Process of fertilization
Prof. Dr. Malak A. Al-yawer
Objectives:
At the end of this lecture, the medical student will
be able to
Name the mechanisms and barriers involved in
sperm transport along the female genital tract
State the events occurring in the spermatozoa
immediately prior to fertilization
State the events occurring in the oocyte
immediately after sperm penetration
Outline the procedures involved in in-vitro
fertilization
Name other types of assisted conception
Fertilization
Includes those mechanisms where
by:
A sperm approaches to
Becomes attached to and
then penetrates the surface
of an ovum
The early series of changes
which follow
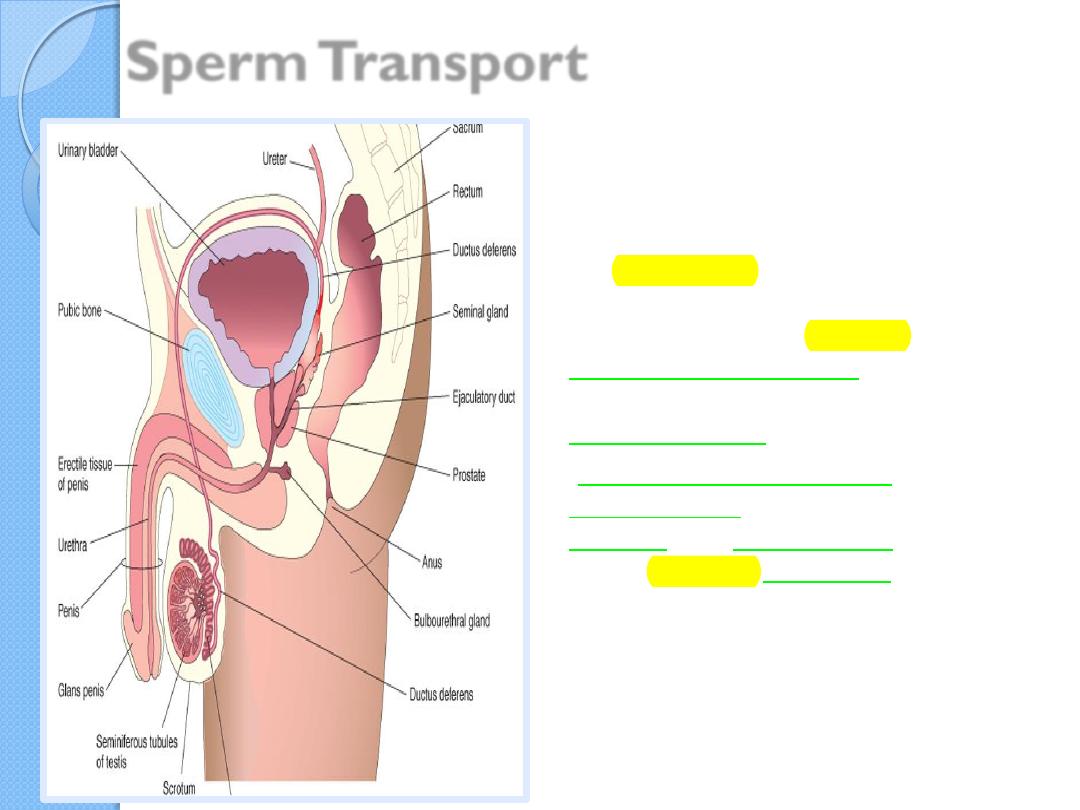
Sperm Transport
•
From their storage site in
the epididymis( mainly in its
tail) the sperms are rapidly
transported to the urethra by
peristaltic contractions of the
thick muscular coat of the
ductus deferens.
•The accessory sex glands-
seminal glands (vesicles),
prostate, and bulbourethral
glands-produce secretions that
are added to the sperm-
containing fluid in the ductus
deferens and urethra
The ejaculate
It’s volume averages
3.5
mL
( a range of 2 to 6
mL). with approximately
100 million sperm per
milliliter.
The sperms move
2 to 3
mm per minute
, but the
speed varies with the pH
of the environment.
They are
nonmotile
during storage
in the
epididymis, but become
motile in the ejaculate.
They
move slowly in
the acid environment
of the vagina,
but
move more rapidly
in the alkaline
environment of the
uterus.
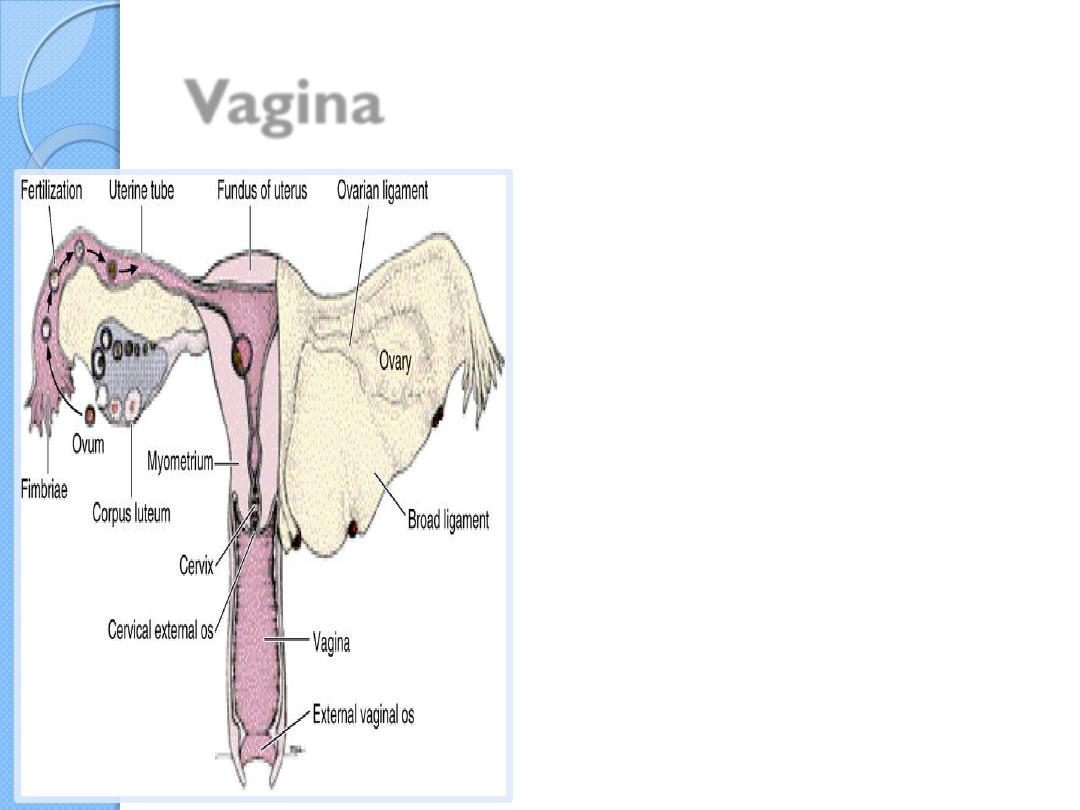
Vagina
200 to 600 million
sperms are deposited
around the external
os of the uterus and
in the fornix of the
vagina during sexual
intercourse
Cervix
Only
1%
of sperm
deposited in the vagina
enter the cervix, where
they may survive for
many hours
.
consistency and
viscosity of cervical
mucus , under hormonal
control , play an
important role in the
process of fertilization.
Prior to ovulation –
watery cervical mucus
luteal phase – viscous
and disorganized
cervical mucus
Passage of sperms through the
uterus
and uterine tubes by
muscular contractions of the uterus
and uterine tube
. Prostaglandins in the
semen are thought to stimulate uterine
motility at the time of intercourse and assist
in the movement of sperms to the site of
fertilization in the ampulla of the tube.
their own propulsion
. Fructose, secreted
by the seminal glands, is an energy source
for the sperms in the semen .
The trip from cervix to oviduct requires a
minimum of 2 to 7 hours
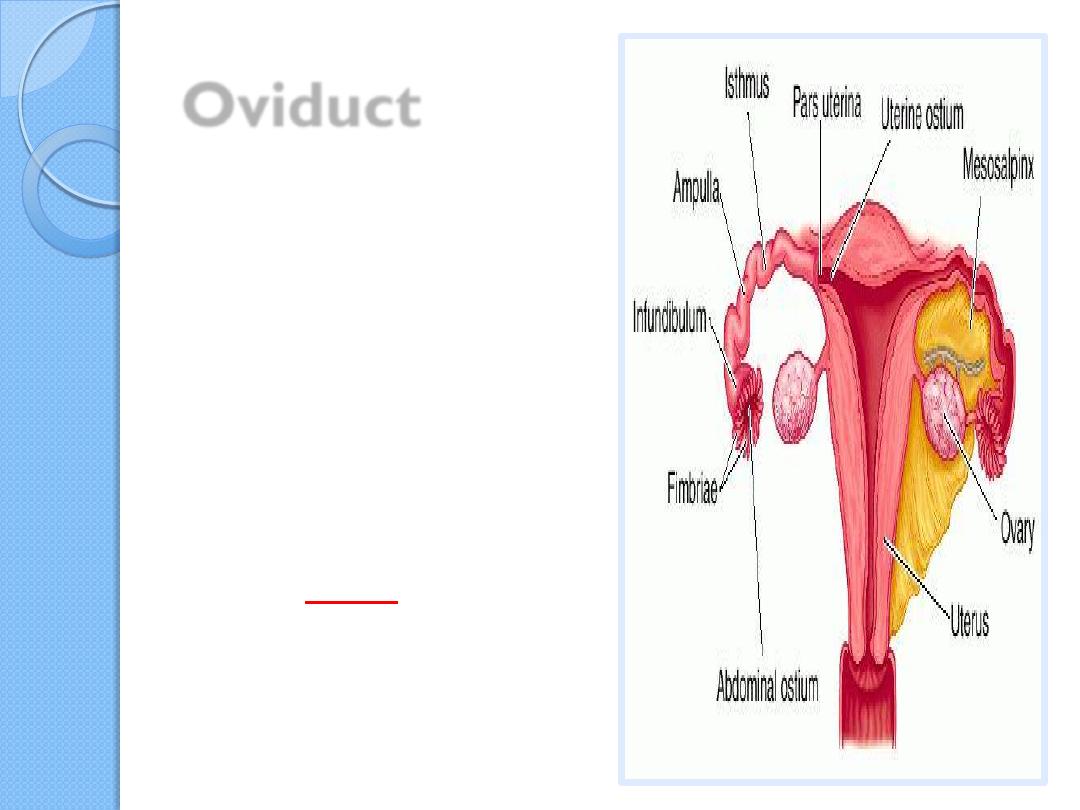
Oviduct
Uterotubal
junction
a
significant barrier
after reaching the
isthmus
, sperm
become less motile
and cease their
migration
Spermatozoa are not able to fertilize the
oocyte immediately upon arrival in the
female genital tract
They must undergo
(1) capacitation and
(2) acrosome reaction to acquire this
capability
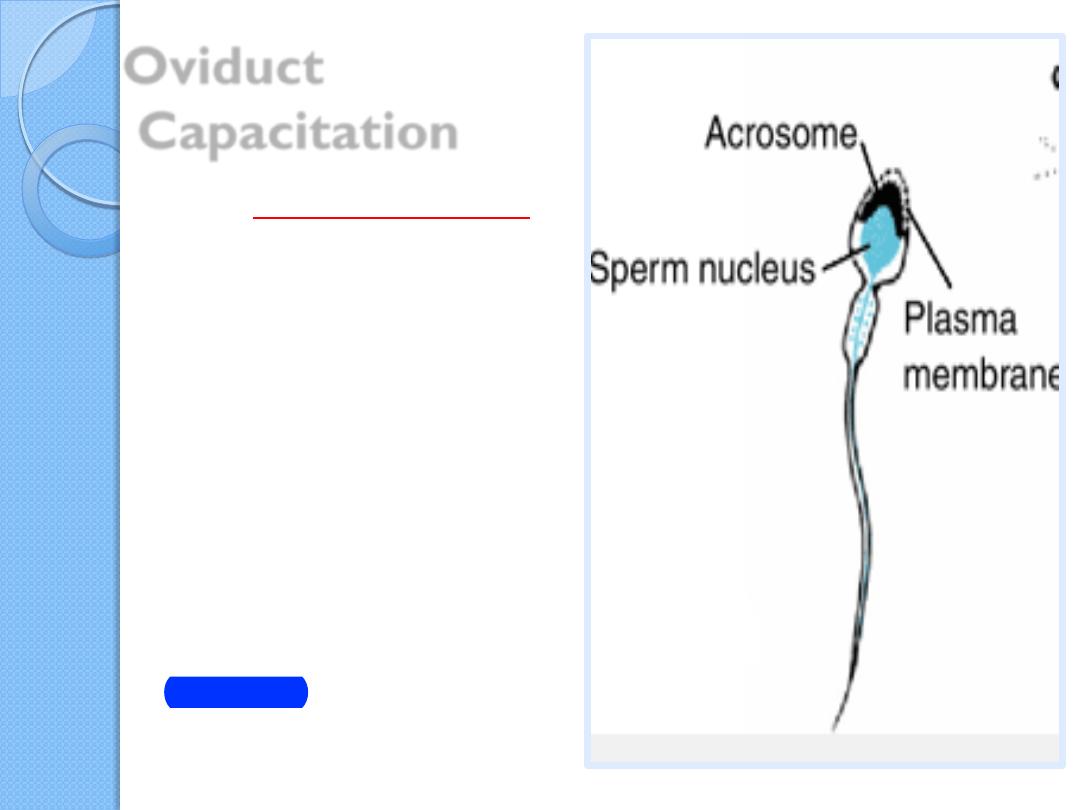
Oviduct
Capacitation
It is a period of conditioning in
the female reproductive tract ,
associated with
1.removal of
glycoprotein coat and
seminal plasma proteins
from
the plasma membrane that
overlies the acrosomal region
of the spermatozoa.
2. reorganization of plasma
membrane lipids and proteins
to prepare the sperm for
acrosome reaction .
Much of this conditioning
occurs in the uterine tube
In the human, it lasts
approximately 7 hours .
Sperm can be capacitated by
incubation in certain
fertilization media.
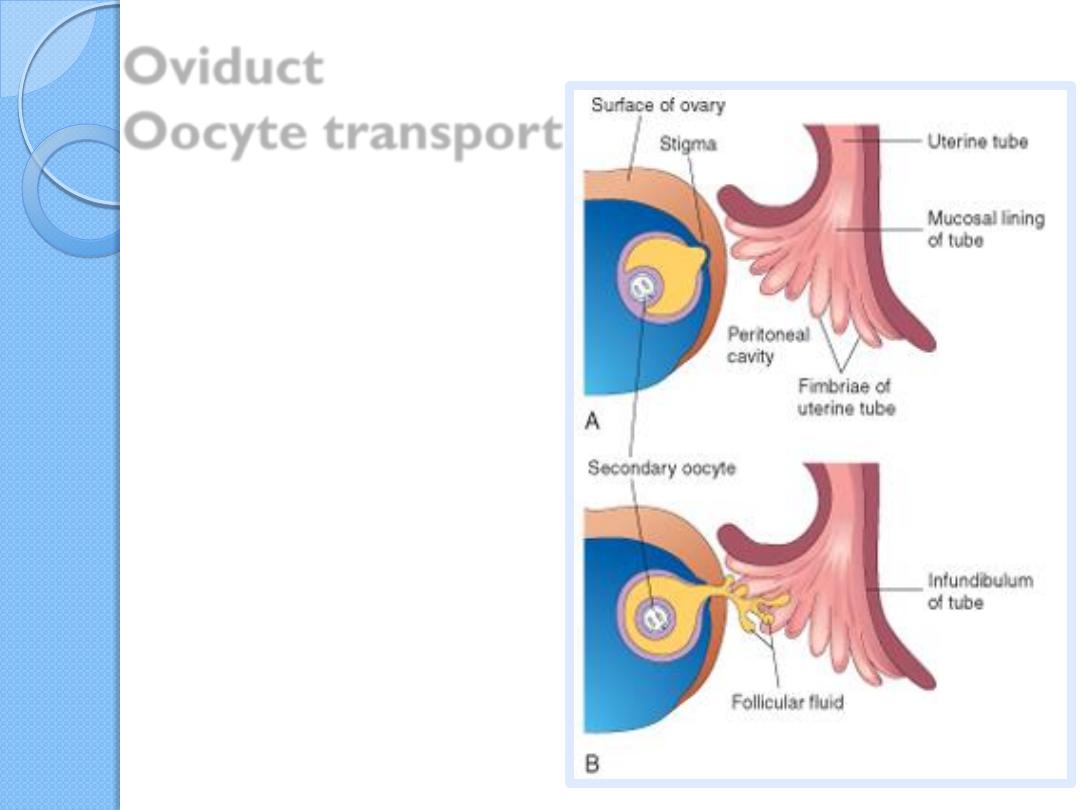
Oviduct
Oocyte transport
During ovulation, the
fimbriated end of the
uterine tube becomes
closely applied to the
ovary.
The fingerlike
processes of the tube,
fimbriae, move back and
forth over the ovary
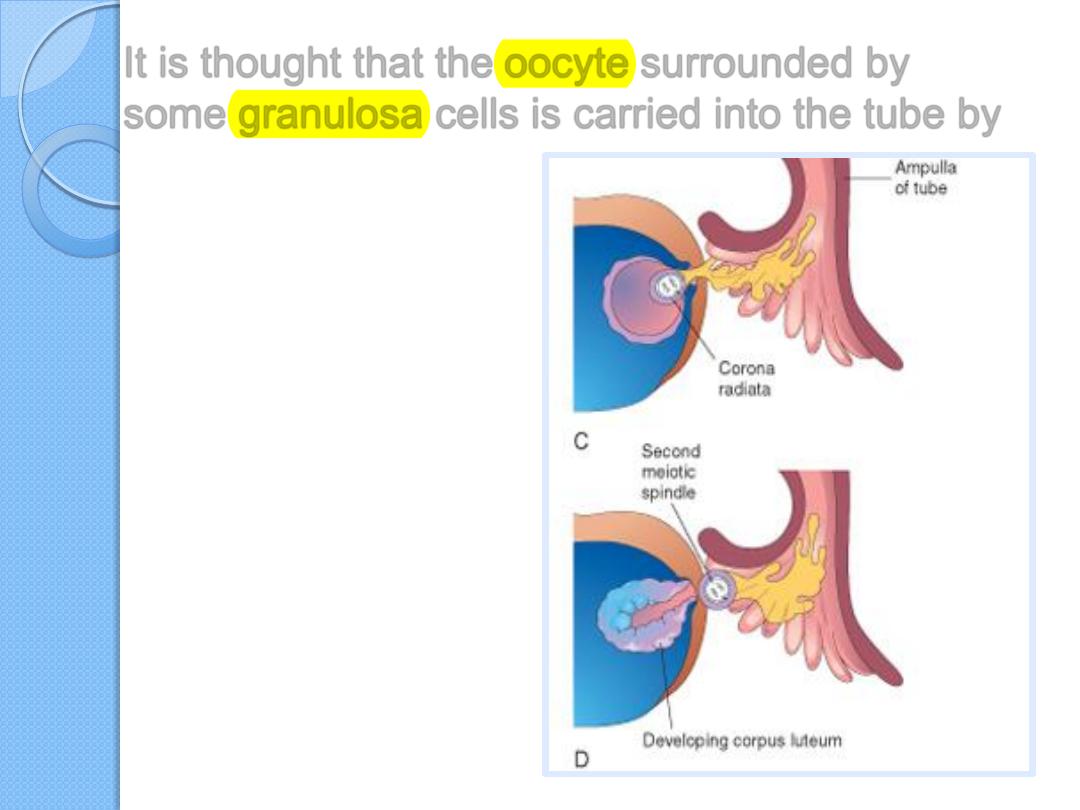
It is thought that the oocyte surrounded by
some granulosa cells is carried into the tube by
•
The sweeping
action of the
fimbriae and
•
fluid currents
produced by the
cilia of the mucosal
cells of the
fimbriae
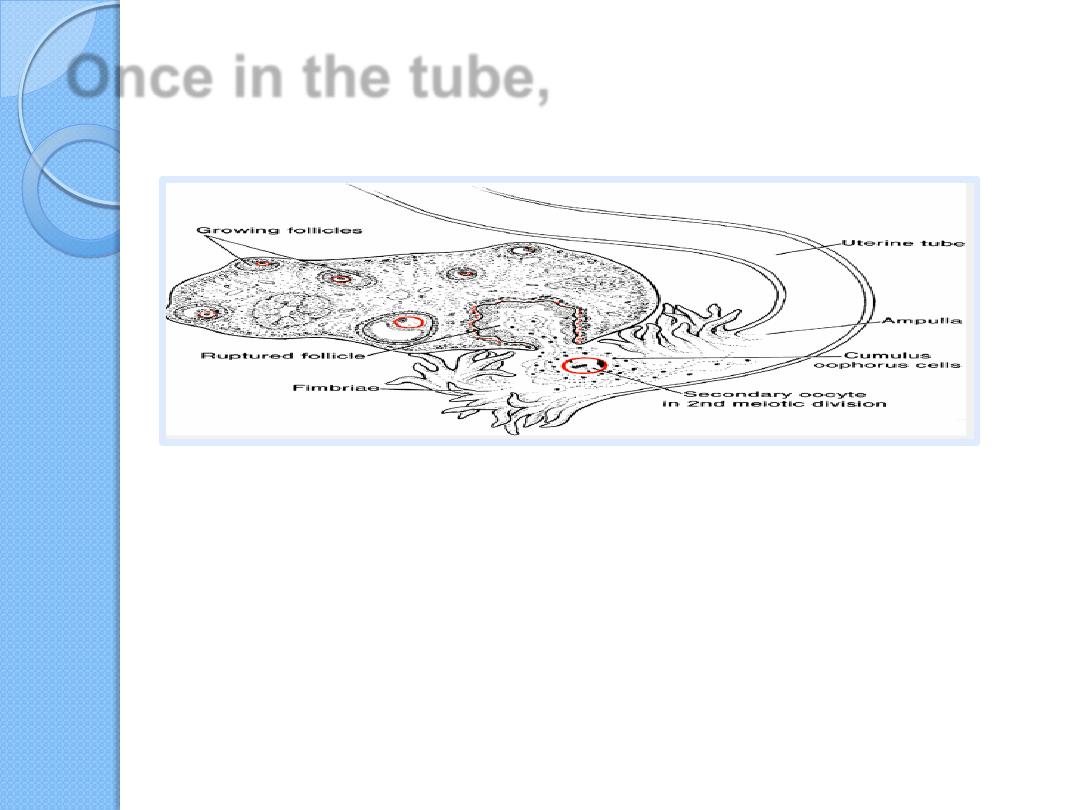
Once in the tube,
cumulus cells withdraw their cytoplasmic processes from
the zona pellucida and lose contact with the oocyte.
The oocyte passes into the
ampulla of the tube
mainly as the result of peristalsis-
movements(alternate contraction and
relaxation) of the wall of the tube
At ovulation, sperm
again become motile, perhaps because of
chemoattractants produced by cumulus
cells surrounding the egg, and
swim to the ampulla, where fertilization
usually occurs .
The oviduct provides the
appropriate environment
not only for fertilization
but for early embryonic development
( the embryo remain there for a period of 3
days ) .
The fertilizable lifespan of gametes
The
oocyte
can be fertilized for up
24 h
after
ovulation
some sperm cells remain viable in the female
reproductive tract for up to
6 days
although
most of them have degenerated after 24h
For fertilization to occur successfully, sexual
intercourse must, therefore, occur between 5
days before and one day after ovulation .
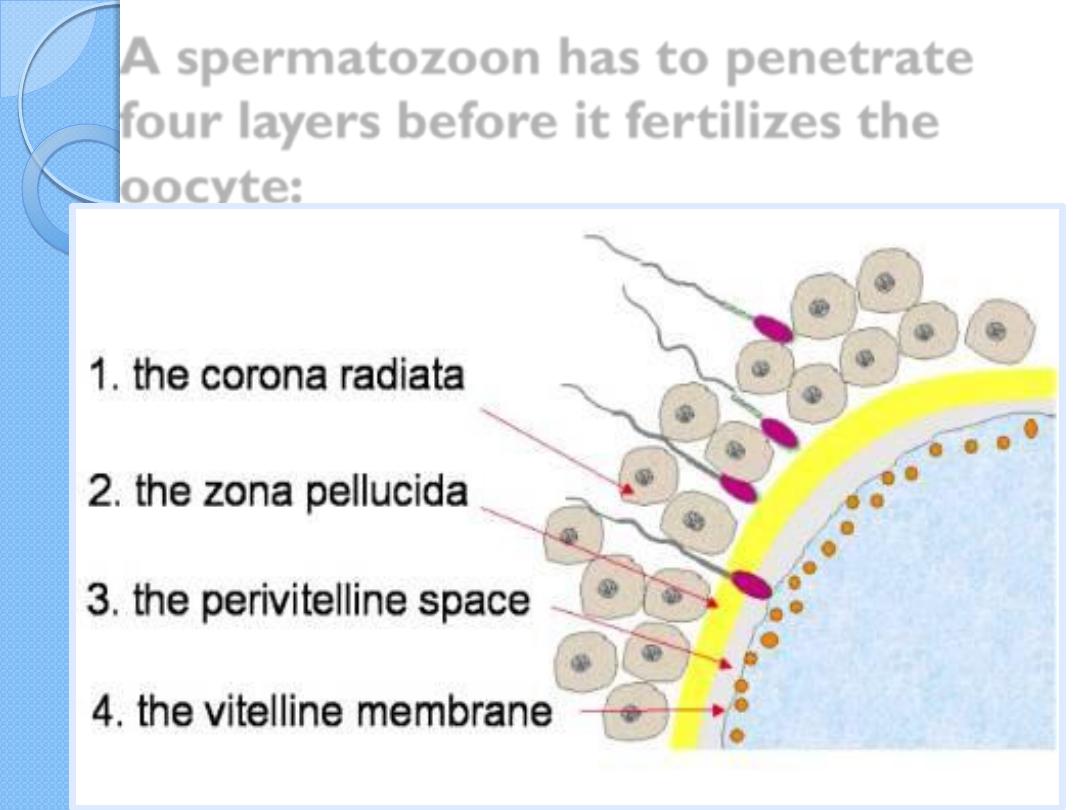
A spermatozoon has to penetrate
four layers before it fertilizes the
oocyte:
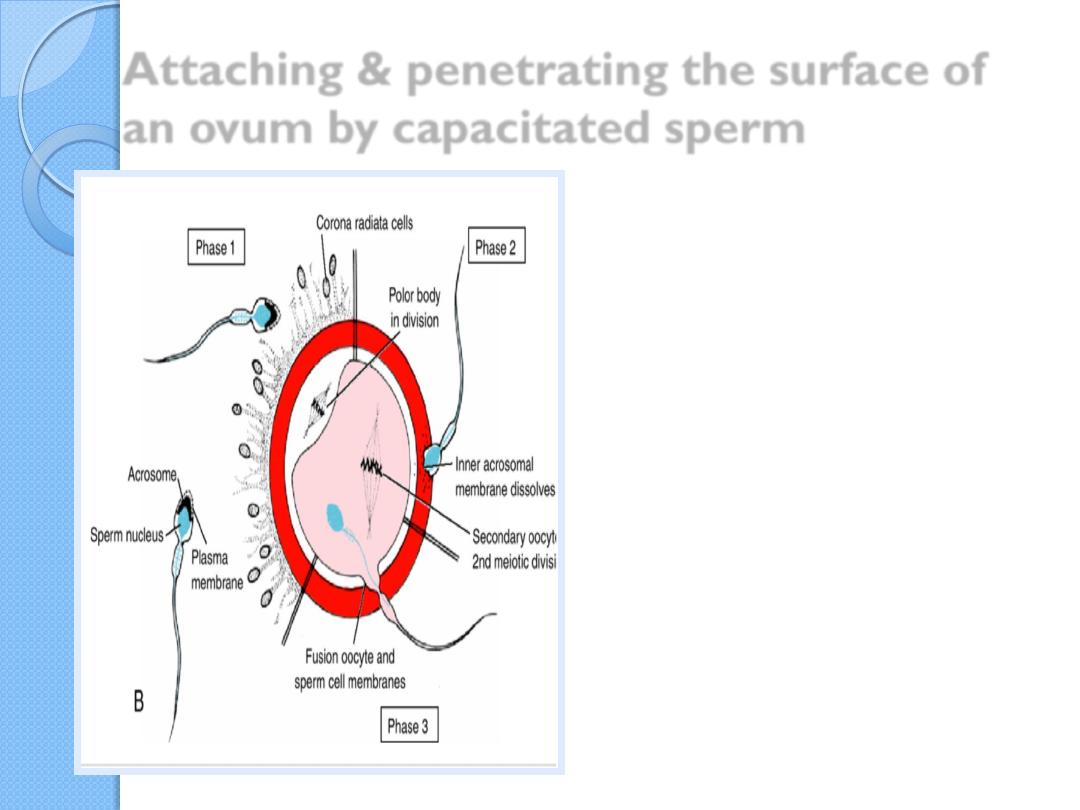
Attaching & penetrating the surface of
an ovum by capacitated sperm
1
. penetration of the
corona radiata
2. penetration of the zona
pellucida
3. penetration of vitelline
membrane
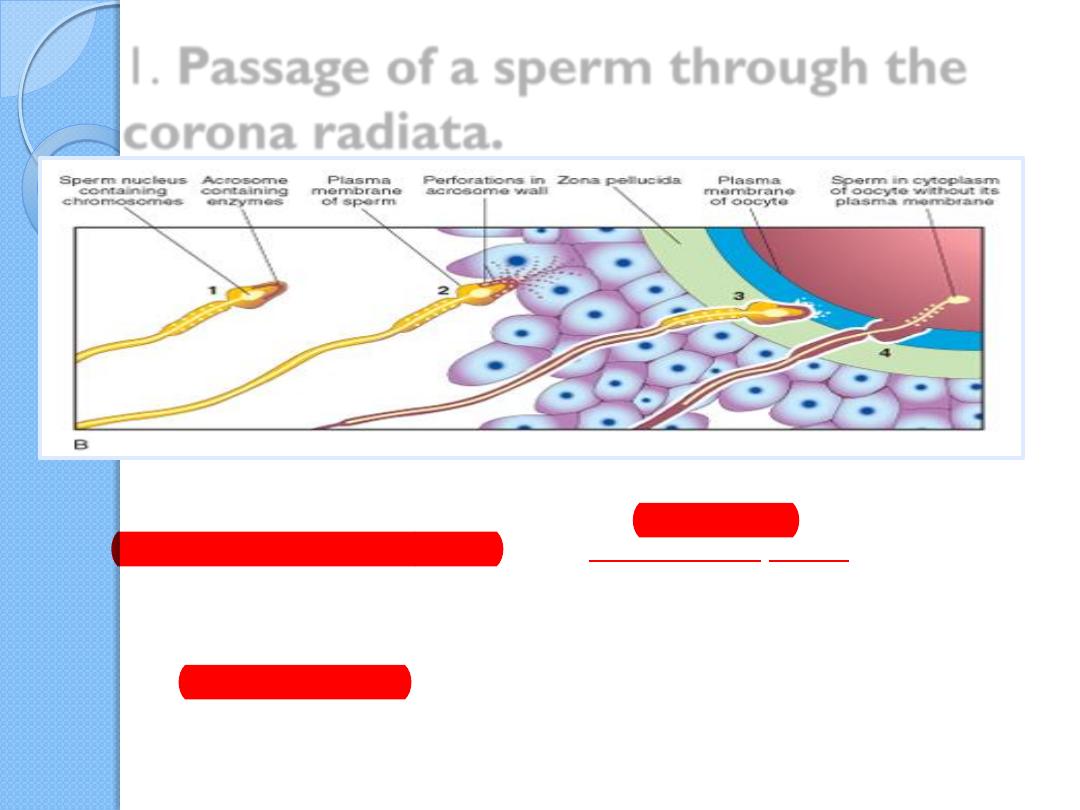
1
. Passage of a sperm through the
corona radiata
.
The corona radiata is a barrier to the sperm cells reaching the oocyte
The sperm cells are propelled through the loose matrix between the
follicular cells of corona radiata by the action of their flagella.
Of the 200 to 300 million spermatozoa deposited in the female genital
tract, only 300 to 500 reach the site of fertilization. Only one of these
fertilizes the egg.
Only capacitated sperm pass freely through corona cells
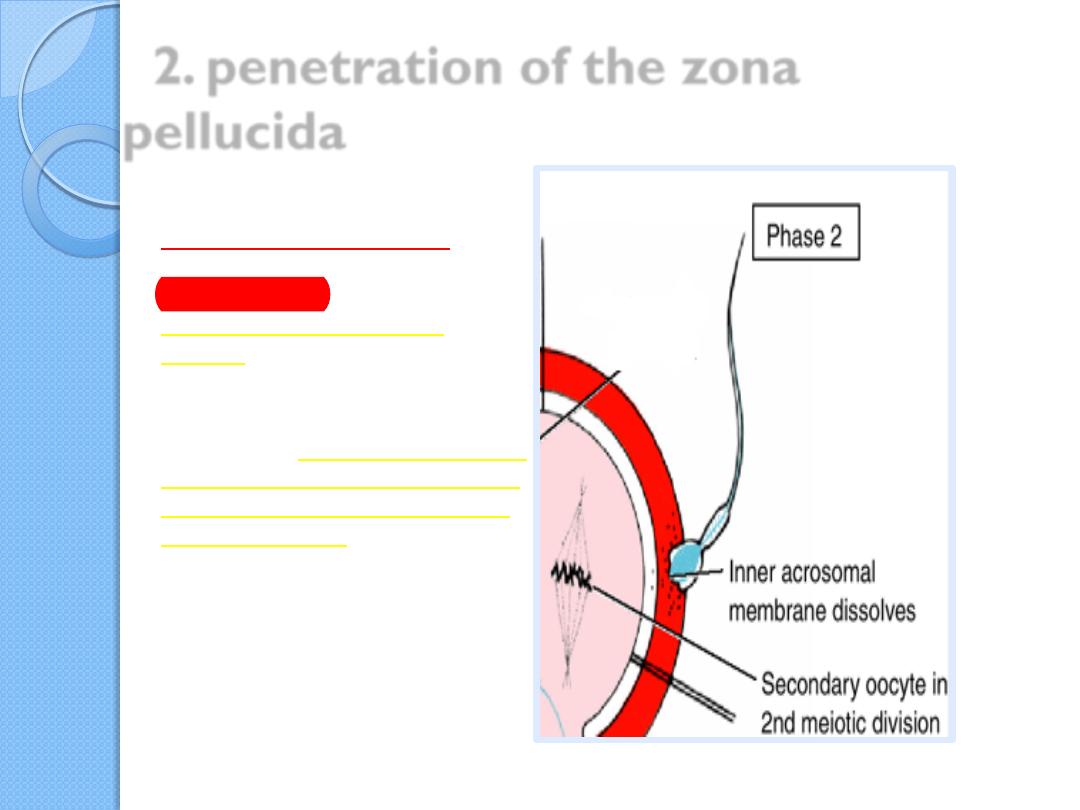
2. penetration of the zona
pellucida
The zona pellucida is an
extracellular membrane ,
comprised mostly of
glycoproteins, between
corona radiata and the
oocyte
One particular zona pellucida
glcoprotein called
zp3
which
is species –specific sperm cell
receptor to which molecules
on the acrosomal cap of the
sperm cell bind .
This binding initiates the
acrosomal reaction
The acrosome reaction
Is stimulated by sperm-binding
glycoprotein molecules in the zona
pellucida (ZP3, ZP1 and ZP2 ligands)
Is accompanied by Ca
2+
influx into sperm
culminates in the release of hydrolytic
enzymes needed to penetrate the zona
pellucida, including acrosin- and trypsin-
like substances.
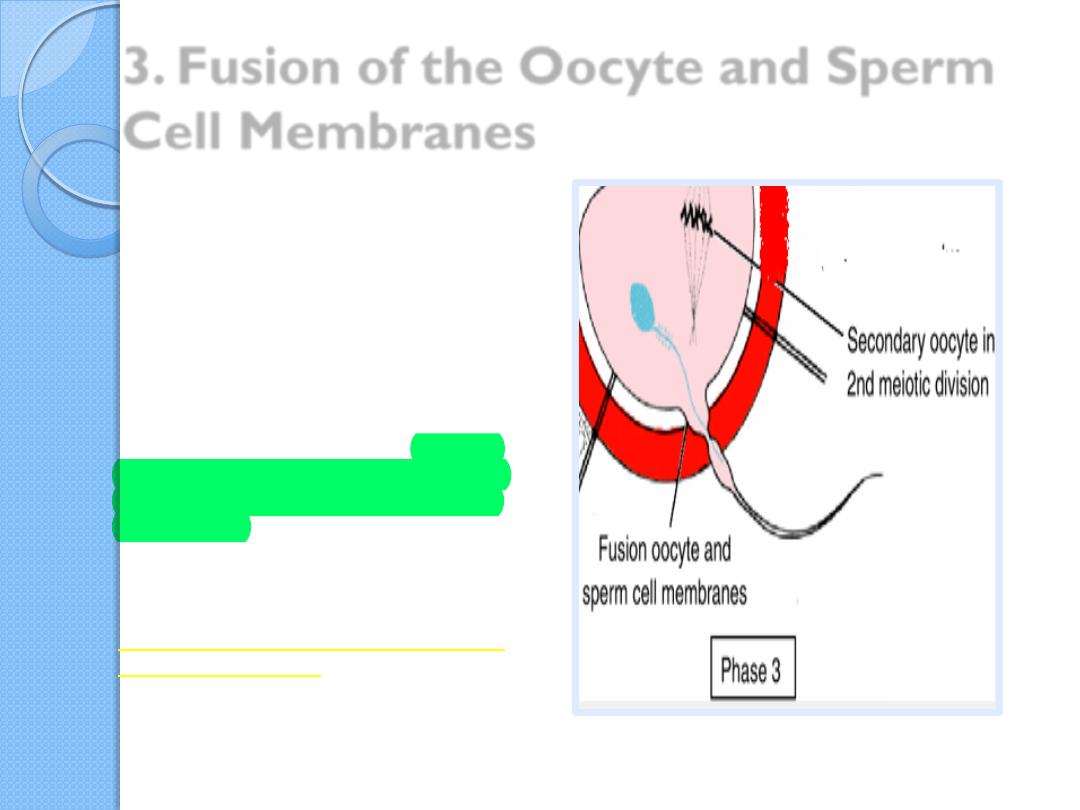
3. Fusion of the Oocyte and Sperm
Cell Membranes
The initial adhesion
of sperm to
the oocyte is mediated in part by
the interaction of
integrins
on the
oocyte and their ligands,
disintegrins
, on sperm.
Because the plasma membrane
covering the acrosomal head cap
disappears during the acrosome
reaction, actual fusion is
accomplished between the oocyte
membrane and the membrane that
covers the posterior region of the
sperm head.
In the human, both the head and tail
of the spermatozoon enter the
cytoplasm of the oocyte, but the
plasma membrane is left behind on
the oocyte surface.
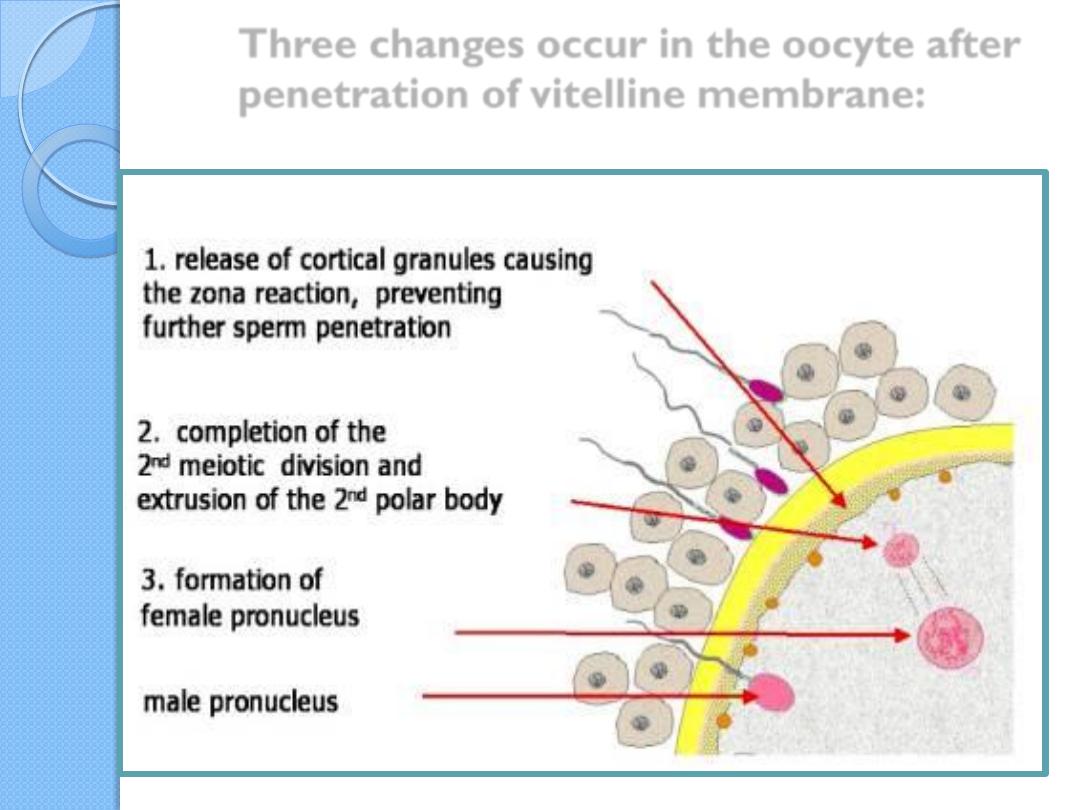
Three changes occur in the oocyte after
penetration of vitelline membrane:
Polyspermy
penetration of more than one
spermatozoon into the oocyte
Prevention of polyspermy
Fast block to polyspermy
Slow block to poly spermy
Prevention of polyspermy
1. Fast block to polyspermy
Once the first sperm cell attaches to the
integrin (alpha 6 beta 1) on the surface of
the oocyte plasma membrane,
depolarization of the oocyte plasma
membrane occurs within 2-3 seconds.
This depolarization( fast block to poly
spermy) prevents additional sperm from
attaching to the oocyte plasma membrane
.
2. Slow block to poly spermy
Depolarization causes the intracellular release
of ca+2 , which in turn causes the exocytosis of
water and other molecules from secretory
vesicles (cortical granules) on the inner surface
of the oocyte plasma membrane
The released fluid causes the oocyte to shrink
and the zona pellucida to denature and expand
away from the oocyte .
As a result of denaturation of the zona
pellucida , zp3 is inactivated and no additional
sperm cells can attach . This reaction is referred
to as the slow block to poly spermy
The early series of changes which
follow “ egg activation “
Prior to fertilization , the egg
is in a quiescent state . Upon
binding of a sperm ,the egg
rapidly
undergoes
a number
of metabolic and physical
changes collectively called
“ egg activation “
Cortical and zona
reactions
Resumption of the
second meiotic division
Metabolic activation of
the egg –The activating
factor is probably
carried by the
spermatozoon.
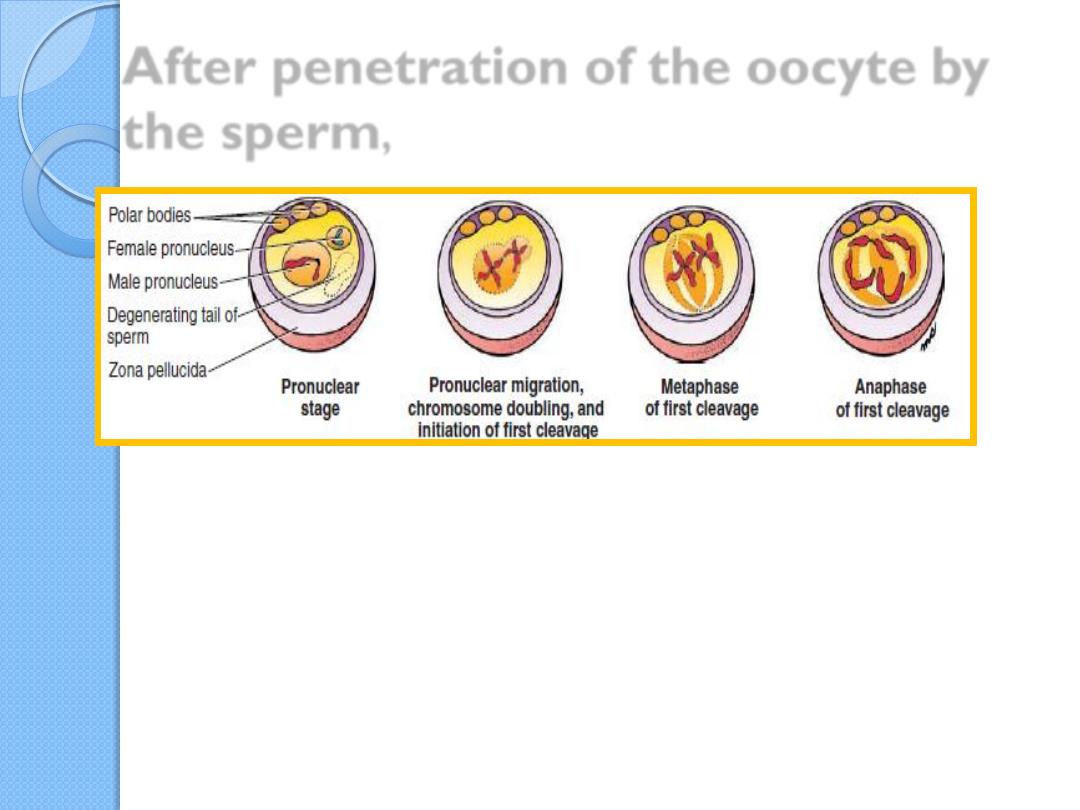
After penetration of the oocyte by
the sperm
,
the oocyte completes meiosis,
the female pronucleus and the larger male pronucleus approach each other as
DNA is doubled in maternal and paternal chromosomes to initiate the first
mitotic division.
Pronuclear membranes then break down and maternal and paternal
chromosomes assemble on the metaphase plate.
Centromeres then replicate, and homologous chromosomes are distributed to
the first two cells of the embryo.
The cytoplasmic organelles of the zygote
are almost entirely maternal
Mitochondrial DNA is almost entirely
maternal
Mitochondrial genetic diseases are generally
inherited through the mother but may affect
both sons and daughters
Most mitochondrial diseases affect muscle
and nerve
Examples of mitochondrial inheritance are:
– mitochondrial myopathy (affects muscle)
– Leber’s optic atrophy (affects optic nerve)
The main results of fertilization
Restoration of the diploid number of
chromosomes, , the zygote contains a new
combination of chromosomes different from
both parents.
Determination of the sex of the new individual.
An X-carrying sperm produces a female (XX)
embryo, and a Y-carrying sperm produces a male
(XY) embryo. Hence, the chromosomal sex of
the embryo is determined at fertilization.
Initiation of cleavage.
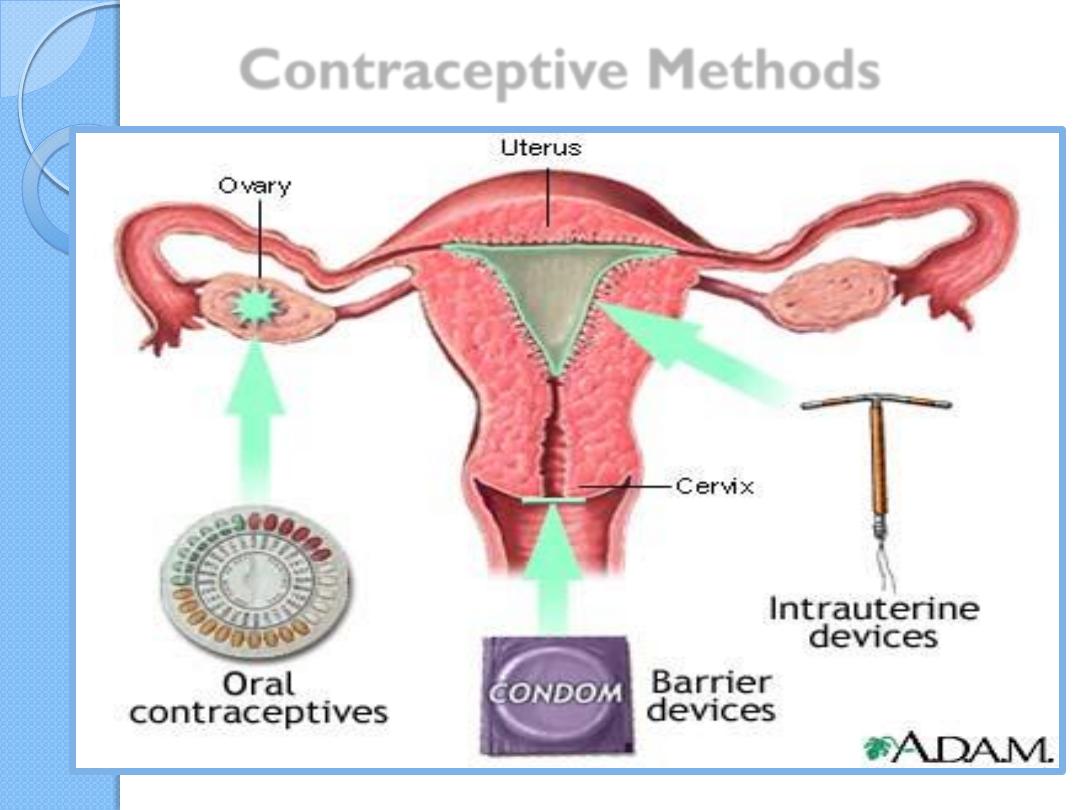
Contraceptive Methods
Barrier techniques of contraception
include
the male condom, and
the female condom
the diaphragm,
the cervical cap, and
the contraceptive sponge.
Prevention of ovulation
The contraceptive pill
is a
combination of estrogen and the
progesterone which together
inhibit ovulation but permit
menstruation.
Depo-Provera
is a progestin
compound that can be implanted
subdermally or injected
intramuscularly to prevent
ovulation for up to 5 years or 23
months.
A male “pill”
has been developed and tested in clinical trials.
It contains a
synthetic androgen
that prevents
both LH and FSH secretion
It
either
stops sperm production (70% to 90% of men)
or
reduces it to a level of infertility.
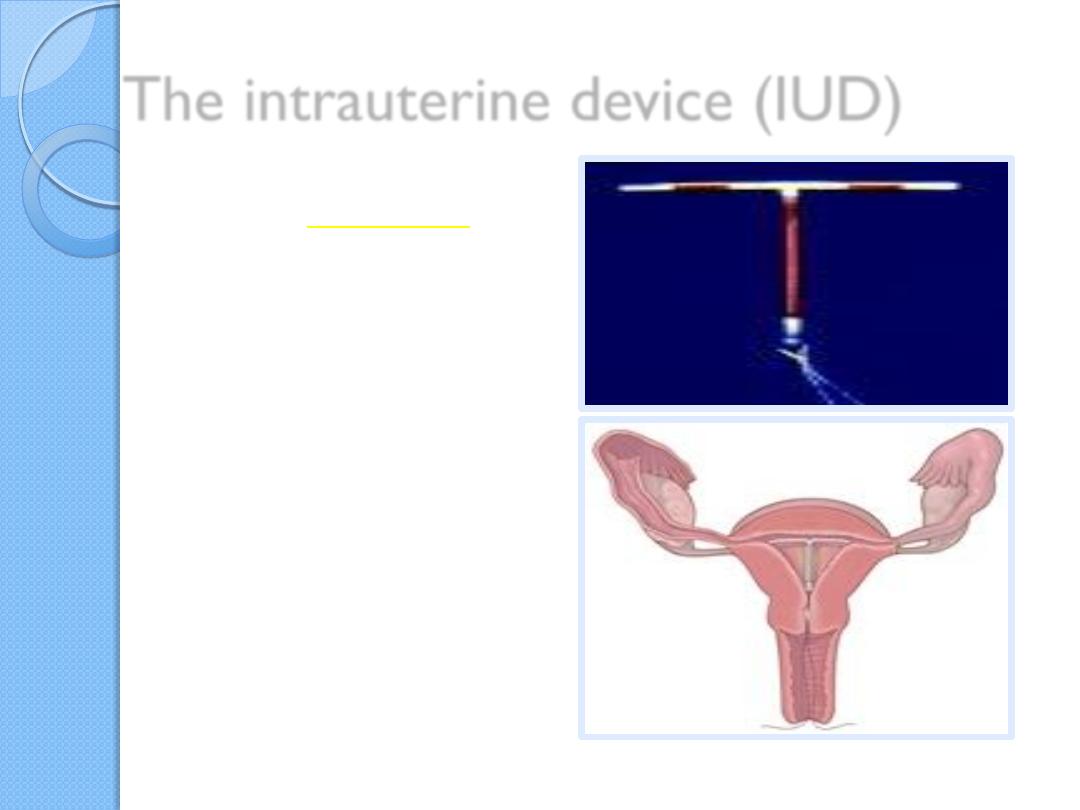
The intrauterine device (IUD)
is placed in the uterine cavity.
Its mechanism for preventing
pregnancy is not clear but
may entail direct effects on sperm
and oocytes or
inhibition of preimplantation stages
of development.
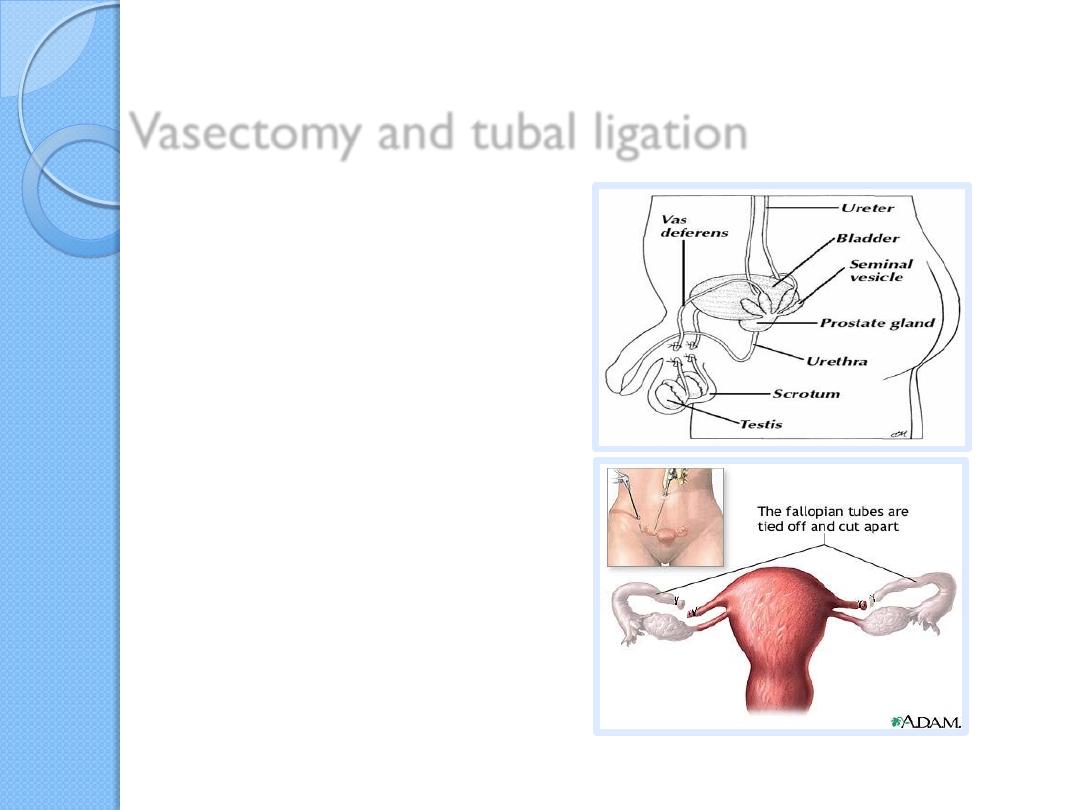
Vasectomy and tubal ligation
are effective means of
contraception, and
both procedures are reversible,
although not in every case.
Infertility is a problem for 15% to
30% of couples.
Male Infertility
be a result of insufficient
numbers of sperm and/or
poor motility.
Female Infertility
occluded uterine tubes
(most commonly caused
by pelvic inflammatory
disease),
hostile cervical mucus,
immunity to spermatozoa,
absence of ovulation, and
others.
Assisted reproductive
technology (ART)
is a group of fertility treatments that involve both the
sperm and the egg.
Assisted reproductive
technology (ART)
In vitro fertilization (IVF)
intracytoplasmic sperm injection (ICSI)
gamete intrafallopian transfer (GIFT)
zygote intrafallopian transfer (ZIFT).
In vitro fertilization
(IVF)
is the most common
type of ART.
the sperm fertilizes the egg
outside the body, and doctors
implant it into the woman's
uterus in hopes of a successful
pregnancy.
IVF cycle takes four to six weeks
to complete and usually costs
about $12,000
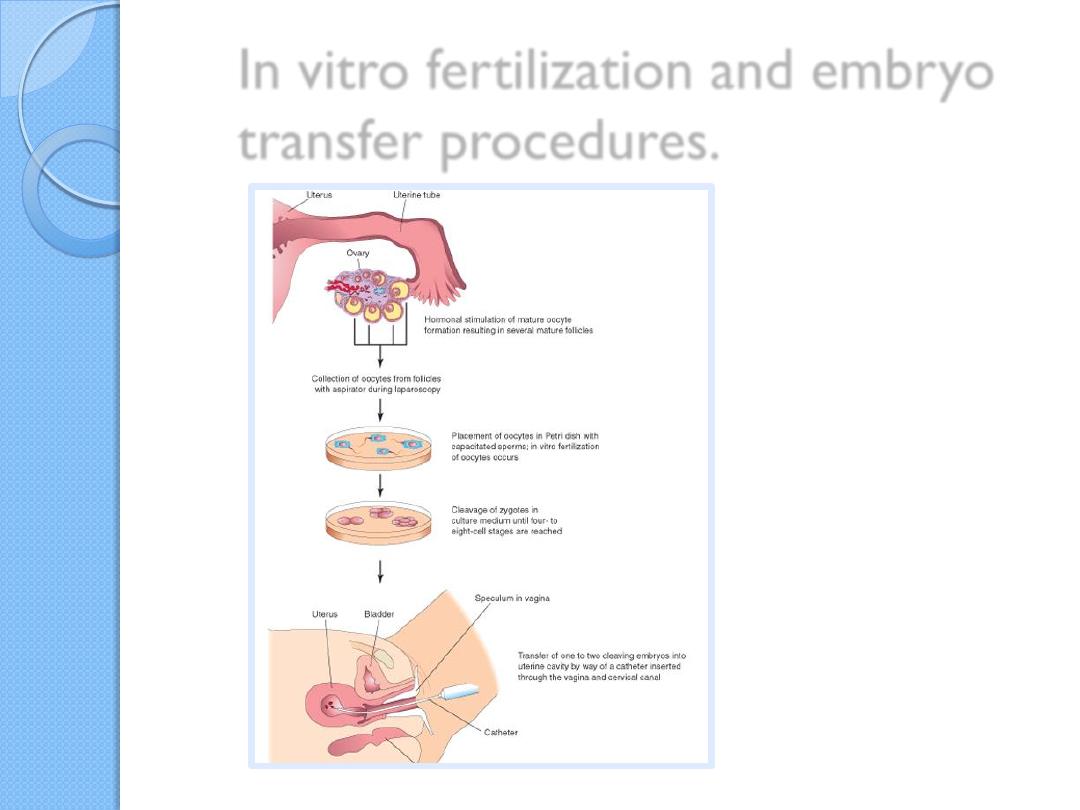
In vitro fertilization and embryo
transfer procedures.
In vitro Fertilization ( IVF )
The risk of
producing
malformed offspring
by in vitro
procedures is low
.
because
preimplantation-
stage embryos
are
resistant to
teratogenic insult,
A disadvantage of IVF is its low
success rate
only
20% of
fertilized ova
implant and
develop to term.
Therefore, to increase chances
of a successful pregnancy,
four
or five ova are collected,
fertilized, and placed in the
uterus
. This approach
sometimes leads to
multiple
births.
The following methods of ART require
patent uterine tubes.
Gamete intrafallopian
transfer (GIFT)
oocytes and sperm
into the ampulla of
the fallopian
(uterine) tube,
where fertilization
takes place.
zygote intrafallopian
transfer (ZIFT)
fertilized oocytes are
placed in the
ampullary region.
(Intracytoplasmic sperm
injection ICSI)
(oligozoospermia) or even (azoospermia),
can be overcome by using
intracytoplasmic sperm injection (ICSI).
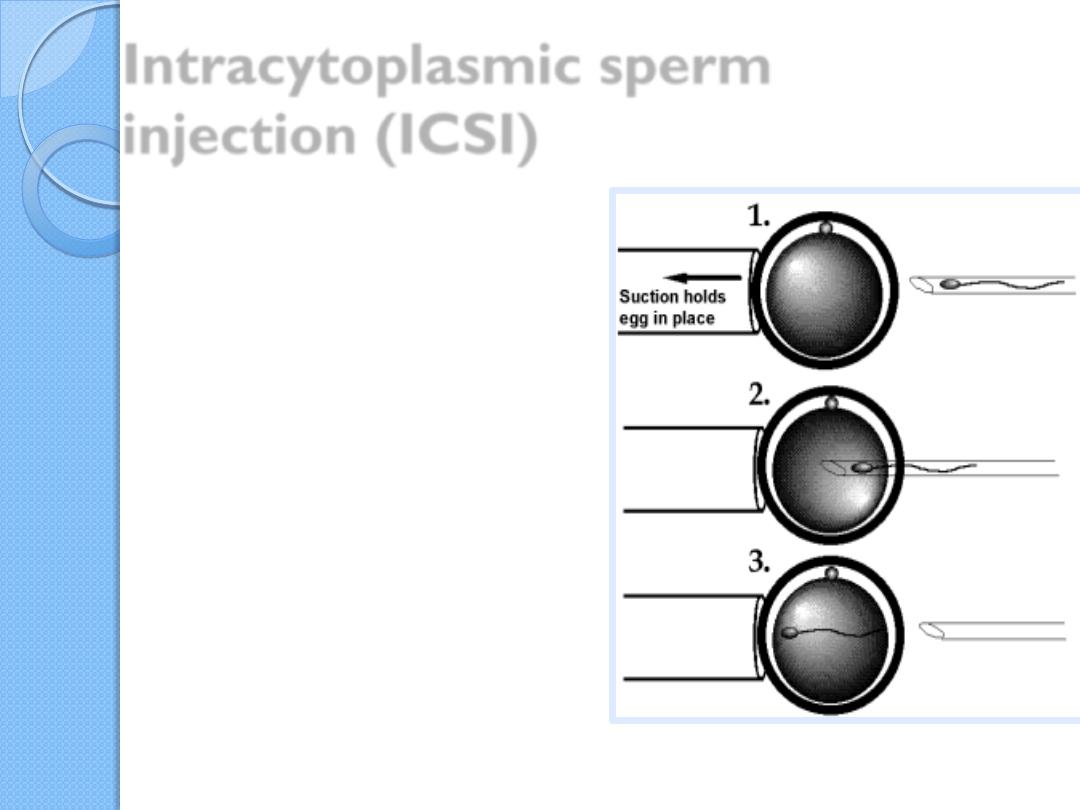
Intracytoplasmic sperm
injection (ICSI)
With this technique, a
single sperm, which may
be obtained from any
point in the male
reproductive tract, is
injected into the
cytoplasm of the egg to
cause fertilization.
The technique carries
an increased risk for
fetuses to have Y
chromosome deletions
but no other
chromosomal
abnormalities.
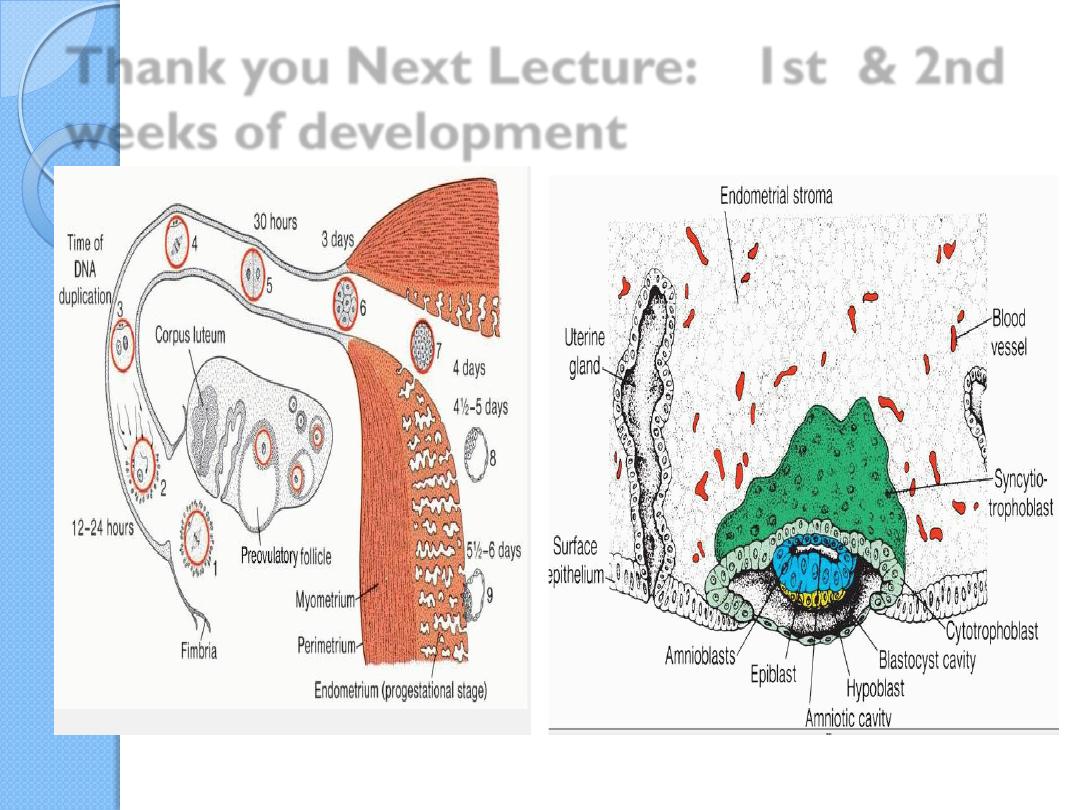
Thank you Next Lecture: 1st & 2nd
weeks of development

Key words of next lecture
Blastocyst
Blastomeres
Morula
Inner cell mass
Outer cell mass
Trophoblast
Embryoblast
Cytotrophoblast
Syncytiotrophoblast
Hypoblast
Epiblast
amniotic cavity
Exocoelomic cavity
(primitive yolk sac)
Extraembryonic mesoderm
Extraembryonic cavity(
chorionic cavity)
Extraembryonic somatic
mesoderm
Extraembryonic splanchnic
mesoderm
Secondary yolk sac (
definitive yolk sac)