
Calcium Disorders
Hypercalcaemia
&
Hypocalcaemia
Calcium balance
ECF CALCIUM
GUT
KIDNEY
BONE (1 kg)
Net 175 mg
Net 175 mg
500 mg
500 mg
1000 mg

Hypercalcemia: clinical signs
GI:
Nausea, vomiting, abdominal pain& Constipation
Acute pancreatitis and gastric ulcer
Renal:
Polyuria, dehydration, renal calcification-stones & Renal
failure
Neurological
Fatigue ,Confusion ,Stupor, coma
Increased neuromascular excitability& muscle weakness
Heart
Characteristic ECG, and in severe cases cardiac arrest

Hypercalcaemia: major causes
Primary hyperparathyroidism (PHPT), and
Tertiary hyperparathyroidism THPT
Malignancy PTHrP
Others

Hyperparathyroidism: causes
Primary PHPT
Adenoma (90%)
Carcinoma (<1%)
Familial benign hypercalcemia (FBH)
Tertiary THPT
It occurred as a result of secondary HPT;
Vitamin D
3 deficiency & chronic kidney
failure.

In
PHPT,
there
is
autonomous
inappropriate secretion of PTH from the
gland (mainly because of tumor) and this
secretion is not subjected to negative
feed back of hypercalcemia. In THPT, the
autonomous secretion of PTH is due to
sustained and prolonged stimulation of
the parathyroid gland by previous
hypocalcemia that caused by either renal
failure and/or vitamin D deficiency.

In Renal failure and vitamin D deficiency,
the hypocalcemia is not corrected even
by stimulated secretion of PTH, this
referred to secondary HPT, which
characterized by ↓ S.Ca++, normal PO4 - -
, and ↑S.PTH. The continues stimulation
of PTH gland leads to its hypertrophy
with resultant autonomous secretion of
PTH
which
unable
to
correct
hypocalcaemia because of renal damage
or deficient vitamin D.

Only after correction of underlying cause of
hypocalcemia by kidney transplantation or
vitamin D supplementation, the serum levels of
Ca
++
will be corrected and increased because
of gland hypertrophy, and this state referred to
THPT in which ↑ S.Ca
++
, ↓S.PO4
-
- -, ↑S.PTH
and the differentiating parameter between the
PHPT and THPT is the marked increased of
S.ALP in THPT, but normal in PHPT, and the
history of previous hypocalcaemia in THPT.

Malignant hypercalcemia: major
causes
PTHrP - mediated
Breast carcinoma
Squamous carcinoma (lung, head &
neck, esophagus)
Renal carcinoma
PTHrP is structurally similar to active
fragment of PTH and mimics its action
in calcium metabolism.

Hypercalcemia: other causes
Drugs:
Vitamin D
Calcium carbonate (milk alkali syndrome)
Lithium
PTH
Vitamin A
Sarcoidosis other granulomatous
disorders
Severe Hyperthyroidism

Hypercalcemia: presentations
Chronic, mild-moderate
Often asymptomatic
Cause: primary hyperparathyroidism
Issues: parathyroidectomy or not
Acute, severe
Symptomatic
Cause: malignant hypercalcemia (rarely others)
Issues: treat hypercalcemia, find & treat cause

Primary hyperparathyroidism
F:M 3:1
Usually > 50 y/o-Menopausal women
Presentation:
Asymptomatic hypercalcaemia (>50%)
Renal stones (20%)
Decreased bone density
Symptoms of hypercalcaemia (<5%)

Hypercalcemia: evaluation
Duration >6 months or renal stones:
PHPT
Signs of malignancy, other rare causes
Plasma PTH
Normal or elevated: primary
hyperpararthyroidism
Low: other causes
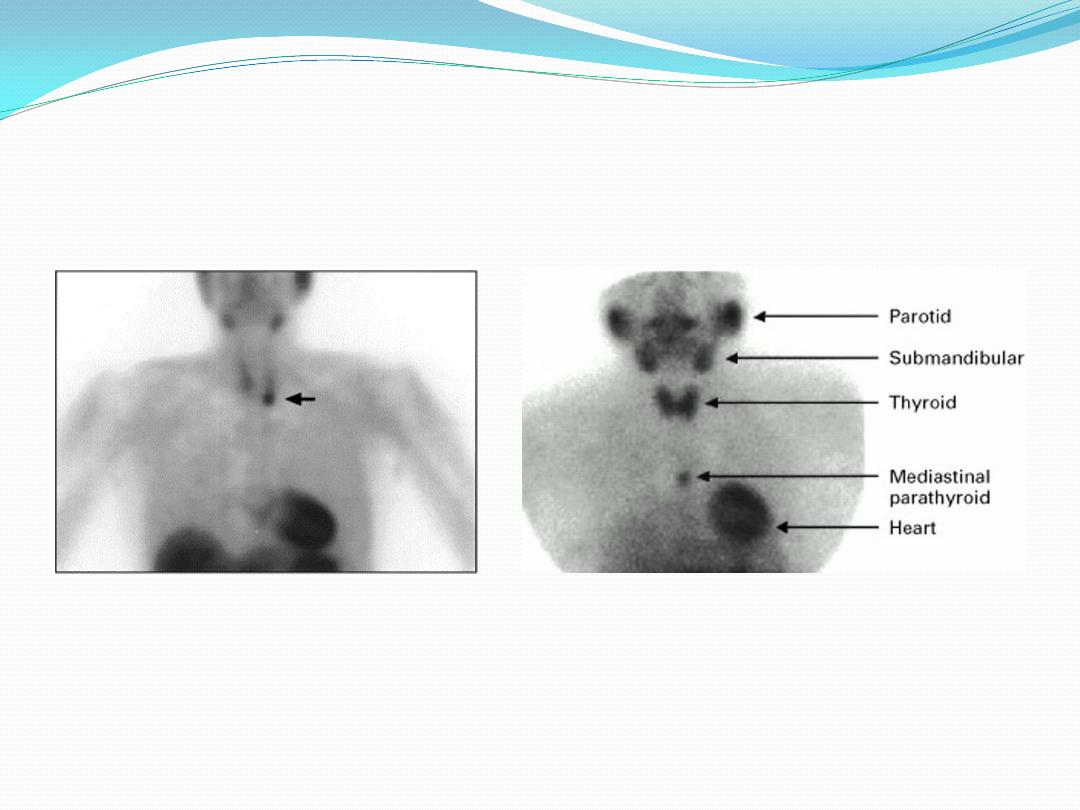
Parathyroid Localization
Sestamibi scans
Left lower parathyroid adenoma
Mediastinal parathyroid adenoma

Biochemical
evaluation:
1. In primary hyperparathyroidism:
PTH ↑, S.Ca ↑ , S.PO4 - - ↓, with
normal renal function, the S.Urea
and S.Creatinine are normal.

2. In malignancies:
a. Bony tumor; primary or metastasis
↑ S.Ca , ↑ S.PO4 - - , S.PTH ↓ and S.ALP ↑.
These are due to bone broken down by
tumor
b. humoral hypercalcaemia of
malignancy: S.Ca ↑, S.PO4 - - ↓ and S.
PTHrP(PTH related protein) is detected
and increased. This PTHrP

produced by malignant tumors of breast,
bronchus, neck, head … etc and has the
biological activity of PTH in rising the
serum levels of Ca and decreasing serum
PO4 - - levels.

Nonparathyroid hypercalcemia
Repeat history (especially drugs)
Vitamin D toxicity suspected: 25 (OH)
vitamin D
Sarcoidosis suspected: 1,25 (OH)
2
vitamin D
In vit. D toxicity :
S.Ca ↑, S.PO4 - - ↑, S.PTH ↓ and S. D3 is
↑.

Severe hypercalcemia
:
Indications for therapy
Symptoms of hypercalcemia
Plasma [Ca] >12 mg/dl

Hypocalcemia: clinical signs
Paresthesias
Tetany (carpopedal spasm)
Trousseau’s, Chvostek’s signs
Seizures
Chronic: cataracts, basal ganglia
Ca

Trousseau’s sign

Hypocalcemia: causes
Primary Hypoparathyroidism
Surgical,total or partial thyroidectomy and or
parathyoidectomy
Autoimmune
Magnesium deficiency;it is important for PTH
secretion
PTH resistance
(pseudohypoparathyroism)
Vitamin D deficiency
Vitamin D resistance
Other: renal failure, pancreatitis

Hypocalcemia: evaluation
Confirm low corrected (change in protein
bound)& ionized calcium(Free Ca
History:
Neck surgery
Other autoimmune endocrine disorders
Causes of Mg deficiency
Malabsorption
Family history

Hypocalcemia: evaluation
Physical exam:
Signs of tetany
Lab
PTH
Creatinine, Mg, P, alkaline
phosphatase
25-OH vitamin D
Hypocalcemia: evaluation
Cause
Hypoparathyroidism
PTH resistance
Vitamin D deficiency
Vitamin D resistance
Phosphate
High
High
Low
Low
Other
PTH low
PTH high
25-OHD low
Alk phos
Normal
Normal
High
High 25-OHDHigh

In renal failure: ↓ S.Ca , ↑S.P, ↑ .S. Urea
and
S.Creatinine,
with
expected
increased
of
S.PTH.
Ricket in childern and Osteomalacia in
adult (demineralized bone dis.) occur due
to deficiency of vitamin D and P. In these
bone disorder serum Ca & P are
decreased due to 1. low intake of these
element 2. low intake in vit. D 3.
malabsorption
of
vitamin
D(GIT
disortders) 4. defect in normal pathway
of vitamin D metabolism 5. hereditary
hypophosphatemia
Hypocalcemia: acute therapy
IV calcium infusion
1-2 gm Ca gluconate (10-20 ml) IV over 10 min
6 gm Ca gluconate/500 cc D5W over 6 hr
Follow plasma Ca & P Q 4-6 hr & adjust rate
IV or oral calcitriol 0.25-2 mcg/day
Oral calcium carbonate 1-2 gm BID-TID

Hypocalcemia: chronic therapy
Oral calcitriol 0.25-2 mcg/day
Calcium carbonate 1-2 gm BID-TID

Hypophosphataemia
Serum or plasma PO4- - may be
associated
with
widespread
cell
dysfunction and cell death. Muscle pain
and weakness(↑CPK), urgent phosphate
supplementation is required . Dietary
deficiency of PO4 is uncommon. ↓PO4
may occur due to; antacids, respiratory
and metabolic(Diabetic ketoacidosis DKA
& lactic acidosis). Insulin in treatment of
DKA
aggravate
hypophosphataemia
(movement to IC)

Magnesium
It is an essential IC cation. It found
mainly in skel. eton, a small proportion
in ECF. Mg deficiency rarely occurs as
an isolated phenomenon, it usually
accompanied by Ca, K, and PO4.
However, tetany, cardiac arrhythmias,
and CNS abnormalities may occur due
to Mg deficiency but not Ca.
Hypomagnesaemia
should
be
suspected in case of hypocalcaemia
and/ or hypokalaemia.↓ Mg may be due
to GIT, and renal disorders, and
reduced intake.