side of the head, being bounded by the
temporal lines above, anteriorly & posteriorly and by the
infratemporal crest of the sphenoid below.
-
The floor of the fossa is formed by frontal, parietal,
squamous temporal bones & greater wing of sphenoid.
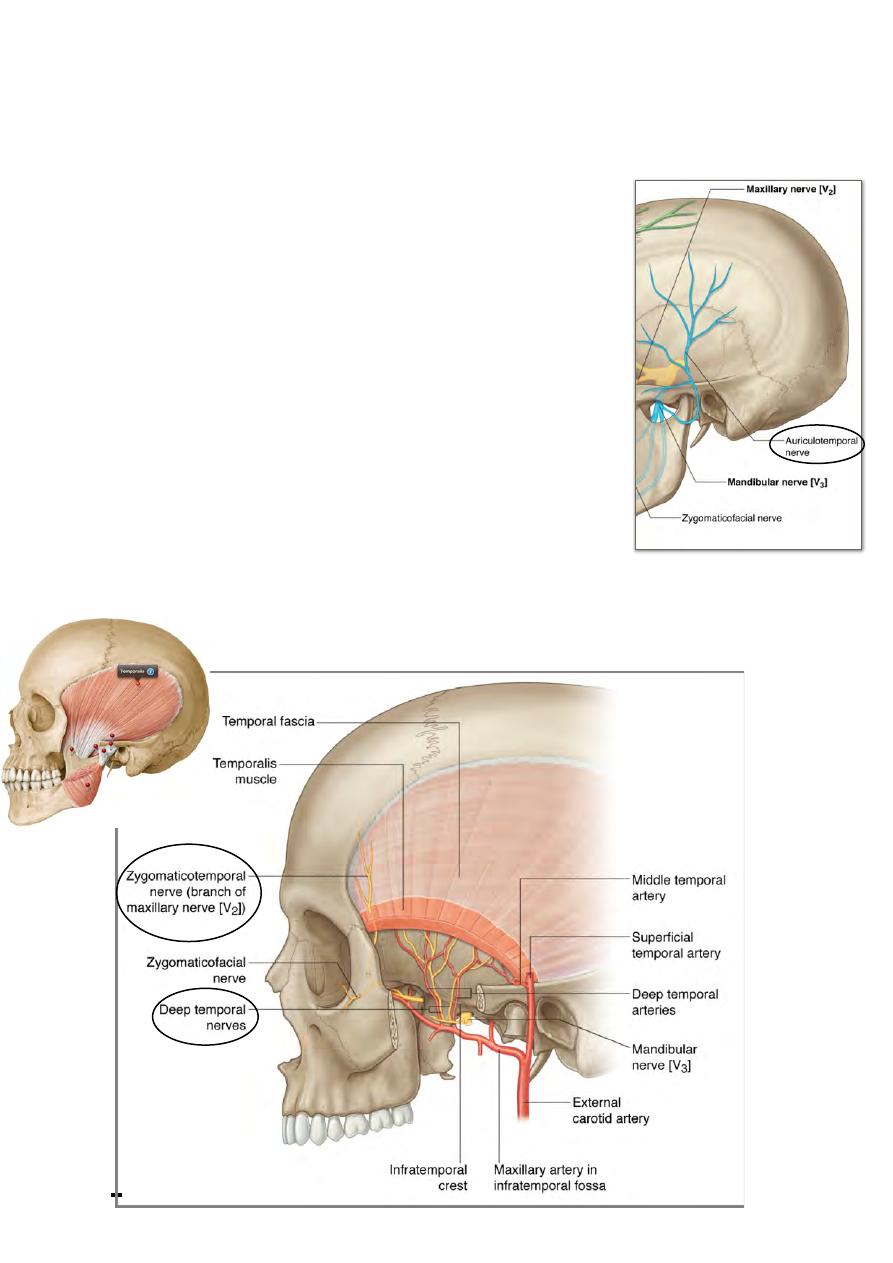
Temporal fascia:
A strong membrane that arises from the area between the
superior & inferior temporal lines and descends down covering
temporalis muscle to be attaches to the upper border of the
zygomatic arch & posterior border of the zygomatic bone.
Temporalis:
Origin; floor of the temporal fossa & temporal fascia.
Insertion; Fibers of this fan-shape muscle converge from this
wide origin into a tringular tendon which slides in the gutter
between the posterior root of the z. arch & the squamous
temporal bone to be inserted in the coronoid process of the
mandible
Nerve supply; anterior & posterior deep temporal branches from the
anterior division of Vc.
!
45
Head & Neck Dr. Nawfal K. Al-Hadithi
Action;
-
Anterior fibers (vertical): close the mouth
-
Posterior fibers (horizontal): retract the mandible
Vessels of the fossa:
Superficial temporal vessels, discussed.
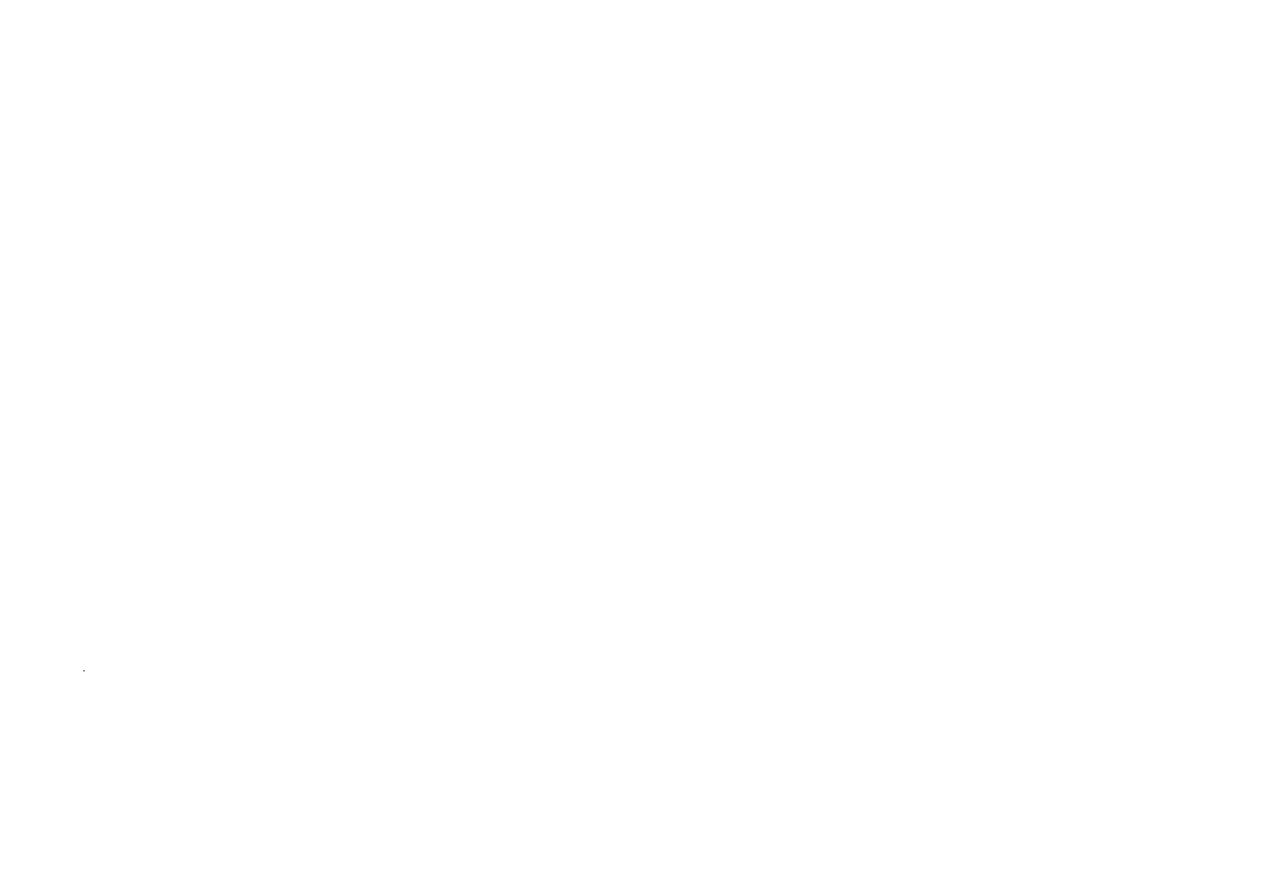
Sensory nerves of the fossa:
1- Zygomaticotemporal n. (branch of Vb): non-hairy part
2- Auriculotemporal n. (branch of Vc): hairy part
The fossa communicates inferiorly through the infratemporal crest with the
infratemporal fossa.
The preauricular region:
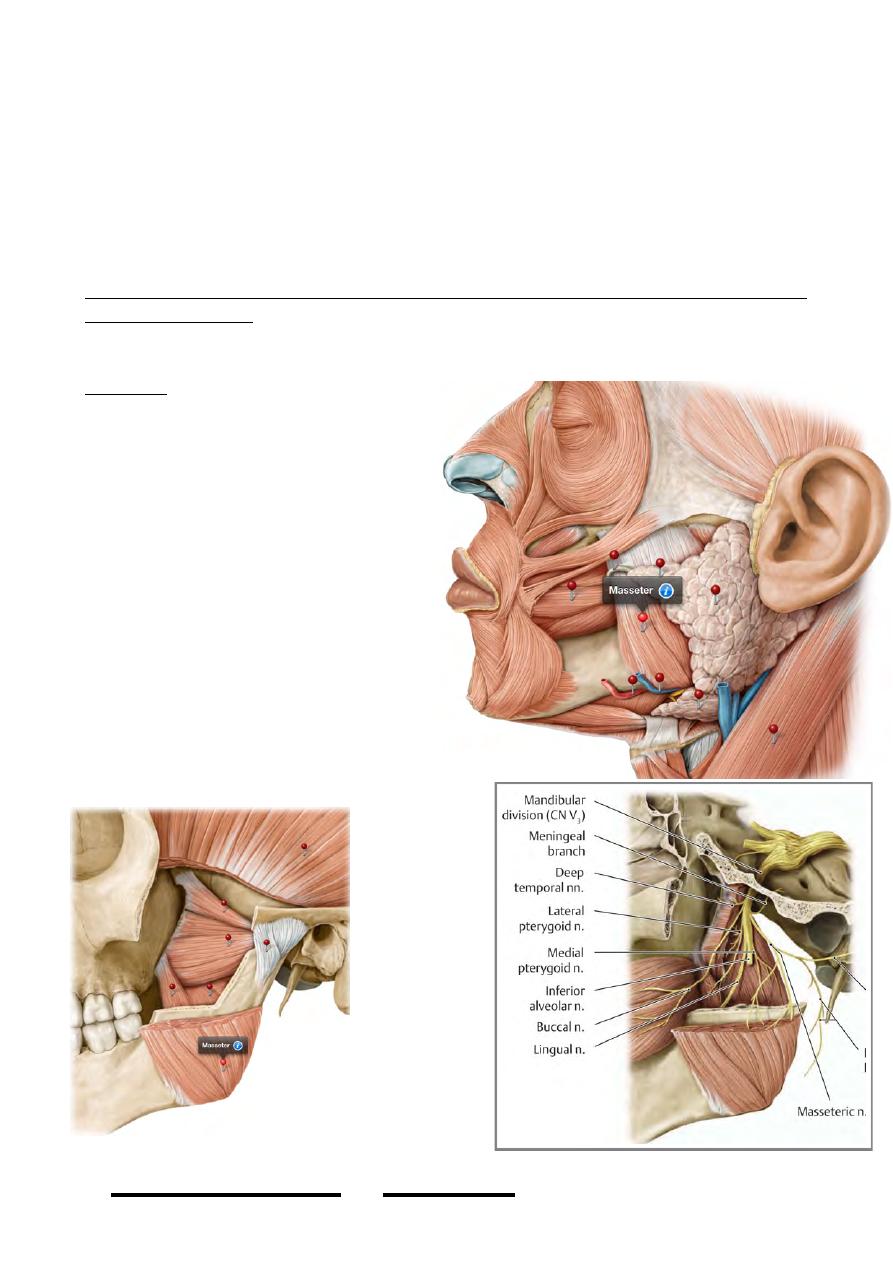
Masseter:
-
A thick quadrangular muscle that
lies on the lateral side of the
angle of the mandible partly
covered by the anterior portion of
the parotid gland & crossed by its
duct
-
It is one of the 4 muscles of
mastication
Origin:
-
The superficial part: anterior 2/3
of the zygomatic arch
-
The deep part: posterior 1/3 &
medial surface of the arch
Insertion: On the lateral aspect of the
angle of the mandible
Nerve supply: Masseteric nerve, a
branch
of anterior
division of
V c e n t e r s
t h e d e e p
s u r f a c e o f
the muscle
after passing
through the
mandibular
notch from
the ITF
A c t i o n :
Closes the
mouth.
!
46
Head & Neck Dr. Nawfal K. Al-Hadithi
The salivary glands:
-This is a group of glands that function as an initial digestion apparatus.
-They lubricate the mouth & partially digest some sorts of food.
-The main glands are three, parotid, submandibular & sublingual, though the mucous
membranes of the oral cavity contains a lot of minute glands.
-Their secretion is a mixture of mucous & serous fluid called the saliva.
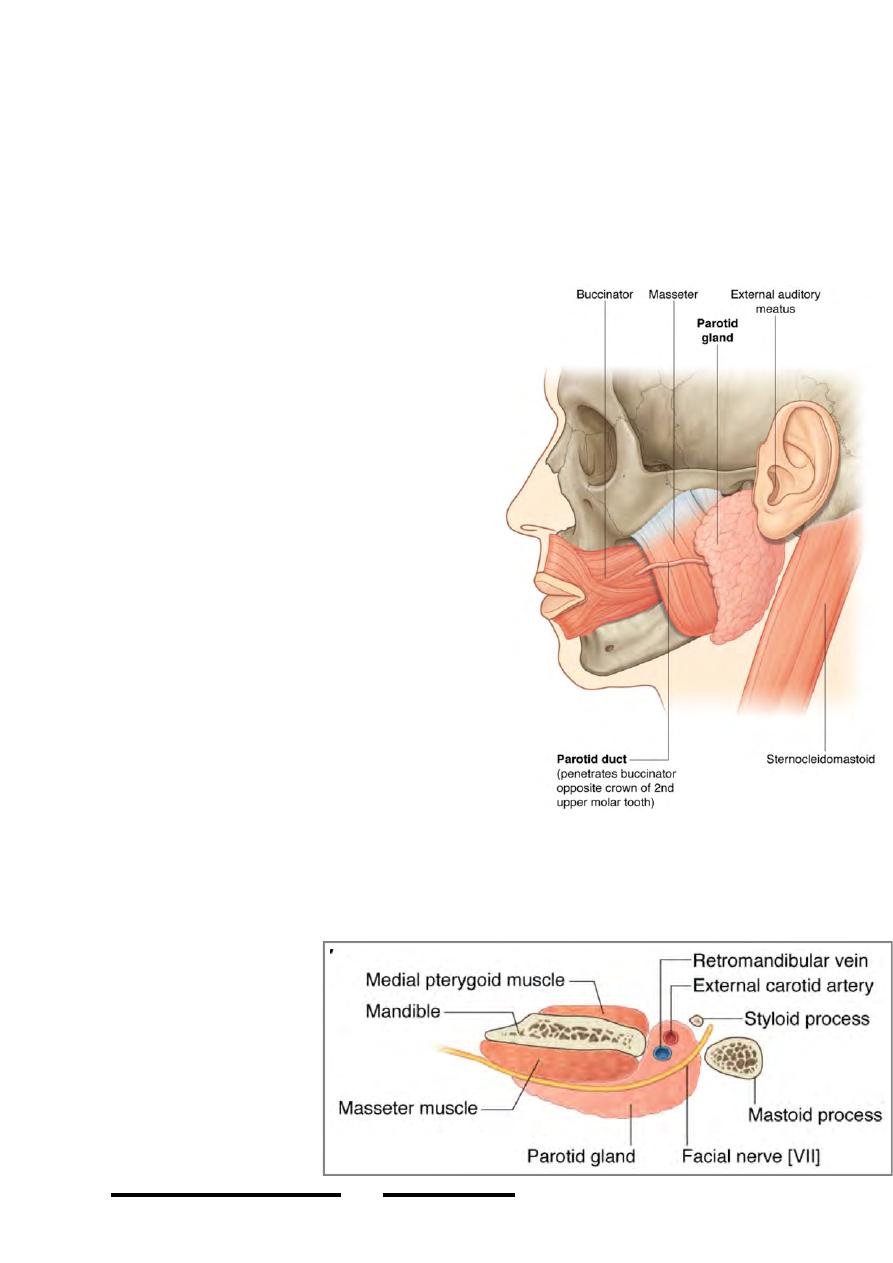
The parotid gland:
Is the largest of the salivary glands, almost
totally serous in secretion.
Shape:
The gland is a pyramid with an irregular
triangular base directed laterally
Position:
*The pyramid is wedged in the slit between the
external auditory meatus posteriorly & the
mandible anteriorly.
*The base of the pyramid lies laterally in the
preauricular region, & the three borders are:
-
Superior: along the zygomatic arch
-
Posterior: anterior to the EOM &
mastoid process
-
Anterior: actually it is antero-inferior
overlies the posterior part of masseter.
*The apex of the pyramid lies deep in the slit
reaching the carotid sheath.
Relations:
* Superiorly: The zygomatic arch & the skull
base above
* Posteriorly:
-
Mastoid process sandwiched by the sternomastoid muscle & the posterior belly
of digastric
-
The EOM, styloid process & stylohyoid are also posterior relations.
* Antero-inferiorly: The
angle of the mandible
s a n d w i c h e d b e t w e e n
m a s s e t e r & m e d i a l
pterygoid muscles
* Laterally: The fatty
tissue of the side of the
face
* Medially: The carotid
s h e a t h & l a t e r a l
pharyngeal space
!
47
Head & Neck Dr. Nawfal K. Al-Hadithi
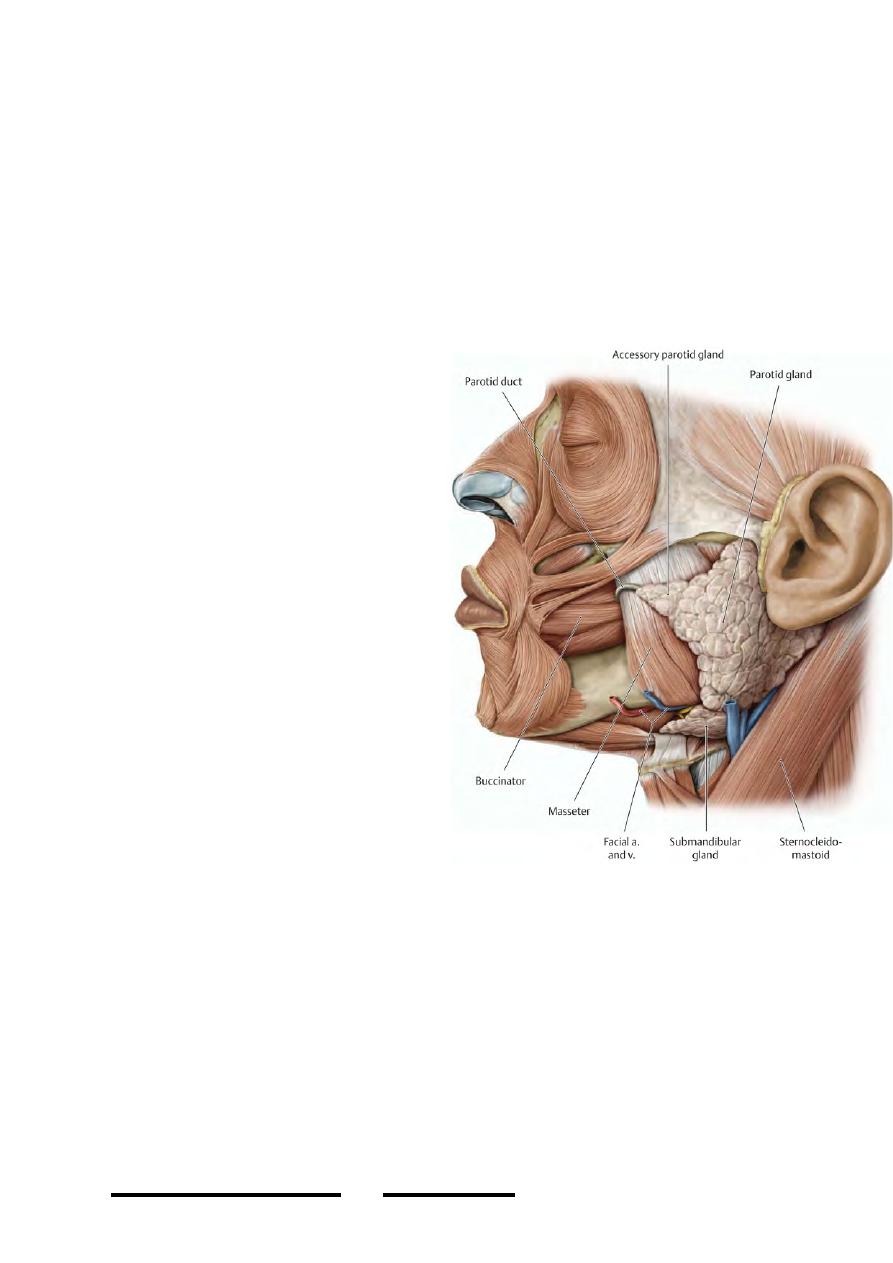
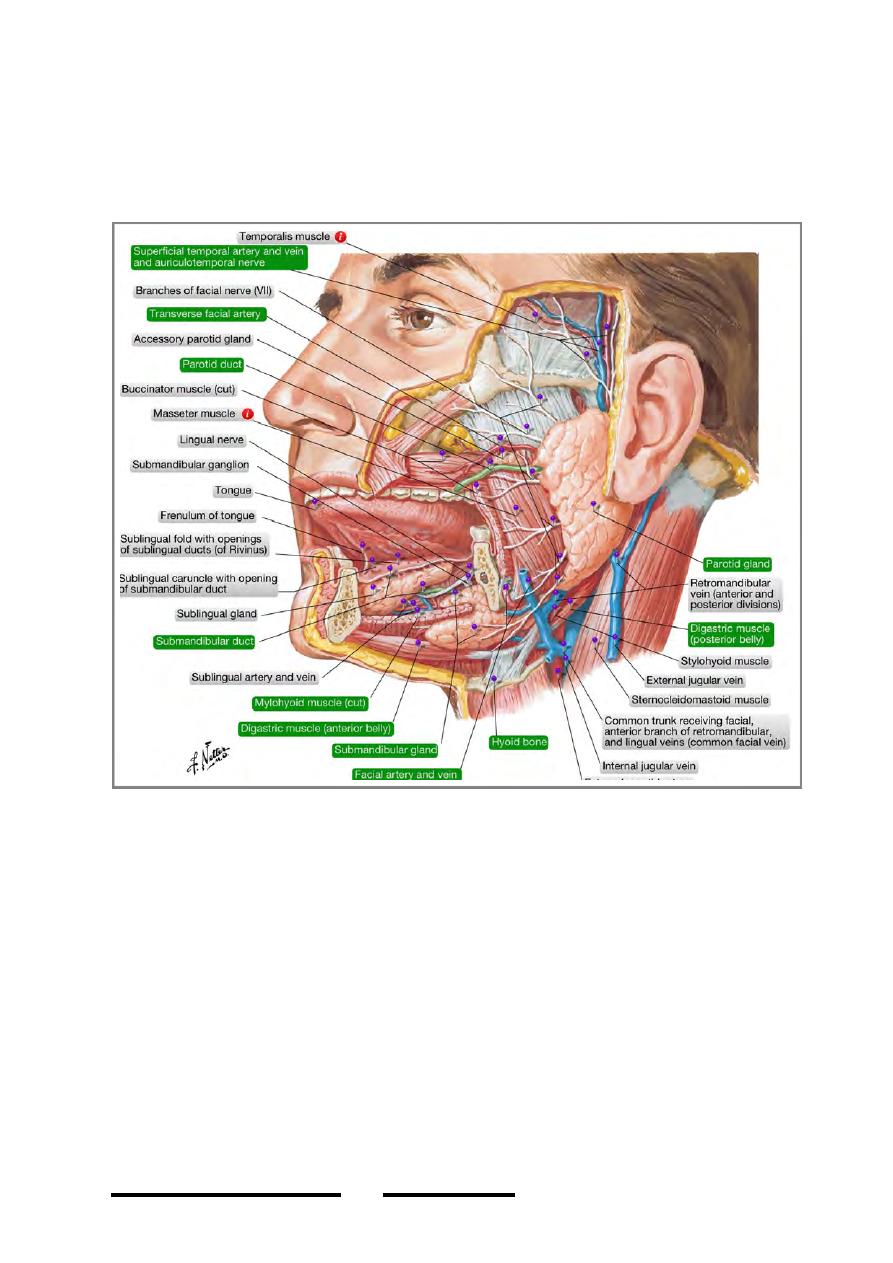
The parotid duct:
-
The duct leaves the anterior border of the gland 1 cm below the zygomatic
arch.
-
It courses over masseter in a horizontal line that could be marked on the
surface as the middle 1/3 of a line passing from the intertragic notch to the
point midway between the red margin of the lip & the lower border of the nose.
-
At the anterior border of masseter, the duct dips medially piercing the buccal
pad of fat & buccinator opposite to the last molar tooth.
-
After a short course in buccinator (which acts as a valve), the duct opens in the
vestibule of the mouth opposite to the upper second molar tooth.
The parotid isthmus:
-
Is the thinnest portion of the gland
that lies between the mandible &
the mastoid process
-
The part of the gland superficial to
the isthmus is called (wrongly!)
the superficial lobe & the part
deep to it called the deep lobe.
-
Actually, VII is the structure
which separates the gland into its
two lobes
The accessory parotid gland:
From the duct over masseter sometimes
a piece of parotid tissue lies & may
extend high up to the temporal fossa.
This is the accessory parotid g. or
sometimes named (glenoid lobe).
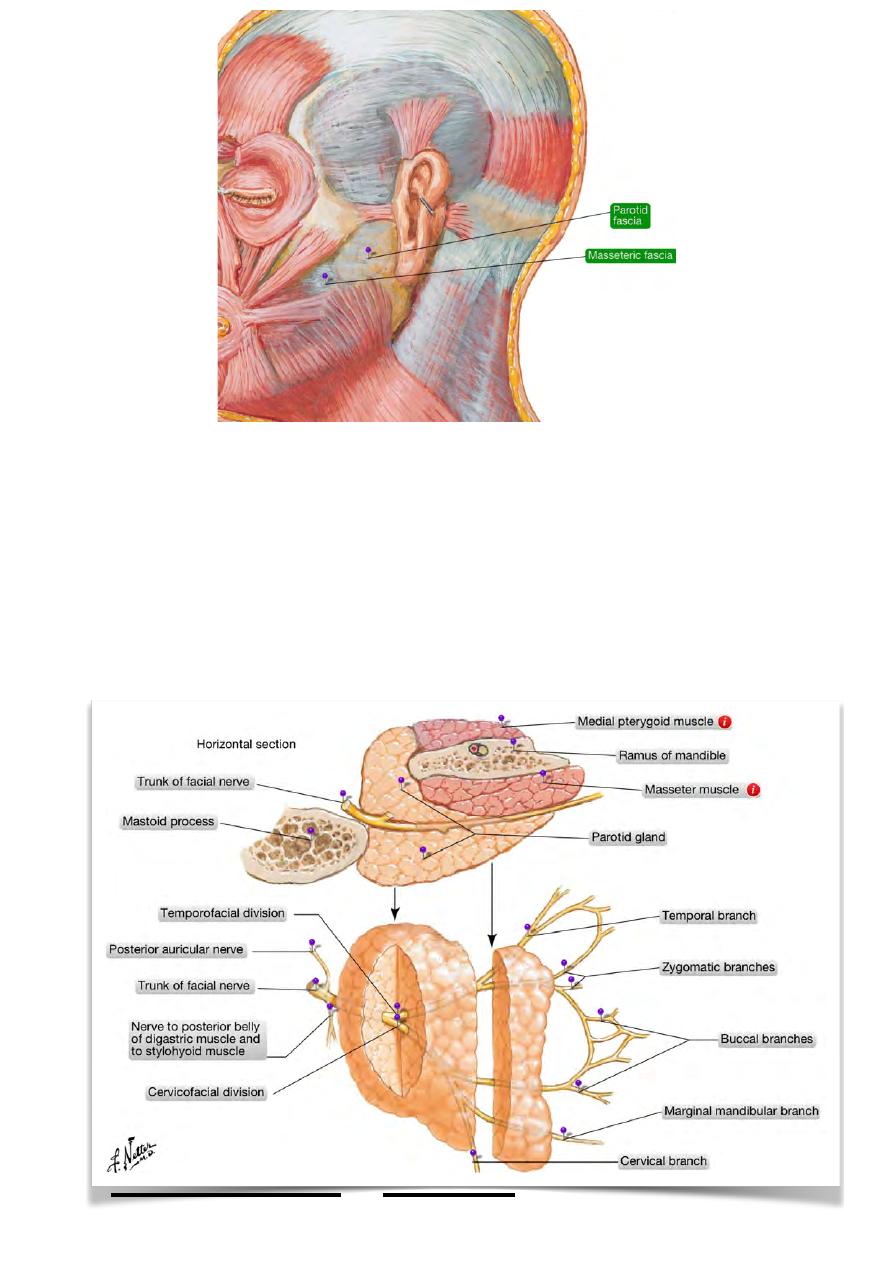
The parotid fascia:
Is derived from the investing cervical
fascia which splits to enclose the gland.
The superficial layer of the fascia will be
attached above to the zygomatic arch &
after it crosses the gland it fuses with
masseteric fascia.
The deep layer is attached above to the lower border of the tympanic plate & reaches
medially the carotid sheath with which it fuses.
A thickening in the deep layer stretches between the styloid process & the angle of
the mandible called the stylomandibular ligament which separates the gland from the
submandibular gland.
The fascia is supplied by the great auricular nerve.
!
48
Head & Neck Dr. Nawfal K. Al-Hadithi
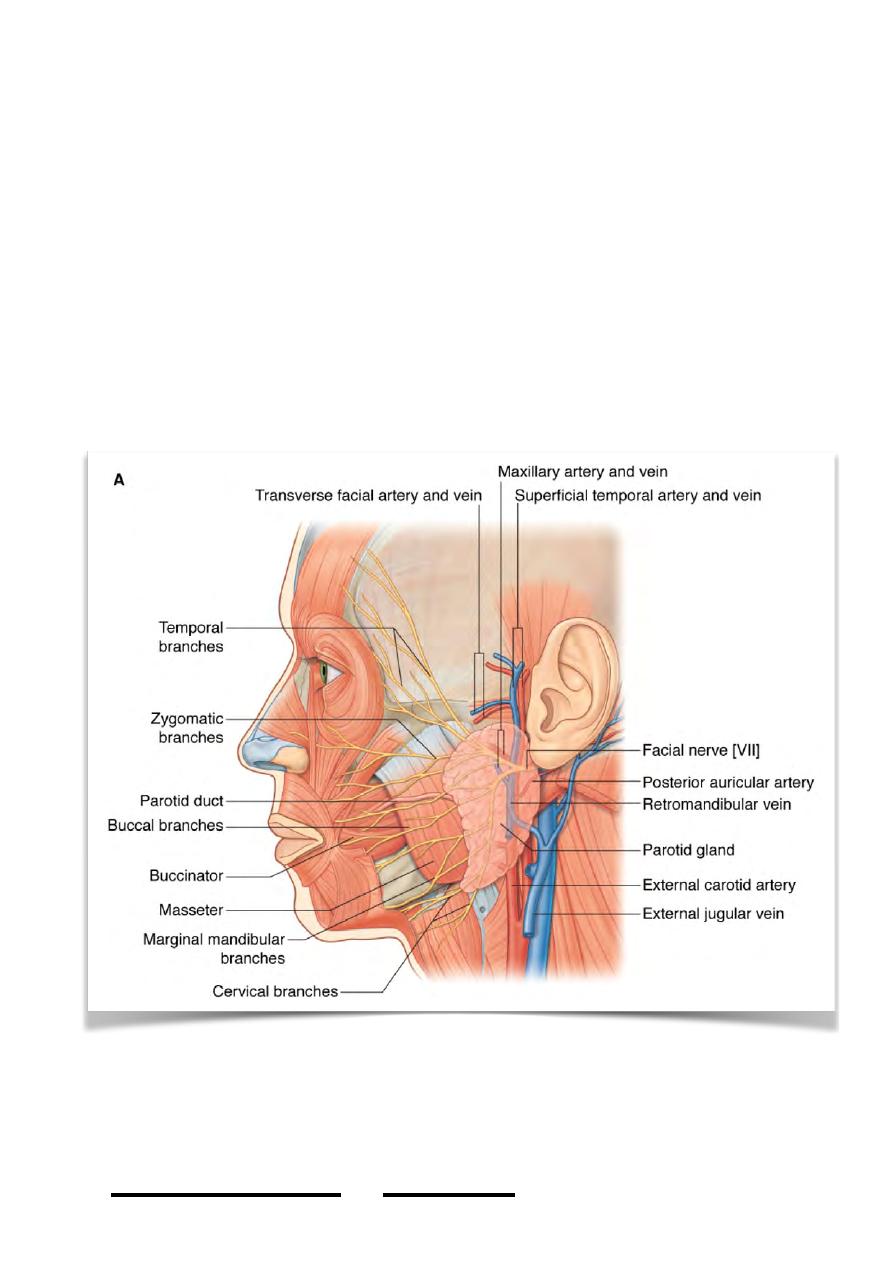
Contents of the gland:
Many important structures lie within or very near to the parotid gland, structures
which lie within the substance of the gland are; from superficial to deep:
1-The facial nerve:
-
After leaving the stylomastoid foramen in its way to the face this nerve enters
the posterior surface of the gland medially then passes very superficial in its
substance where it gives its terminal branches from the anterior border of the
gland to the face.
-
The facial branches are almost horizontal at their beginning and could be
injured in parotid incisions.
!
49
Head & Neck Dr. Nawfal K. Al-Hadithi
2-The retromandibular vein:
-
The two maxillary veins leave the ITF & go forward medial to the neck of the
mandible to enter the parotid deep to the facial nerve
-
After receiving the superficial temporal vein, the retromandibular vein is
formed within the gland.
-
It drains the parotid & divides into:
a. Anterior division: receives the anterior facial vein to form the common facial
vein in the submandibular triangle.
b. Posterior division: receives the posterior auricular vein to form the EJV behind
the angle of the mandible.
3-The external carotid artery:
-
Enters the gland from below & ascends in it deep to the above two structures
-
When reaches the neck of the mandible the ECA divides into its two terminal
divisions which leave the gland from its anterior & superior borders.
4- The preauricular (parotid) lymph nodes:
a. Superficial nodes: between the gland & its fascia.
b. Deep nodes: embedded within the gland.
!
50
Head & Neck Dr. Nawfal K. Al-Hadithi
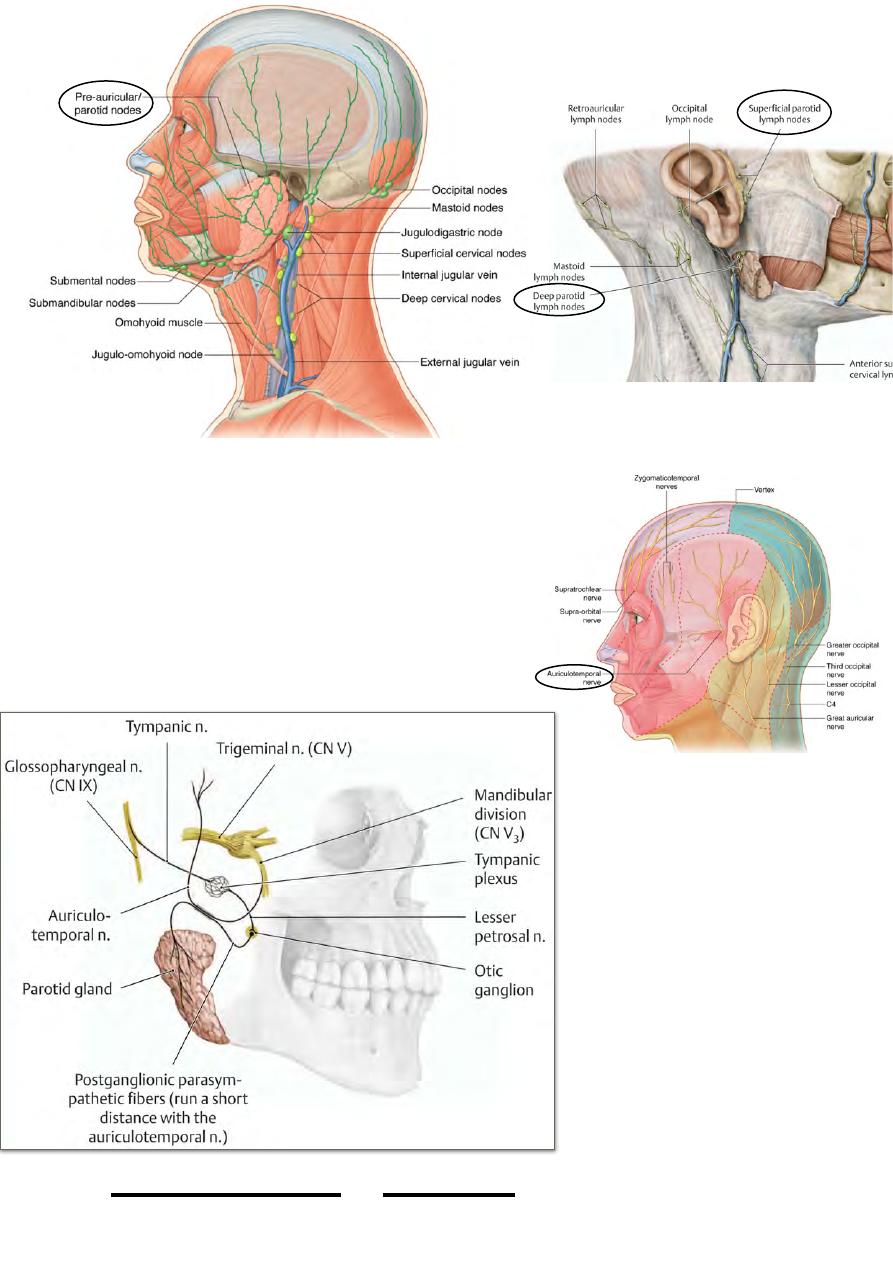
5- The auriculo-temporal nerve: figure p.44 p.29
In its way from the ITF to the temporal fossa, it
passes through the upper part of the gland to
accompany the superficial temporal artery & go to
the scalp.
Blood supply:
-
Superficial temporal a. Figure p50
-
Posterior auricular a. Figure p43
Venous drainage:
Retromandibular vein.
Lymphatic drainage:
The parotid lymph nodes.
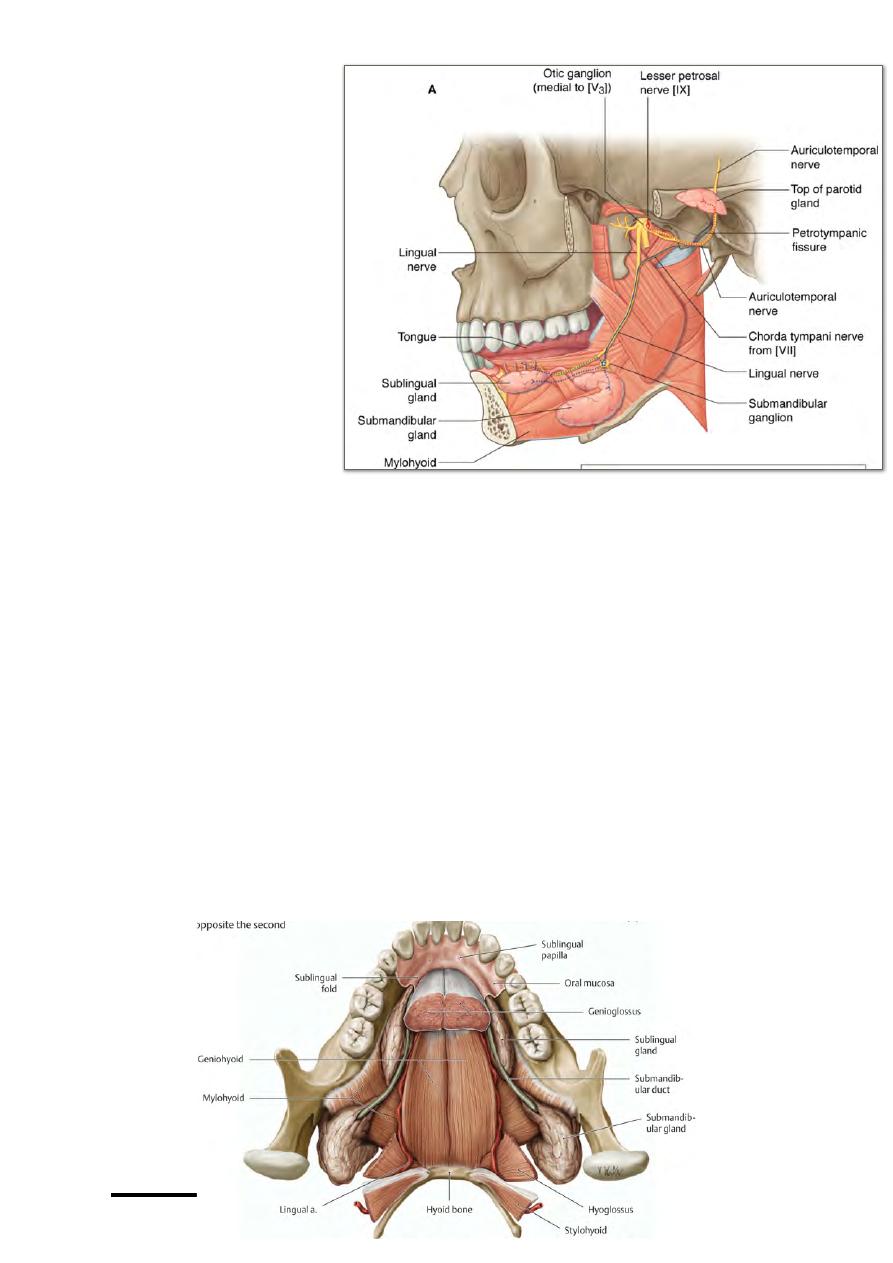
Nerve supply:
1- Sensory & secretomotor:
Lesser petrosal fibers from
the otic ganglion via the
a u r i c u l o t e m p o r a l
nerve.concept will be fully
understood in p64
2- Parotid fascia is supplied
by the great auricular
nerve.
!
51
Head & Neck Dr. Nawfal K. Al-Hadithi
Applied anatomy: p.49
•
Malignant tumors of the parotid sometimes involve the facial nerve forming
lower motor facial palsy.
•
Incisions in the substance of the gland should be horizontal along the facial
nerve branches because they are superficial to the vessels of the gland &
paralysis could occur by cutting the facial nerve before a serious bleeding is
encountered.
•
Inflammation of the parotid as in mumps usually obliterate the angle between
the lobule of the auricle & the angle of the mandible.
The submandibular gland:
Shape & position:
- This mixed gland occupies most of the submandibular triangle
- It rests on the investing fascia while the latter is stretched between the mandible &
the hyoid bone
- It leaves a smooth impression on the inside of the mandible below the mylohyoid
line
- The gland goes posteriorly to reach the angle of the mandible near the parotid gland,
here it turns up around the free posterior border of mylohyoid (which overlies it) &
the remaining part of it will lie above this muscle in the floor of the mouth
- The part of the in the neck is called “superficial lobe” while the part in the floor of
the mouth is called “deep lobe”
Relations:
- Anterolateral: mandible
- Below: investing fascia
- Above: mylohyoid
- Behind: parotid, digastric “post. belly” & stylohyoid
- Medial: digastric “ant. belly” & hyoid bone
!
52
Head & Neck Dr. Nawfal K. Al-Hadithi
Structures in close relation to the gland:
1- Facial artery: lies between the gland & mylohyoid then between it & the mandible
where it enters the face.
2- Common facial vein: is formed in the triangle superficial to the gland.
3- Submandibular lymph nodes: in and around the gland.
The submandibular fascia:
-
Like the parotid, this gland derives its fascia from the investing layer of deep
cervical fascia on which the gland rests.
-
The investing fascia encloses the gland by a superficial layer superficial to it &
a deep layer between it & myelohyoid.
-
Infection of the submandibular space causes Ludwig’s angina with increased
pressure in the space pushing the tongue out of the mouth
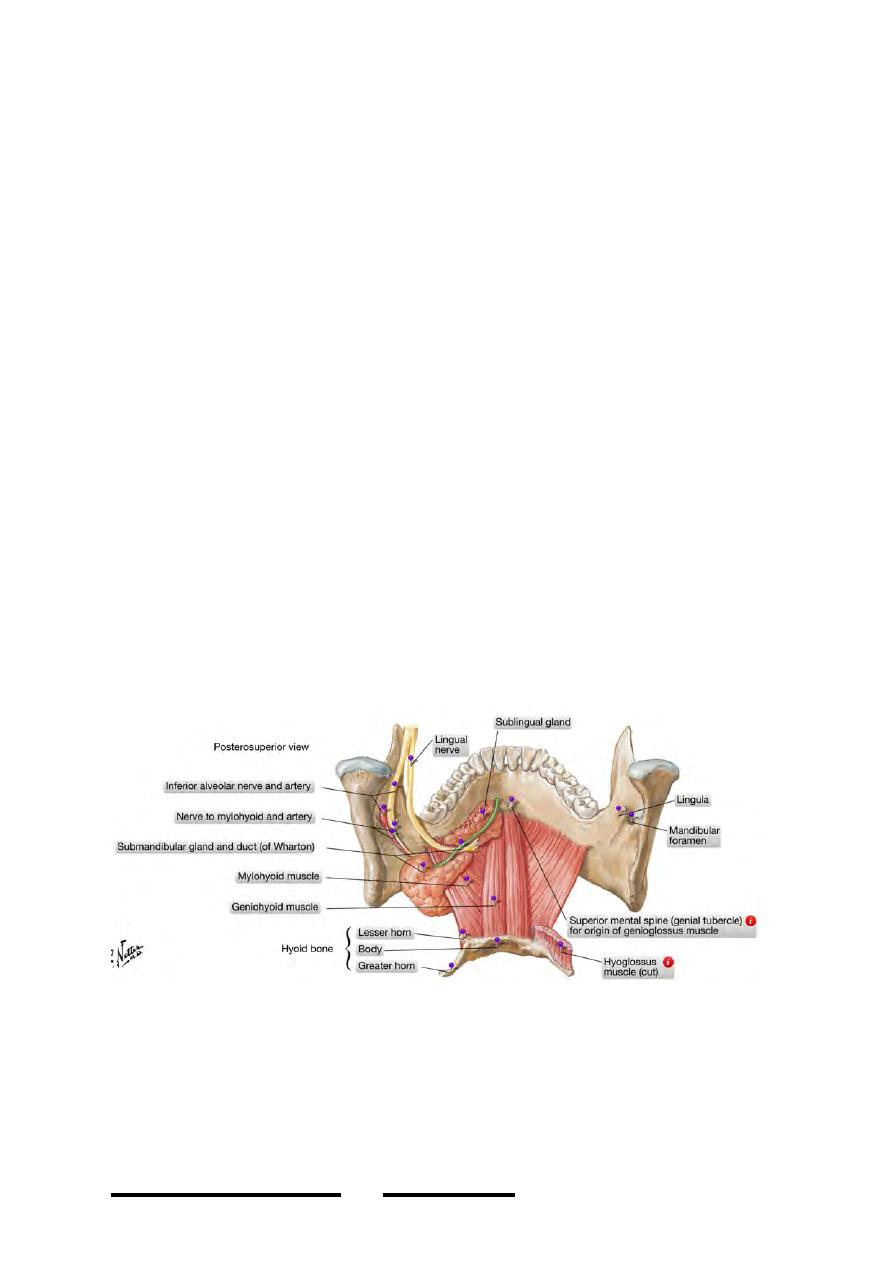
The submandibular duct:
-
A 5 cm duct leaves the anterior portion of the tongue-like deep lobe to pass in
the floor of the mouth between mylohyoid & hyoglossus.
-
On the lateral surface of hyoglossus the duct lies together with the lingual &
hypoglossal nerves being crossed by the former twice.
!
53
Head & Neck Dr. Nawfal K. Al-Hadithi
-
The duct then lies
more anteriorly on
the lateral surface of
g e n i o g l o s s u s &
extends forward to
open in the sublingual
papilla on each side
o f t h e f r e n u l u m
linguae.
Blood supply:
Facial artery.
Venous drainage:
Common facial vein.
Lymphatic drainage:
The submandibular lymph
nodes.
Nerve supply:
1- Sensory & secretomotor (parasympathetic): chorda tympani fibers from the
submandibular ganglion via the lingual nerve.
2- Submandibular fascia is supplied by the anterior cutaneous nerve of the neck.
The sublingual gland:
•
The smallest of the three main salivary glands, almost totally mucous in
secretion.
•
An almond sized gland lies in the floor of the mouth being covered only with
the mucous membrane of the floor of the mouth.
•
It is bounded medially by the two genial muscles & laterally by the mandible
on which it leaves a smaller impression than the submandibular one above the
mylohyoid line.
•
The gland opens by numerous duct onto the sublingual papilla & in the floor of
the mouth.
•
The gland has no fascia.
•
It is supplied by the sublingual branch of the lingual artery & the submental
branch of the facial artery.
!
54
Head & Neck Dr. Nawfal K. Al-Hadithi
•
Veins are similar to arteries.
•
Nerve supply is identical to the submandibular gland.
•
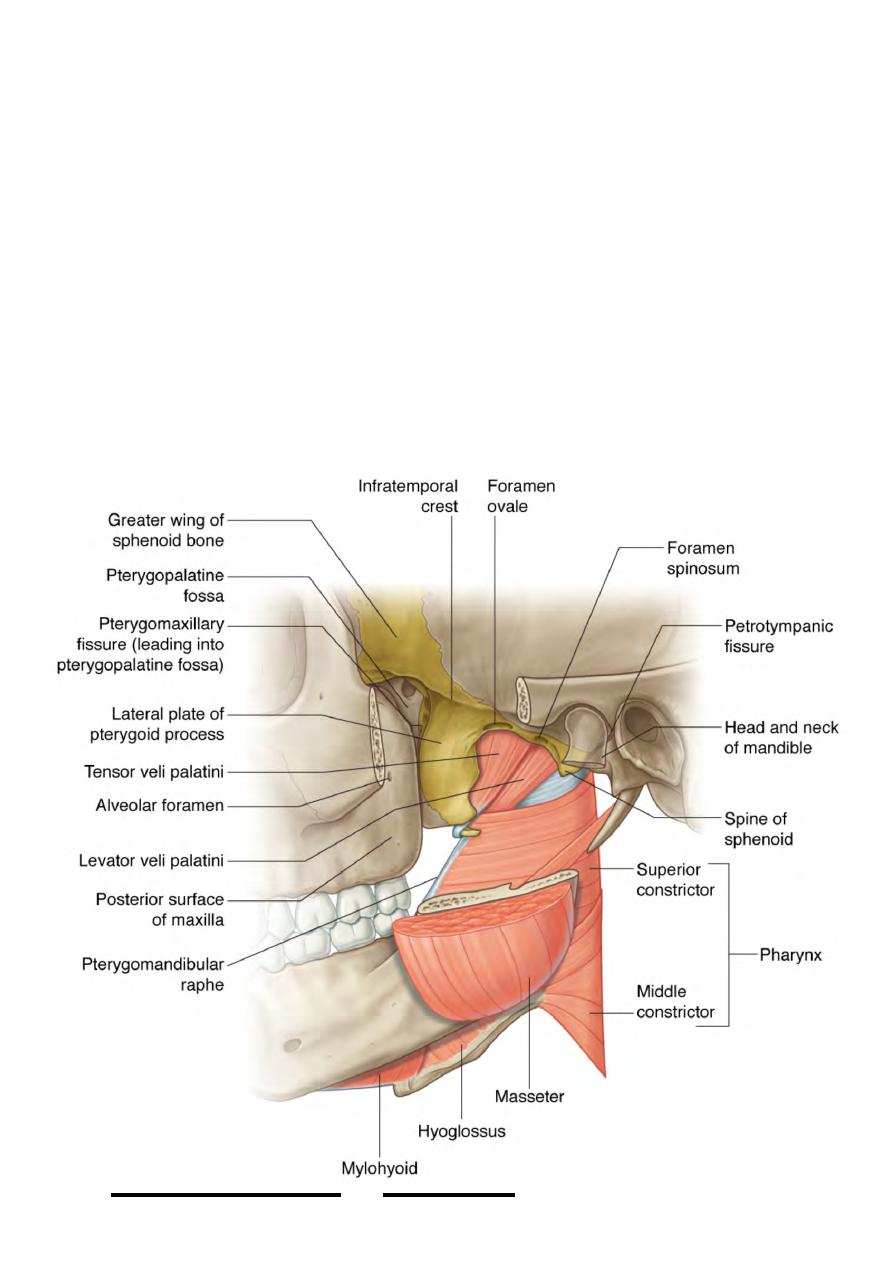
The infratemporal fossa:
•
This is the space which lies between the pharynx medially & the angle of the
mandible laterally.
•
Boundaries:
-Anteriorly: the back of maxilla & pterygoid process
-Posteriorly: the styloid apparatus laterally & the carotid sheath medially
-Laterally: the ramus & angle of the mandible
-Medially: the wall of the pharynx & medial pterygoid plate
-Superiorly: the floor of the middle cranial fossa formed by the greater wing of
sphenoid & squamous temporal, the roof ends laterally in the infratemporal crest
which leads to the temporal fossa
-Inferiorly: the ITF is continuous with the neck at the retropharyngeal space which
leads down through the superior into the posterior mediastinum.
!
55
Head & Neck Dr. Nawfal K. Al-Hadithi