Urinary System
Prof. Dr. Malak A. Al-yawer
Learning Objectives
At the end of this lecture, the medical student will be able to:
Explain the following statement “ the genital and urinary systems
are intimately interwoven embryologically and anatomically”
Identify the three stages of kidney development and give
characteristics of each of the stages
List the adult derivatives of the embryonic structures of each of
the early kidney stages
Describe the ascent of the kidneys including changes to arterial
blood supply
List the three components of the uro-genital sinus and describe
their adult derivatives
Explain the formation of the urinary bladder proper
List some clinical correlates
Urogenital System
can be divided into two
entirely different
components:
1.
Urinary system
2. Genital system
Embryologically and anatomically, they are
intimately interwoven
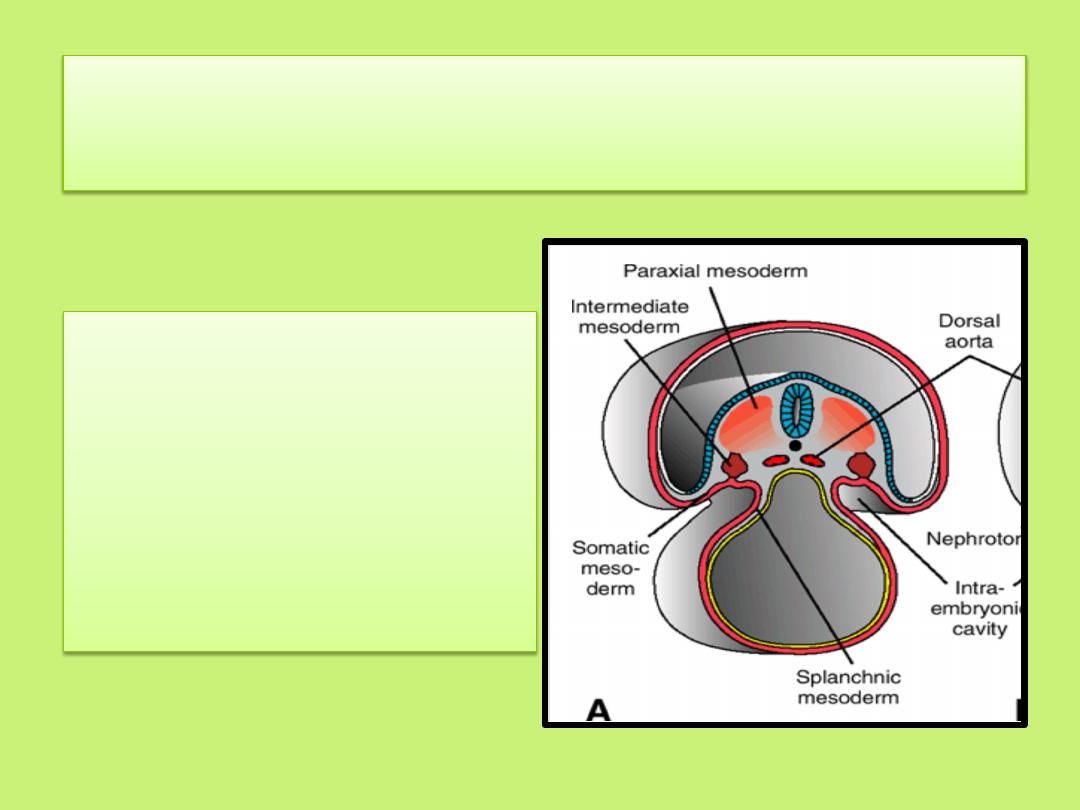
Both systems
(a)
develop from
intermediate mesoderm (uro
genital ridge): a common mesodermal ridge along
the posterior wall of the abdominal cavity
(b) initially the excretory ducts of both systems
enter a common cavity, the cloaca.
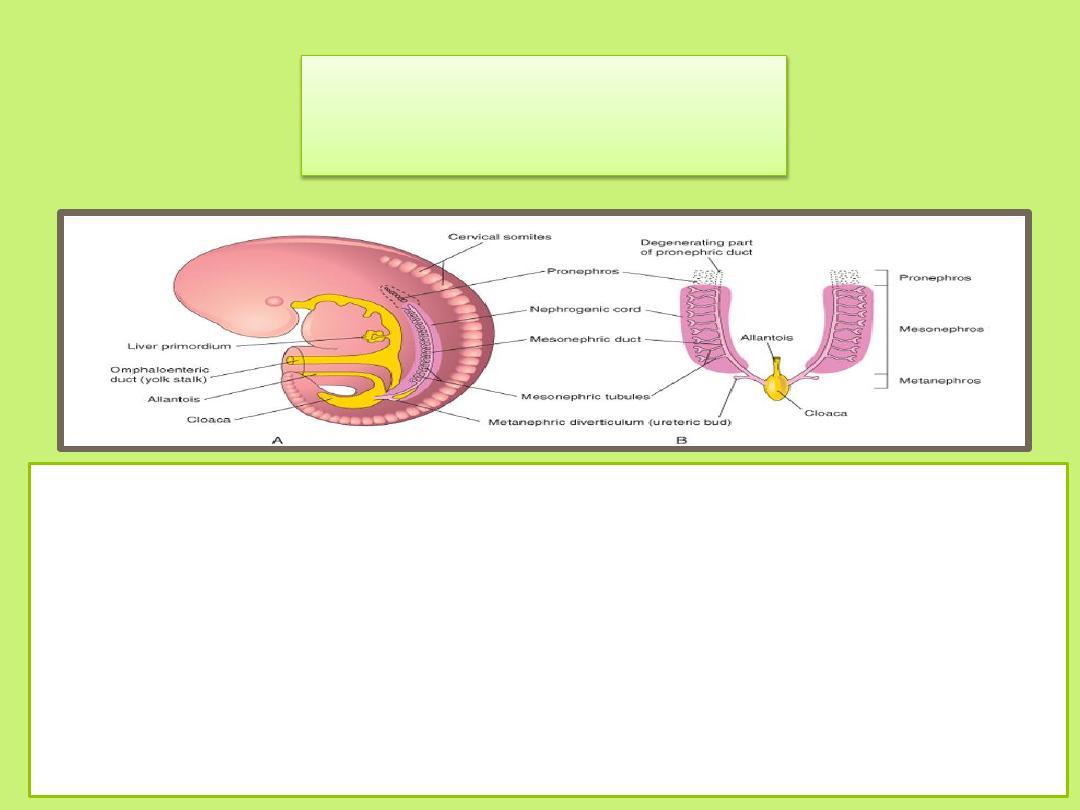
Kidney Systems
Three slightly overlapping kidney systems are formed in a
cranial to caudal sequence during intrauterine life in humans:
(a) pronephros: rudimentary and nonfunctional
(b) mesonephros : may function for a short time during the early
fetal period
(c) metanephros: forms the permanent kidney.
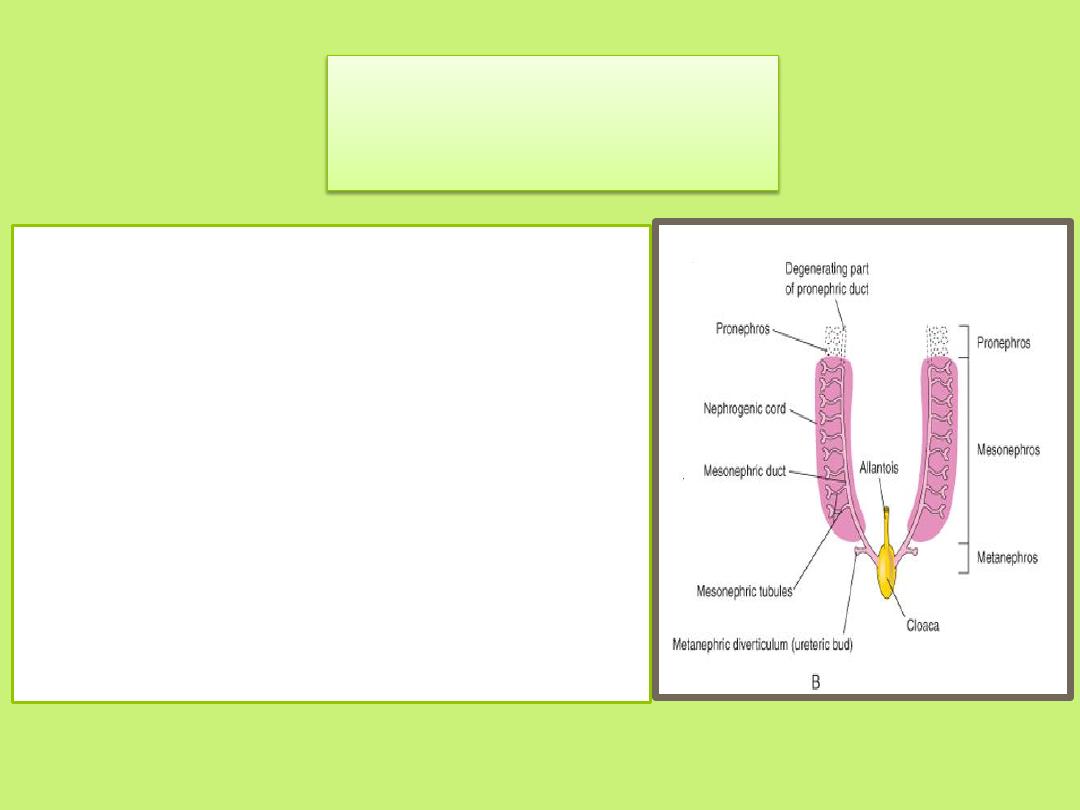
Pronephros
• At the beginning of the 4
th
week, the
pronephros is represented by 7 to 10
solid cell groups in the cervical region,
nephrotomes, that regress before
more caudal ones are formed.
• The pronephric ducts run caudally and
open into the cloaca
• By the end of the 4
th
week, the
pronephroi soon degenerate; however,
most of the length of the pronephric
ducts persists and is used by the next
set of kidneys.
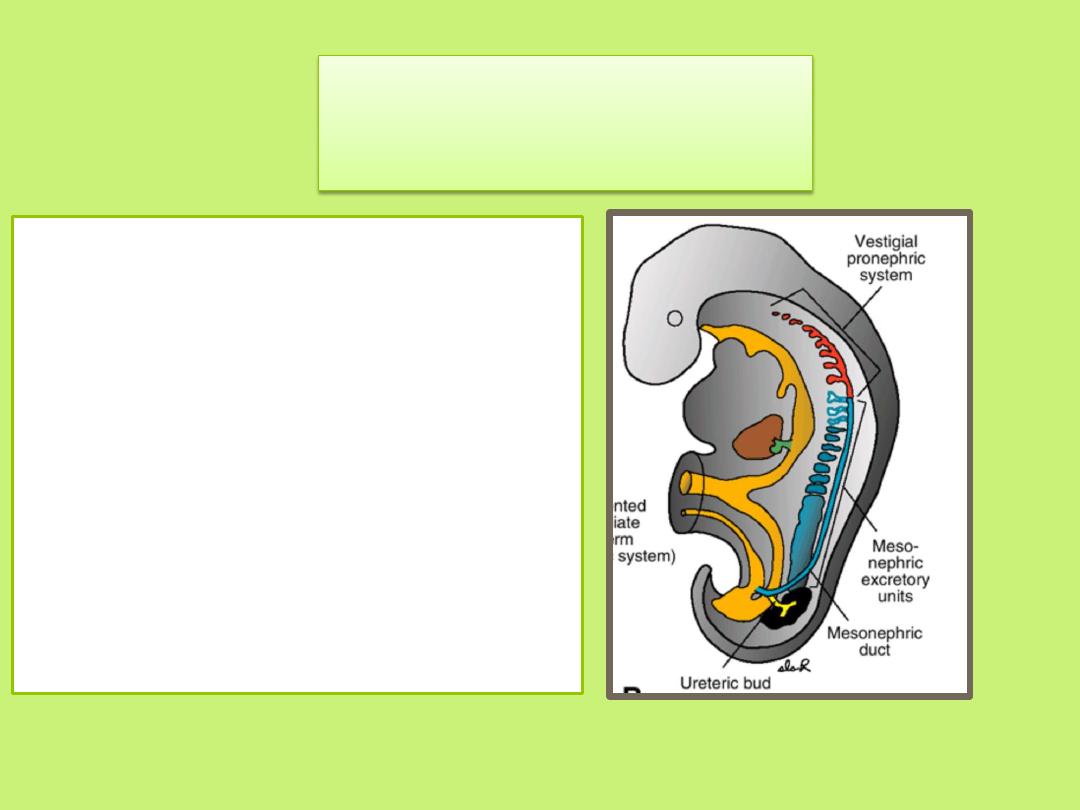
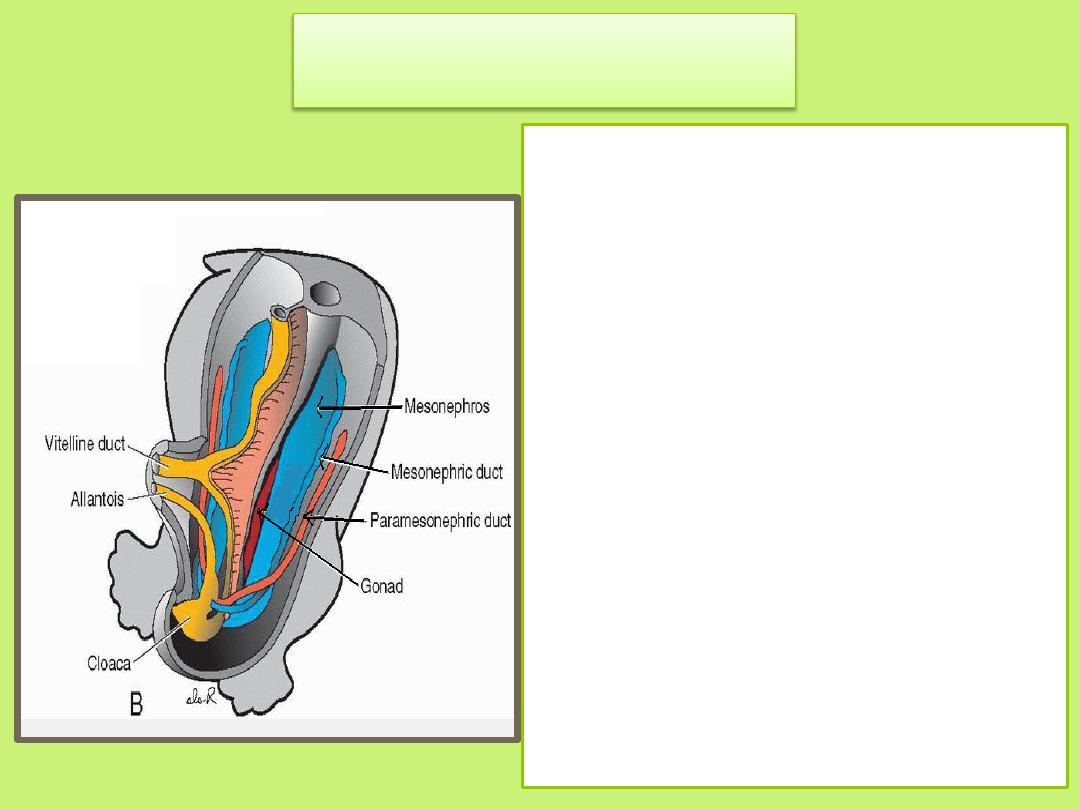
Mesonephros
• The mesonephros and
mesonephric ducts are derived
from intermediate mesoderm
from upper thoracic to upper
lumbar (L3) segments.
Mesonephros –Urogenital ridge
• In the middle of the second month
the mesonephros forms a large
ovoid organ on each side of the
midline.
• Since the developing gonad is on
its medial side, the ridge formed
by both organs is known as the
Urogenital ridge.
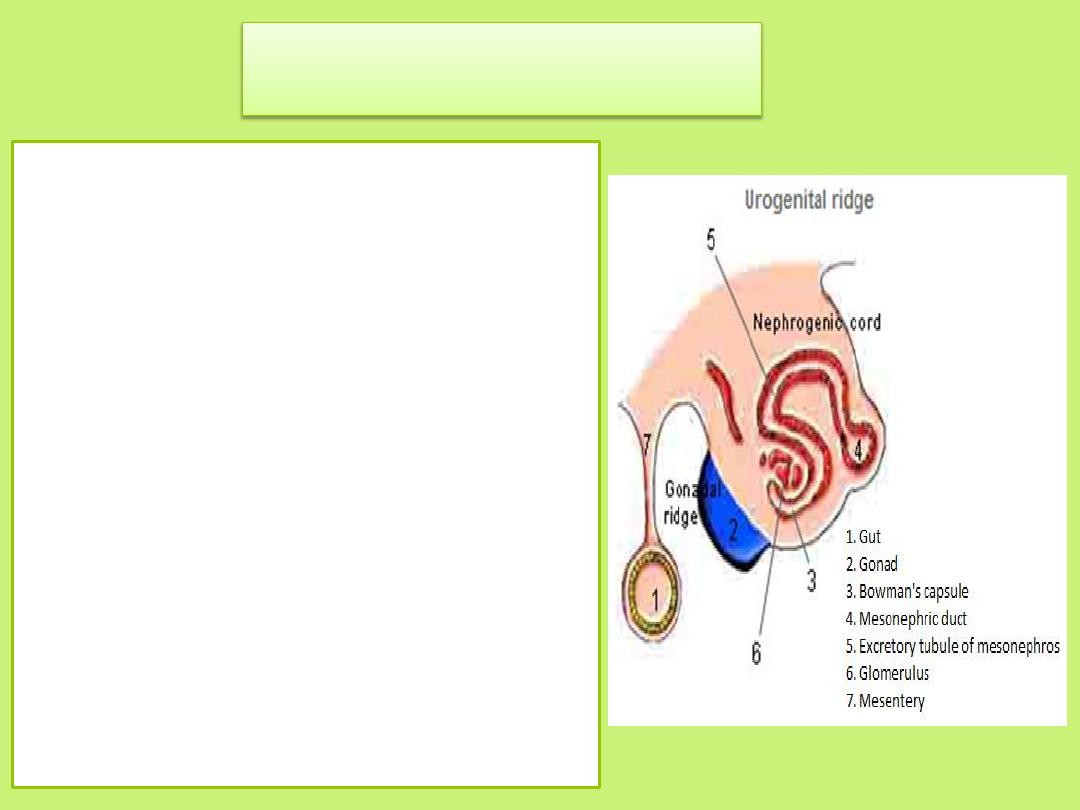
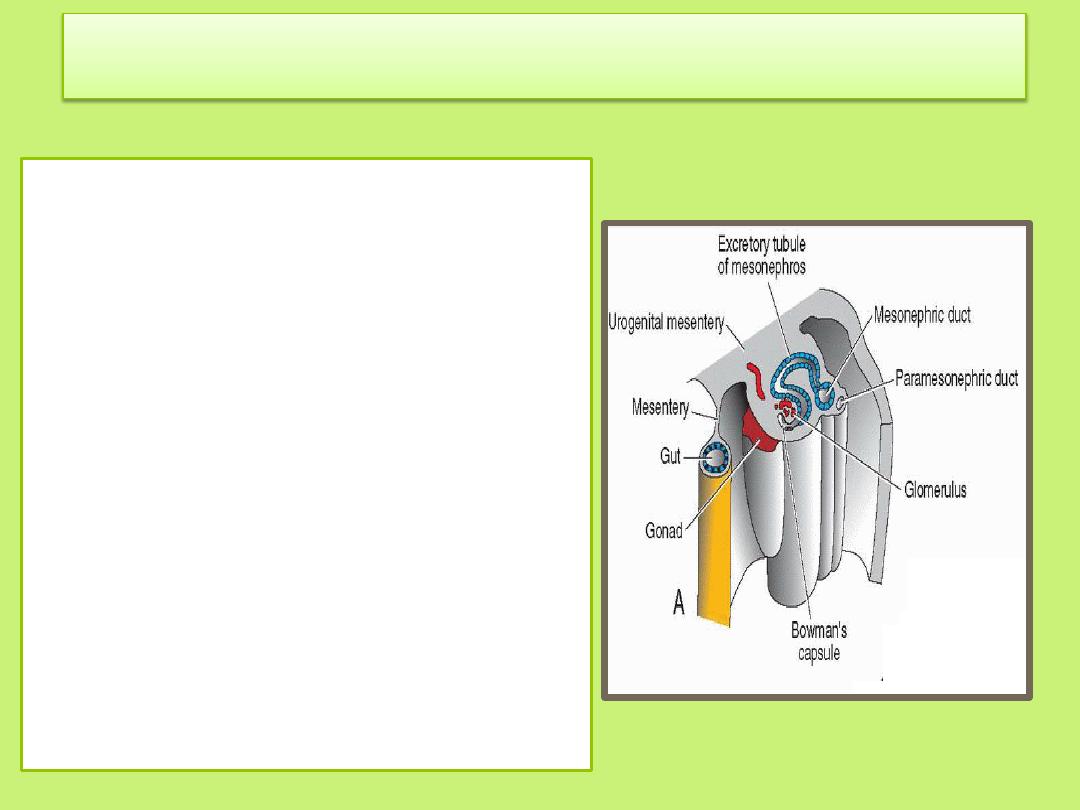
Mesonephros
• During regression of the
pronephric system, the first
excretory tubules of the
mesonephros appear. They
lengthen rapidly, form an S-
shaped loop, and acquire a tuft
of capillaries that will form a
glomerulus at their medial
extremity.
• Around the glomerulus the
tubules form Bowman's capsule,
and together these structures
constitute a renal corpuscle.
Mesonephrons
• Laterally, the tubule enters the
longitudinal collecting duct
known as the mesonephric or
wolffian duct.
• By the end of the second month,
the majority of excretory tubules
have disappeared.
• In the male, a few of the caudal
tubules and the mesonephric
duct persist and participate in
formation of the conduit for
sperm from the testes to the
urethra. In the female, these
ducts regress.
Metanephros
• appears in the 5
th
week.
• develops from the lower lumber
and sacral portions of the
nephrogenic cord
• Its excretory units develop in the
same manner as in the
mesonephric system.
• The development of the duct
system differs from that of the
other kidney systems.
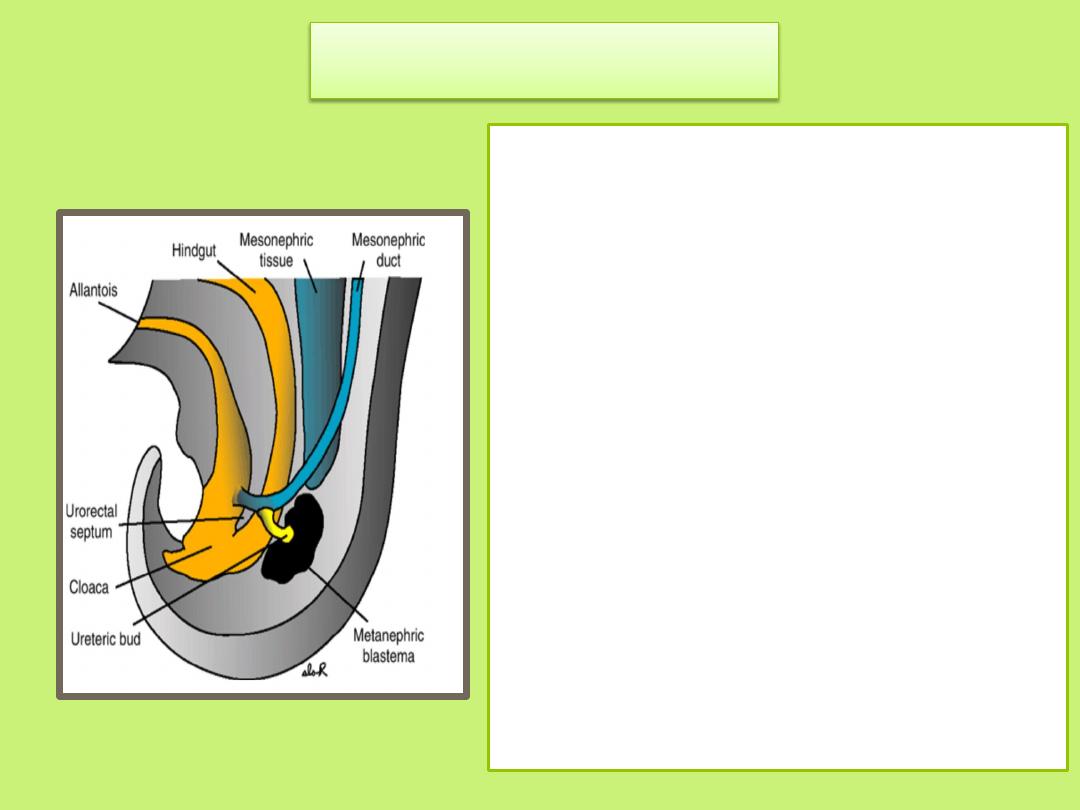
Collecting System
• Collecting ducts of the
permanent kidney develop
from the ureteric bud ( an
outgrowth of the mesonephric
duct close to its entrance to
the cloaca ).
• The bud penetrates the
metanephric tissue, which is
molded over its distal end as a
cap.
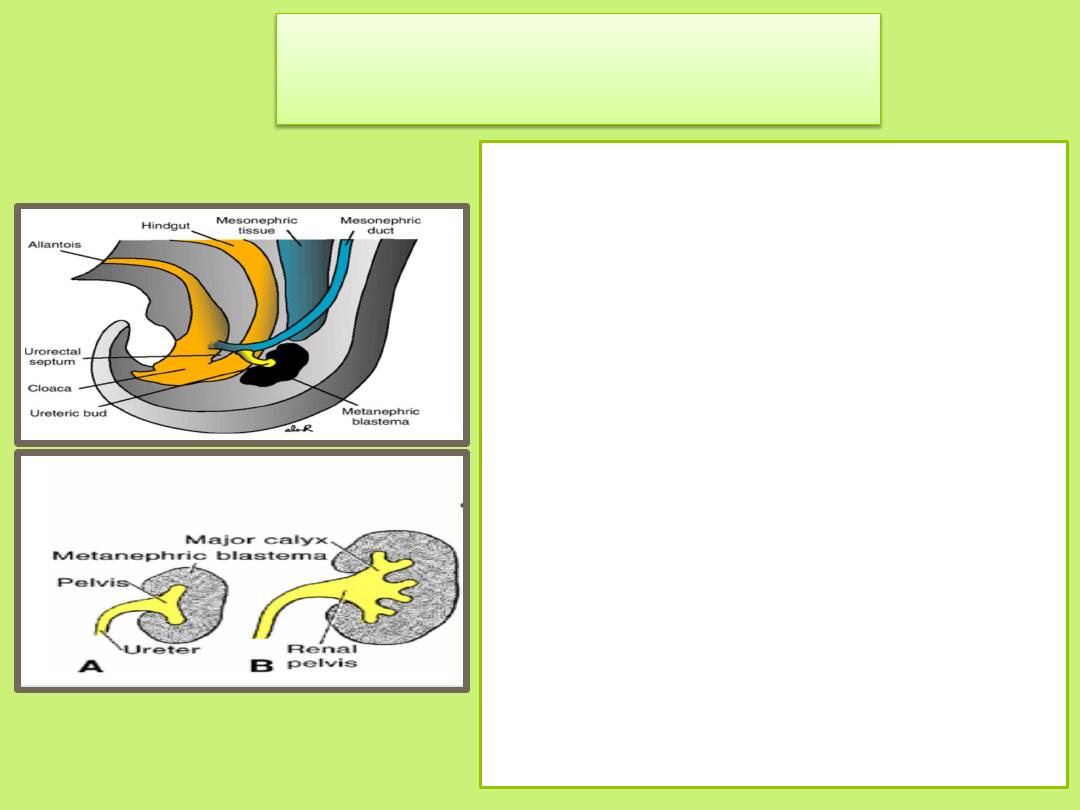
• Subsequently the bud dilates,
forming the primitive renal
pelvis, and splits into cranial
and caudal portions, the
future major calyces
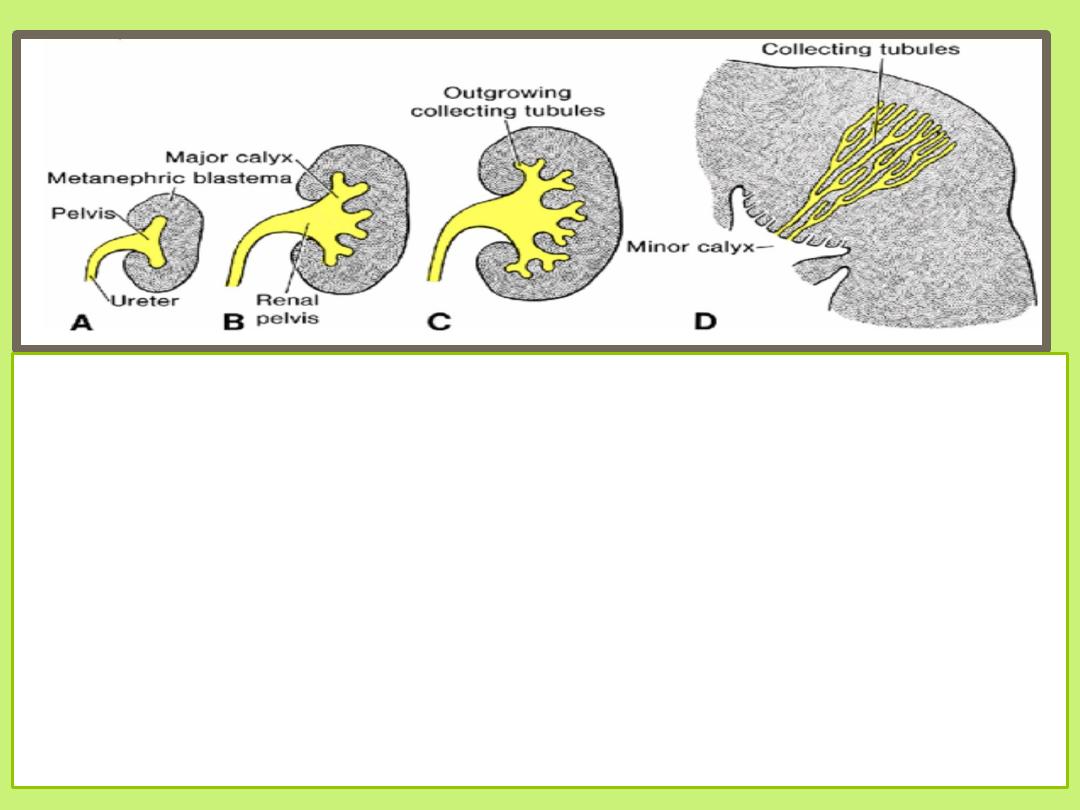
• Each calyx forms two new buds which continue to subdivide until
12 or more generations of tubules have formed.
• The tubules of the second order enlarge and absorb those of the
third and fourth generations, forming the minor calyces of the renal
pelvis.
• During further development, collecting tubules of the fifth and
successive generations elongate considerably and converge on the
minor calyx, forming the renal pyramid
• The ureteric bud gives rise to the ureter, the renal pelvis, the major
and minor calyces, and approximately 1 to 3 million collecting
tubules
.
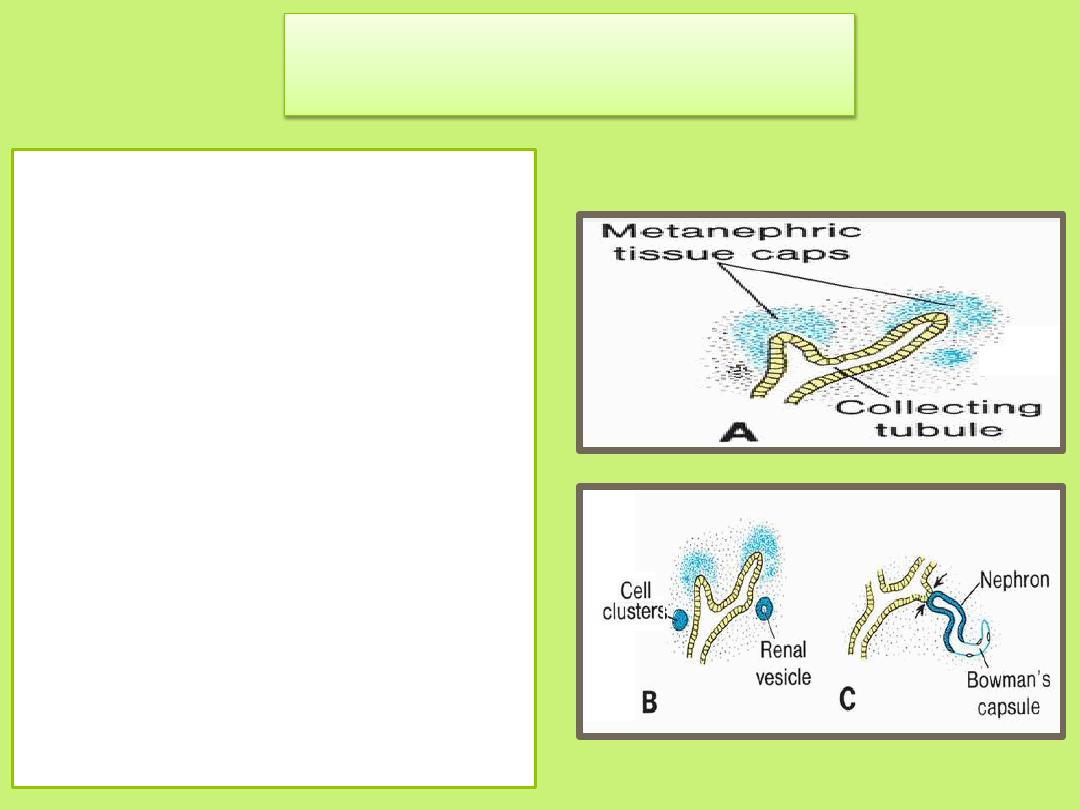
Excretory System
• Each newly formed
collecting tubule is
covered at its distal end by
a metanephric tissue cap .
• Under the inductive
influence of the tubule,
cells of the tissue cap form
small vesicles, the renal
vesicles, which in turn give
rise to small S-shaped
tubules.
Excretory System
• Capillaries grow into the
pocket at one end of the S
and differentiate into
glomeruli.
• The proximal end of each
nephron forms Bowman's
capsule, which is deeply
indented by a glomerulus.
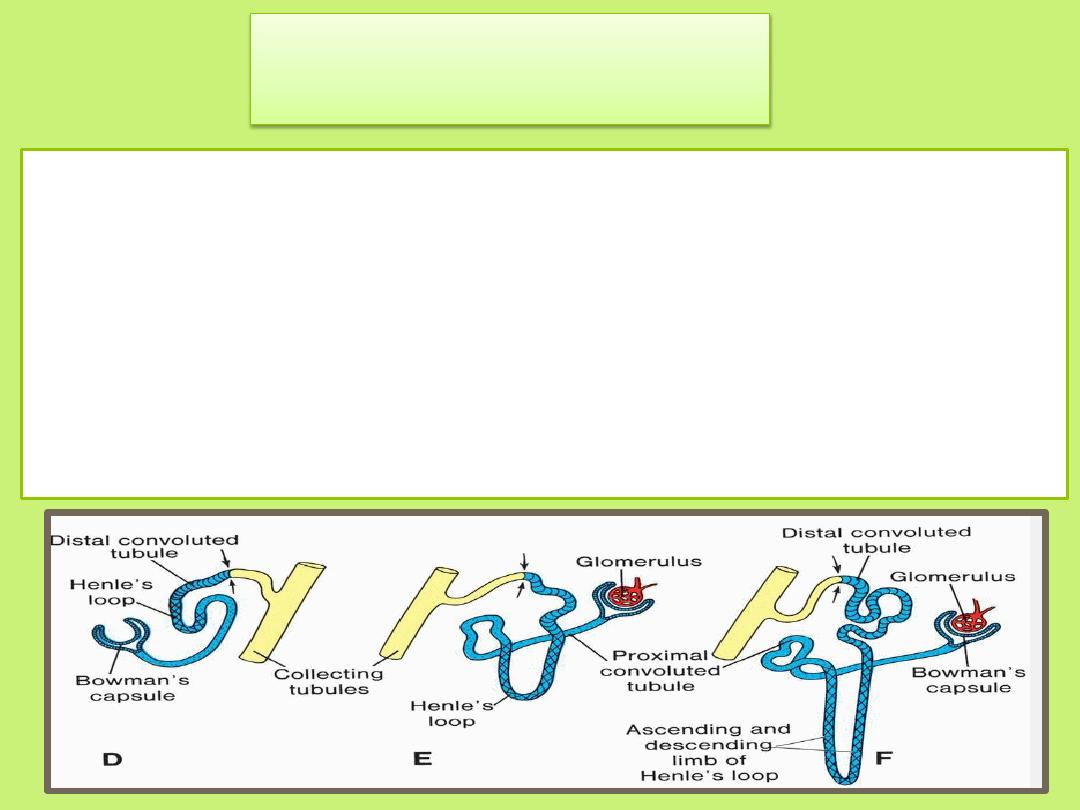
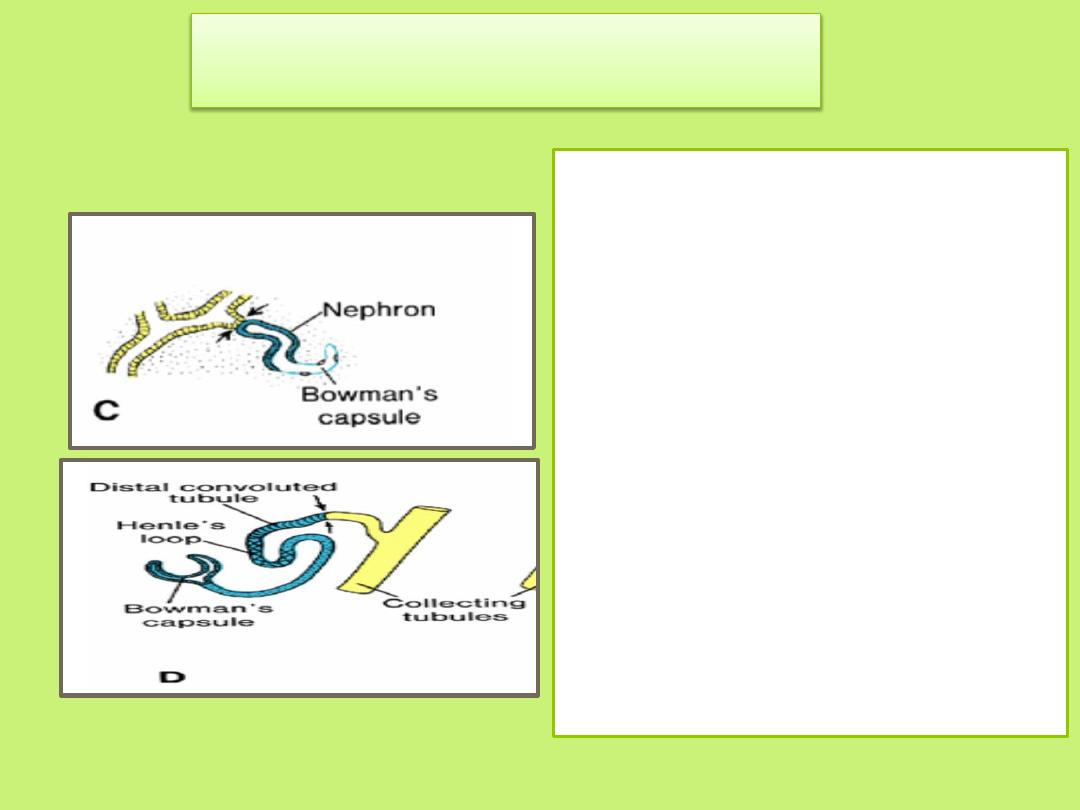
Excretory System
• The distal end forms an open connection with one of the
collecting tubules.
• Continuous lengthening of the excretory tubule results in
formation of the proximal convoluted tubule, loop of
Henle, and distal convoluted tubule
• Hence, the kidney develops from two sources:
Metanephric mesoderm, which provides
excretory units
Ureteric bud, which gives rise to the collecting
system.
• There are approximately 1
million nephrons in each
kidney. They are formed until
birth.
• Urine production begins soon
after differentiation of the
glomerular capillaries, which
start to form by the 10th week.
The definitive kidney becomes
functional near the 12th week.
• During fetal life, the kidneys are
not responsible for excretion of
waste products, since the
placenta serves this function.
• At birth, the kidneys have a
lobulated appearance, but
the lobulation disappears
during infancy as a result of
further growth of the
nephrons, although there is
no increase in their number.
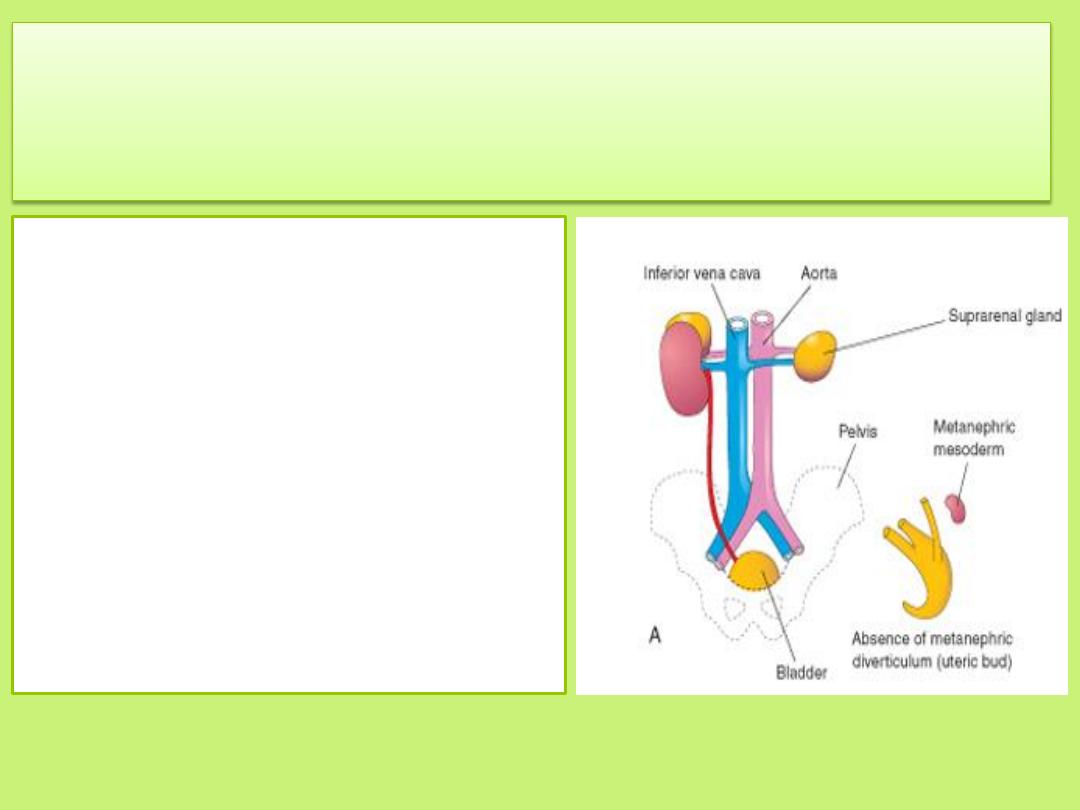
Renal agenesis
may arise if the interaction between the metanephric mesoderm and
the ureteric bud fails to occur
• Unilateral renal agenesis
often causes no symptoms
and is usually not discovered
during infancy because the
other kidney usually
undergoes compensatory
hypertrophy and performs
the function of the missing
kidney.
• Unilateral renal agenesis
should be suspected in
infants with a single
umbilical artery
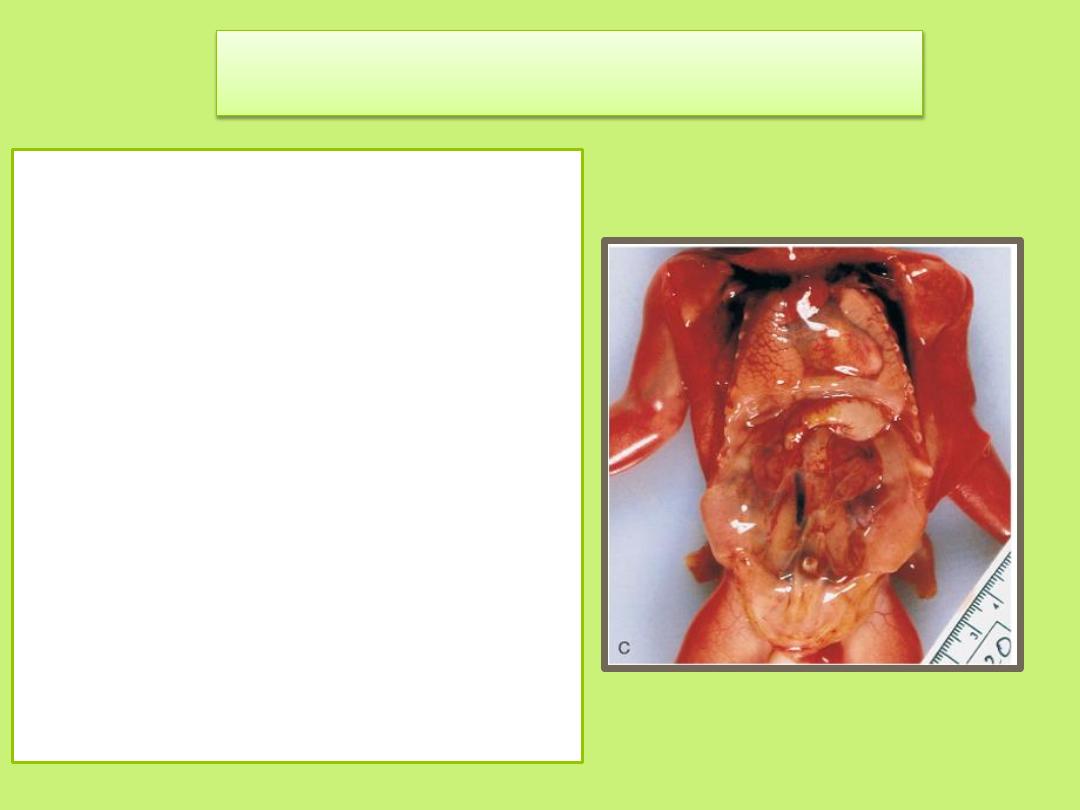
Bilateral renal agenesis
•
is associated with
oligohydramnios (small
amount of amniotic
fluid) because little or no
urine is excreted into the
amniotic cavity.
• Most infants with
bilateral renal agenesis
die shortly after birth or
during the first months
of life
.
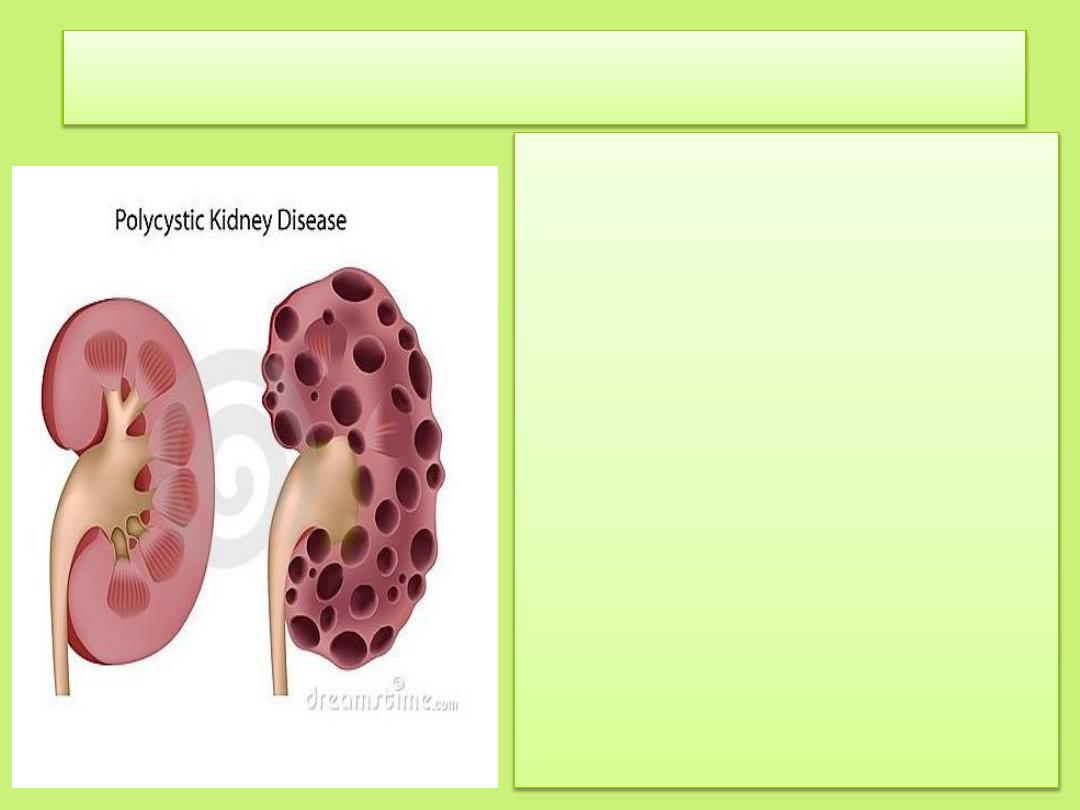
Congenital polycystic kidney disease
numerous cysts form.
Autosomal recessive polycystic
kidney disease is a progressive
disorder in which cysts form
from collecting ducts. The
kidneys become very large, and
renal failure occurs in infancy or
childhood.
Autosomal dominant polycystic
kidney disease ,cysts form from
all segments of the nephron and
usually do not cause renal failure
until adulthood. The autosomal
dominant disease is more
common but less progressive
than the autosomal recessive
disease .
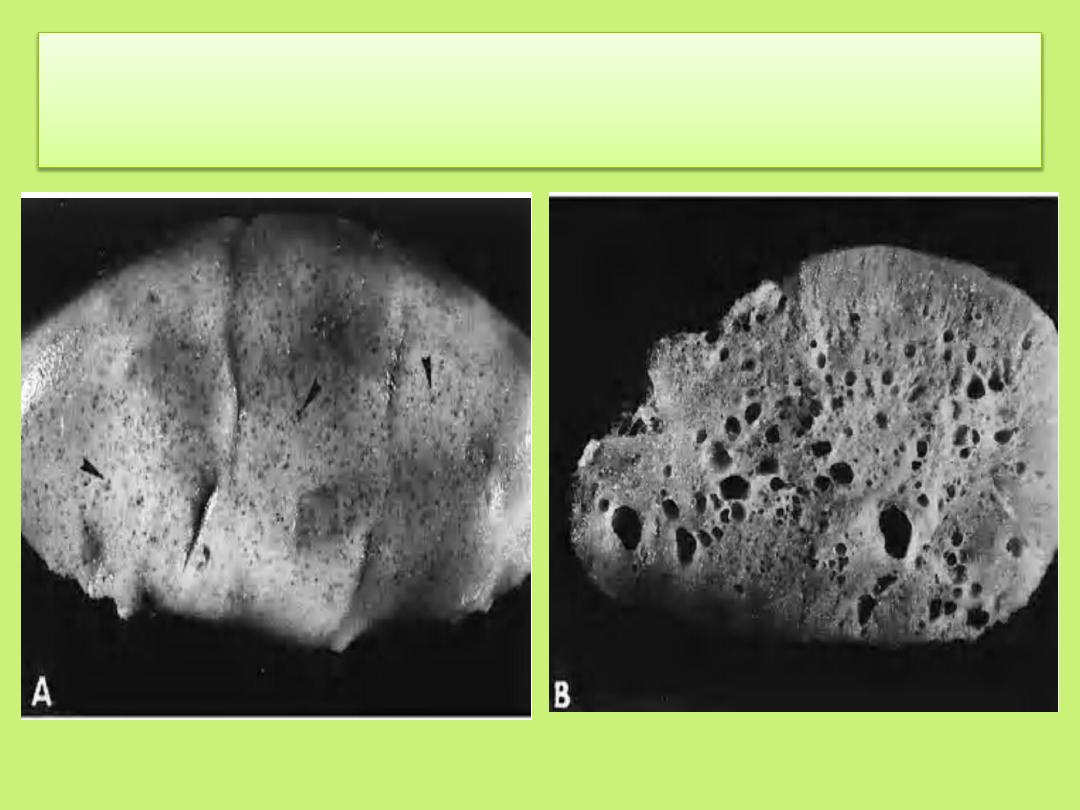
(A) Surface view of a fetal kidney with multiple cysts
(B) Section of the kidney in A, showing multiple cysts.
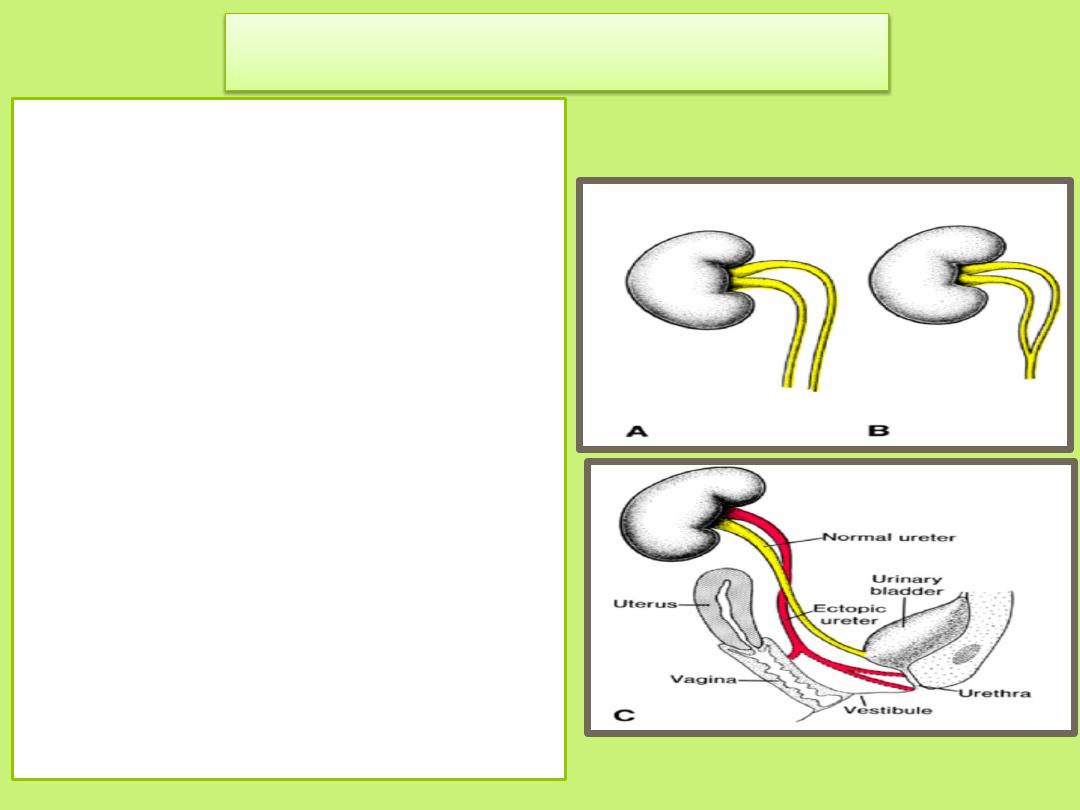
Duplication of the ureter
results from:
• early splitting of the ureteric
bud . Splitting may be partial or
complete, and metanephric
tissue may be divided into two
parts, each with its own renal
pelvis and ureter.
• In rare cases, one ureter opens
into the bladder, and the other
is ectopic, entering the vagina,
urethra, or vestibule .This
abnormality results from
development of two ureteric
buds. One of the buds usually
has a normal position, whereas
the abnormal bud moves down
together with the mesonephric
duct. Thus it has a low, abnormal
entrance in the bladder, urethra,
vagina, or epididymal region.
Position of the Kidney
• The kidney,
initially in the pelvic region
, later shifts to a more
cranial position in the abdomen.
• This ascent of the kidney is caused by:
1. diminution of body curvature
2. growth of the body in the lumbar and sacral regions
• The position of the kidneys becomes fixed once they come
into contact with the suprarenal glands in the 9
th
week
where they attain their adult position
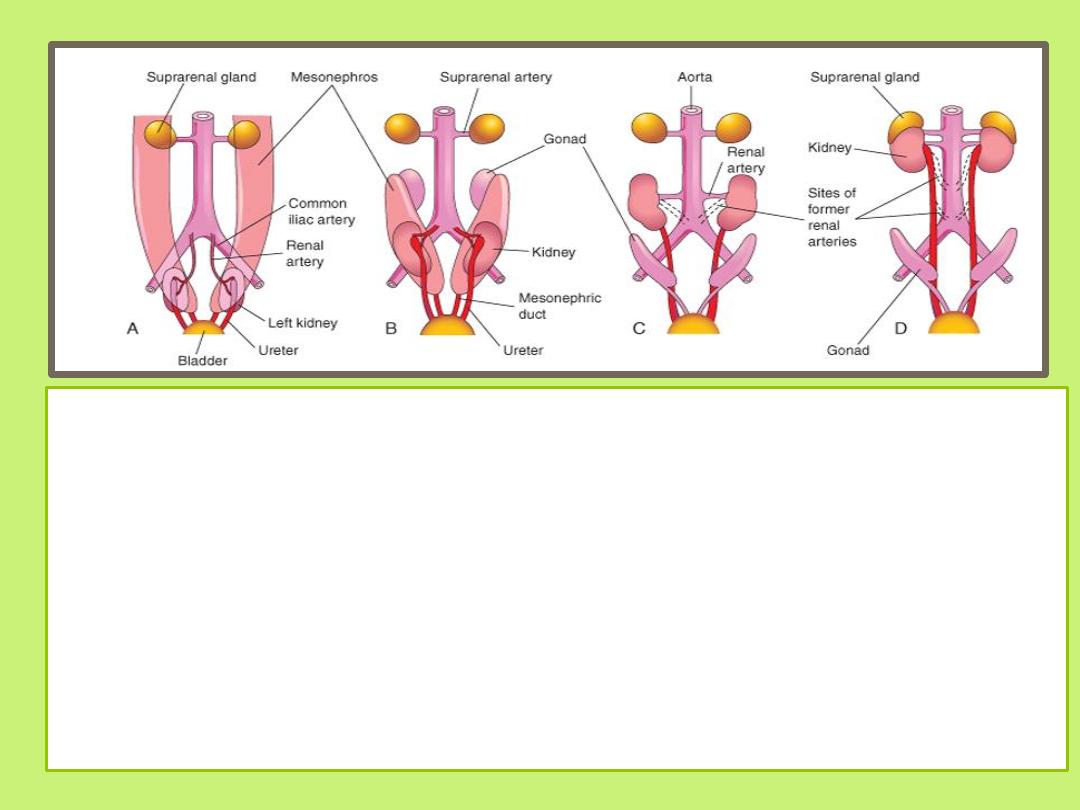
• In the pelvis, the metanephros receives its arterial supply from a pelvic branch
of the aorta.
• During its ascent to the abdominal level, it is vascularized by arteries that
originate from the aorta at continuously higher levels.
• The lower vessels usually degenerate, but some may remain.
• Initially the hilum of the kidney faces ventrally; however, as the kidney
relocates (ascends), it rotates medially almost 90 degrees. By the 9
th
week, the
hilum is directed anteromedially.
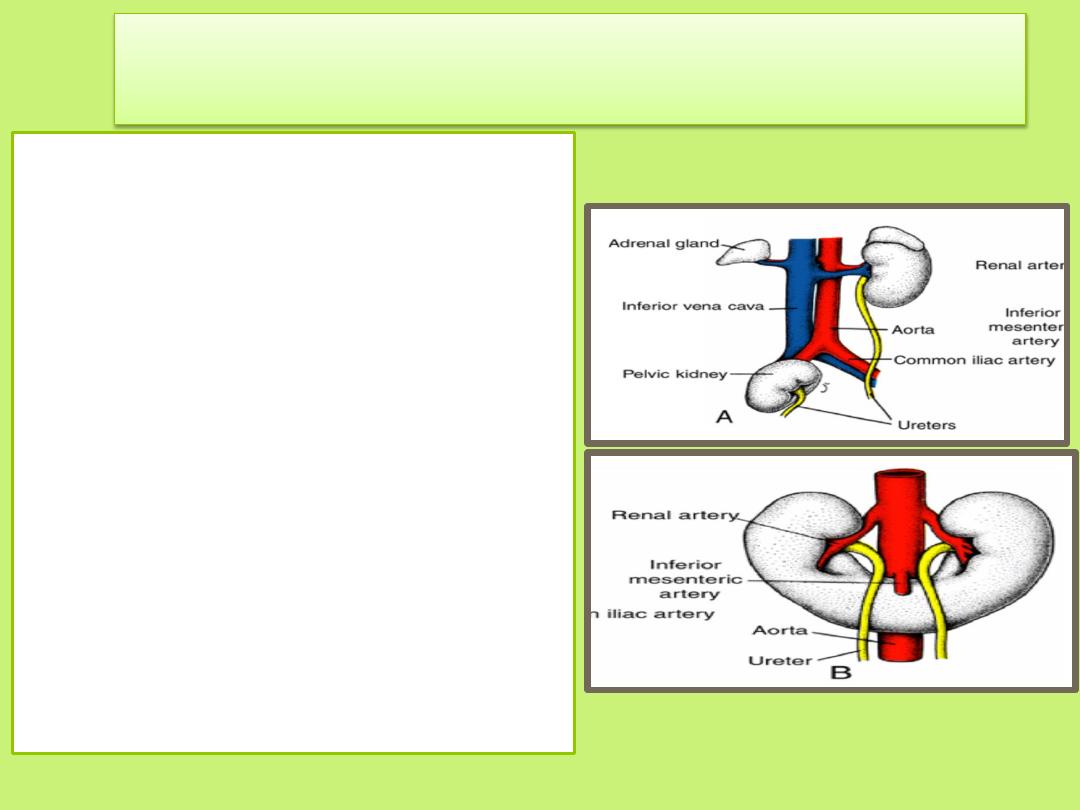
Abnormal Location of the Kidneys
• During their ascent, the kidneys
pass through the arterial fork
formed by the umbilical arteries,
but occasionally one of them fails
to do so. Remaining in the pelvis
close to the common iliac artery,
it is known as a pelvic kidney
• Sometimes the kidneys are
pushed so close together during
their passage through the arterial
fork that the lower poles fuse,
forming a horseshoe kidney . The
horseshoe kidney is usually at the
level of the lower lumbar
vertebrae, since its ascent is
prevented by the root of the
inferior mesenteric artery
Accessory renal arteries
• are common
• they derive from the persistence of embryonic
vessels that formed during ascent of the
kidneys.
• These arteries usually arise from the aorta and
enter the superior or inferior poles of the
kidneys
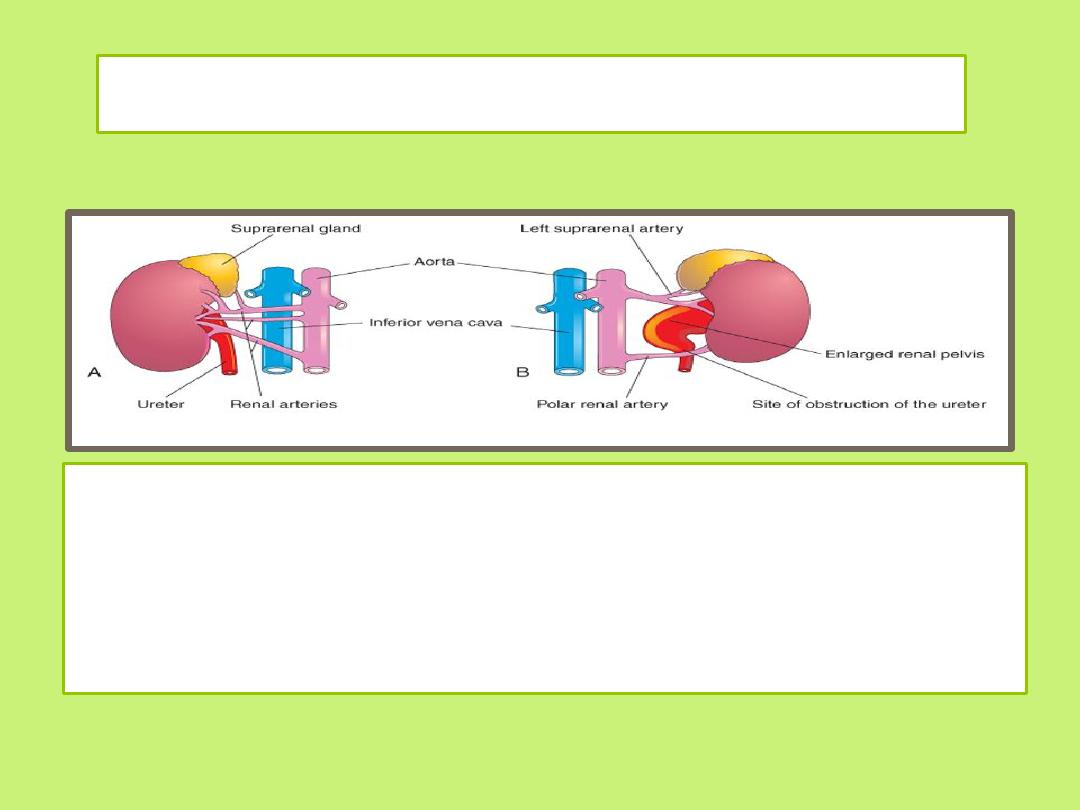
Common variations of renal vessels
• A and B, Multiple renal arteries.
• Note the accessory vessels entering the poles of the kidney.
• The polar renal artery, illustrated in B, has obstructed the ureter
and produced an enlarged renal pelvis.
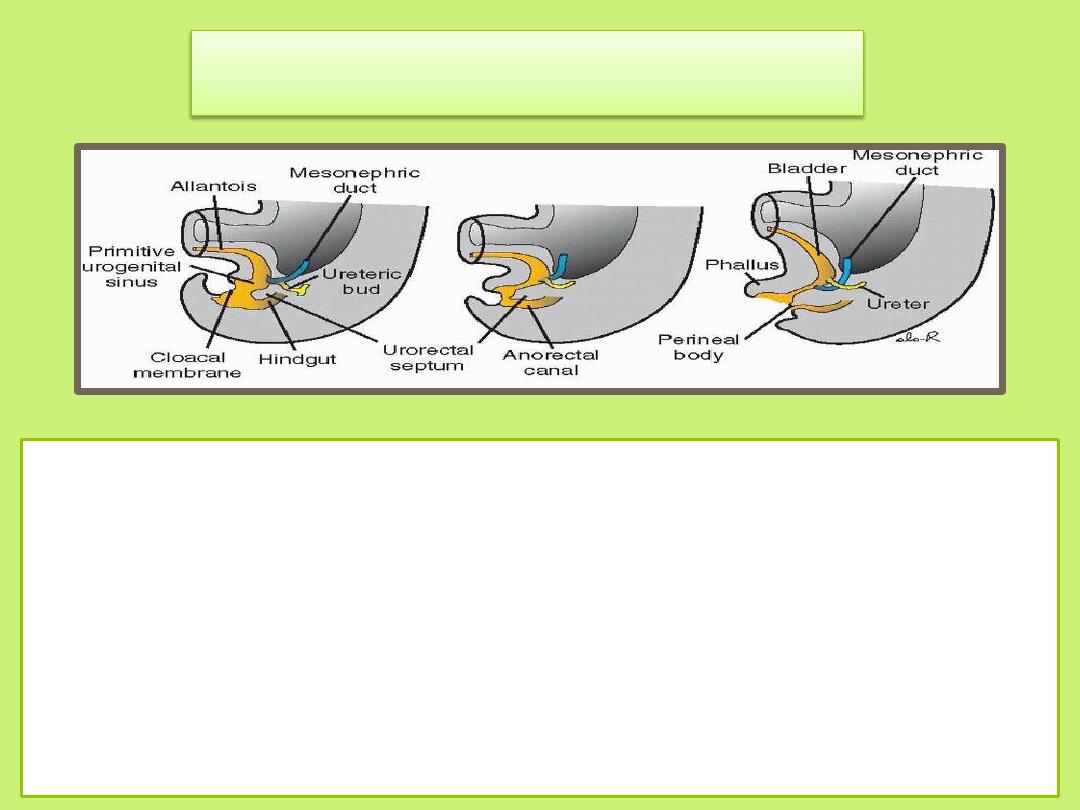
Bladder and Urethra
• During the 4
th
-7
th
week of development, the Cloaca
divides into the urogenital sinus anteriorly and the anal
canal posteriorly .
• The Urorectal septum is a layer of mesoderm between
the primitive anal canal and the urogenital sinus. The tip
of the septum will form the perineal body .
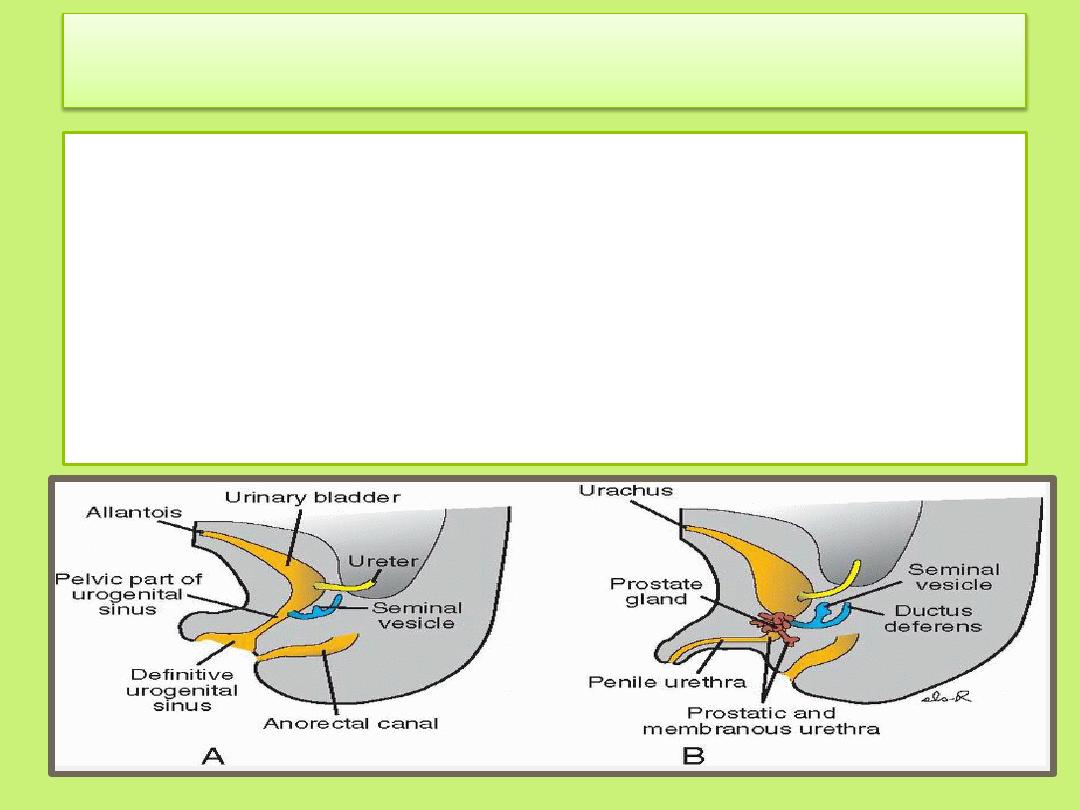
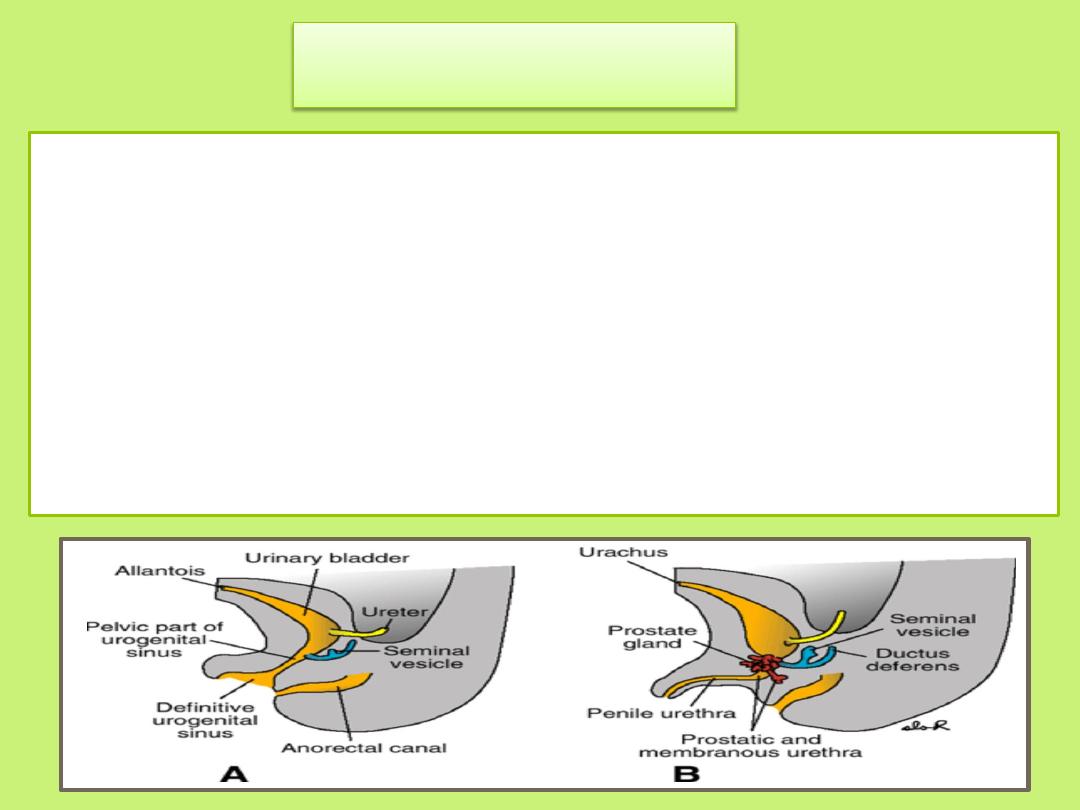
Three portions of the urogenital sinus can be distinguished
the upper part ( the urinary bladder)
Is the largest part.
Initially, the bladder is continuous with the allantois
when the lumen of the allantois is obliterated, a thick fibrous
cord, the Urachus, remains and connects the apex of the
bladder with the umbilicus . In the adult, it is known as the
median umbilical ligament.
The next part is
the pelvic part of the urogenital sinus
is a rather narrow canal
in the male , it gives rise to the prostatic and
membranous parts of the urethra
.
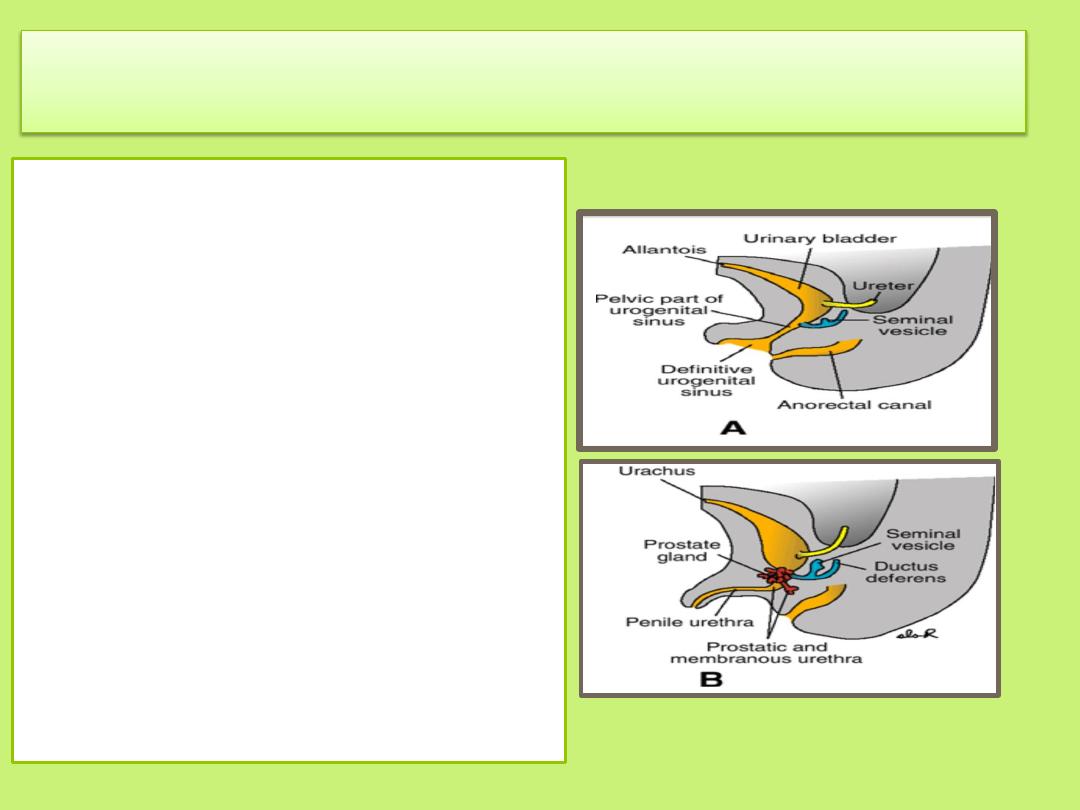
The last part is
the phallic part of the
urogenital sinus
It is flattened from side to
side, and as the genital
tubercle grows, this part of
the sinus will be pulled
ventrally .
Development of the phallic
part of the urogenital sinus
differs greatly between the
two sexes.)
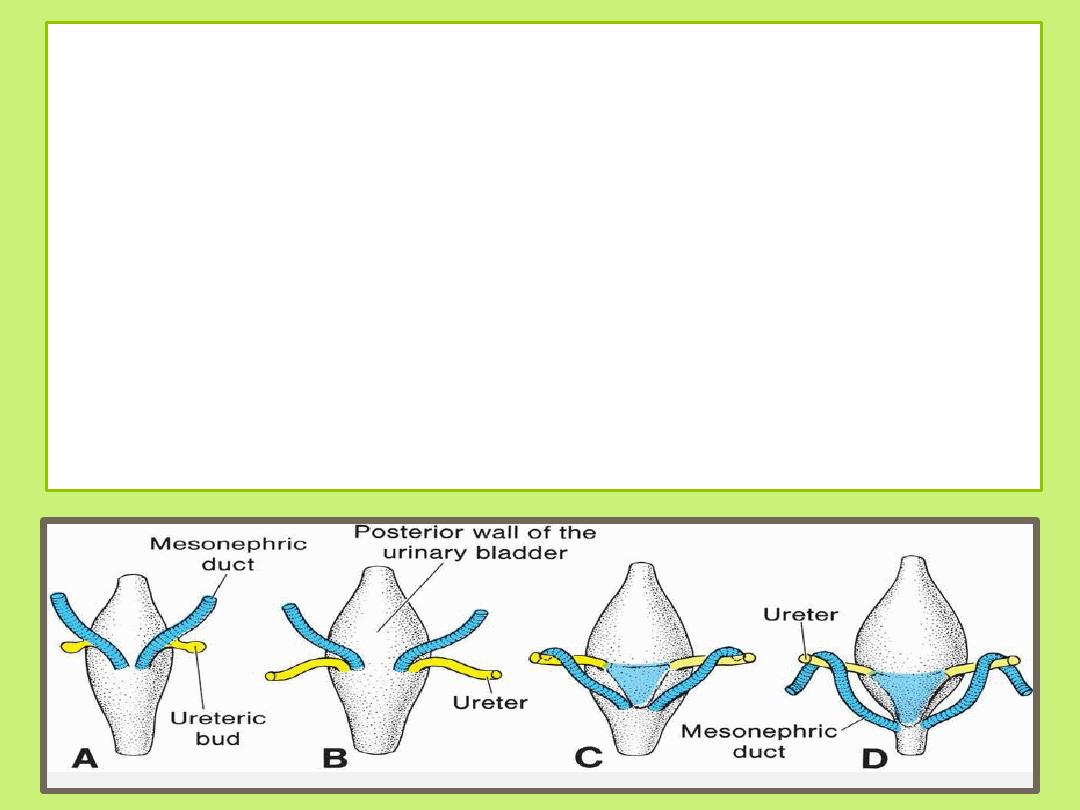
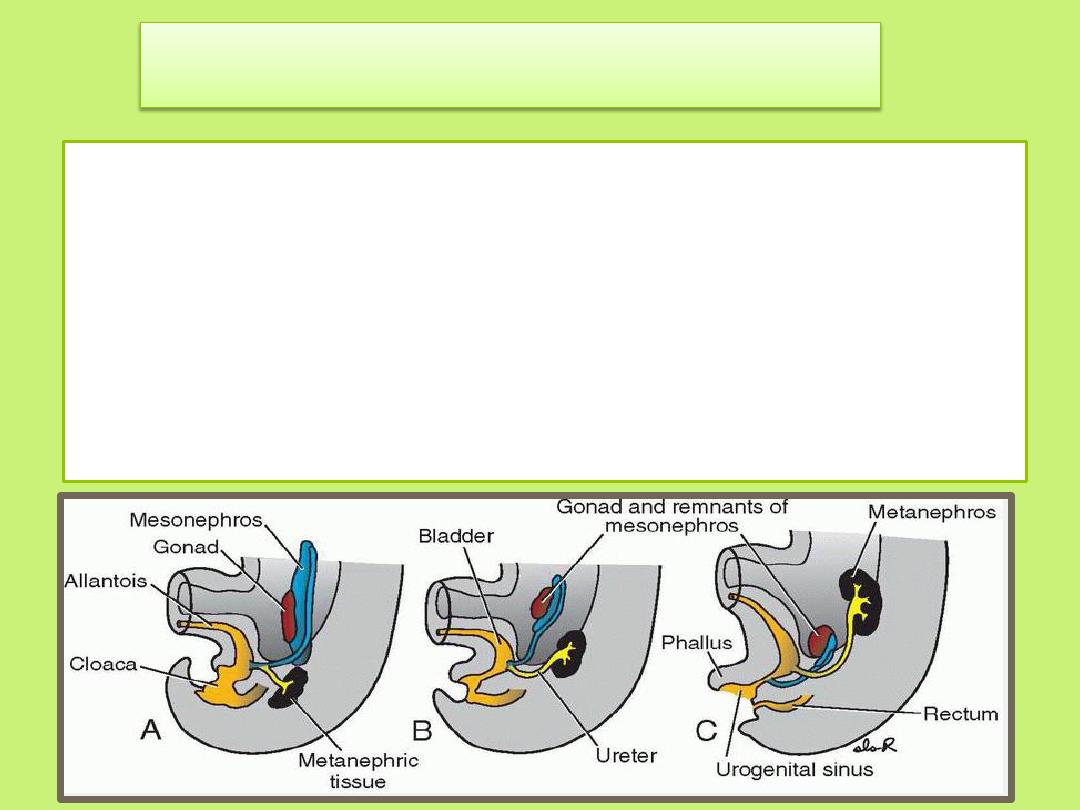
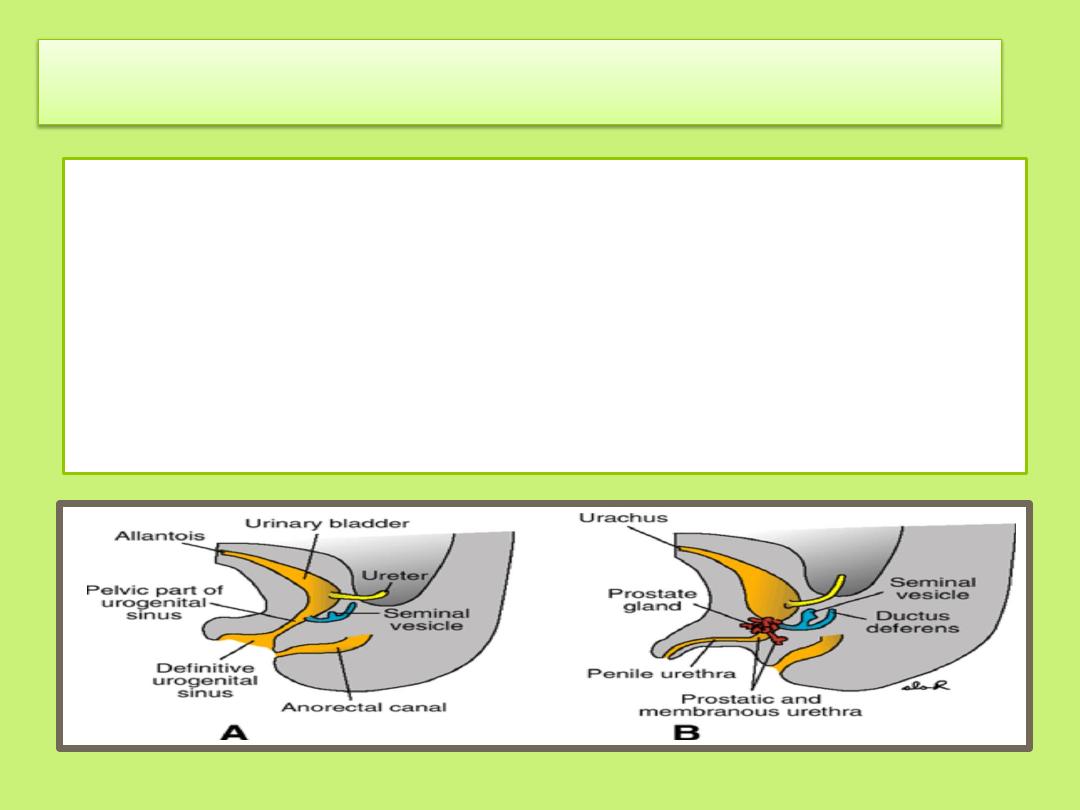
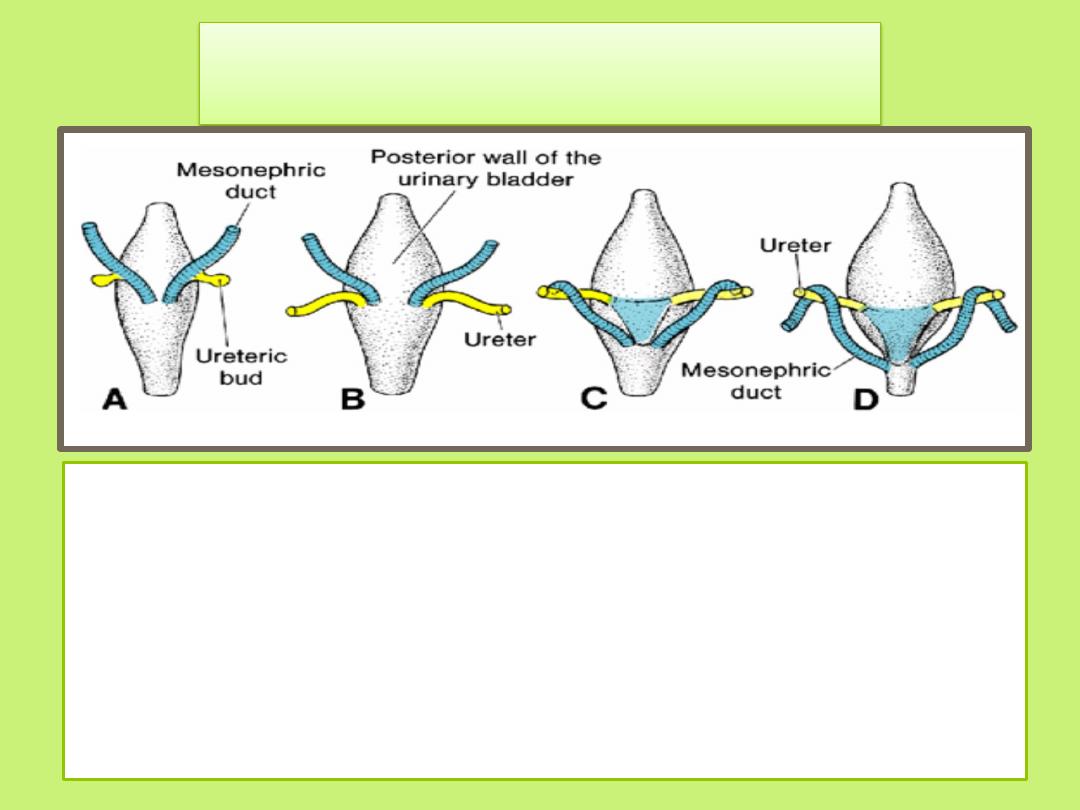
During differentiation of the cloaca, the caudal portions of the
mesonephric ducts are absorbed into the wall of the urinary
bladder
As a result of ascent of the kidneys,
the orifices of the ureters move farther cranially;
those of the mesonephric ducts move close together to enter
the prostatic urethra and in the male become the ejaculatory
ducts
Trigone of the bladder
• Since both the mesonephric ducts and ureters originate in
the mesoderm, the mucosa of the bladder formed by
incorporation of the ducts (the trigone of the bladder) is also
mesodermal.
• With time, the mesodermal lining of the trigone is replaced
by endodermal epithelium, so that finally the inside of the
bladder is completely lined with endodermal epithelium
.
• In infants and children, the urinary bladder,
even when empty, is in the abdomen.
• It begins to enter the greater pelvis at
approximately 6 years of age, but it does not
enter the lesser pelvis and become a pelvic
organ until after puberty.
Urethra
• The epithelium of the urethra in both sexes originates in the
endoderm;
• the surrounding connective and smooth muscle tissue is derived
from splanchnic mesoderm.
• At the end of the third month, epithelium of the prostatic urethra
begins to proliferate and forms a number of outgrowths that
penetrate the surrounding mesenchyme.
• In the male, these buds form the prostate gland.
• In the female, the cranial part of the urethra gives rise to the
urethral and para-urethral glands.
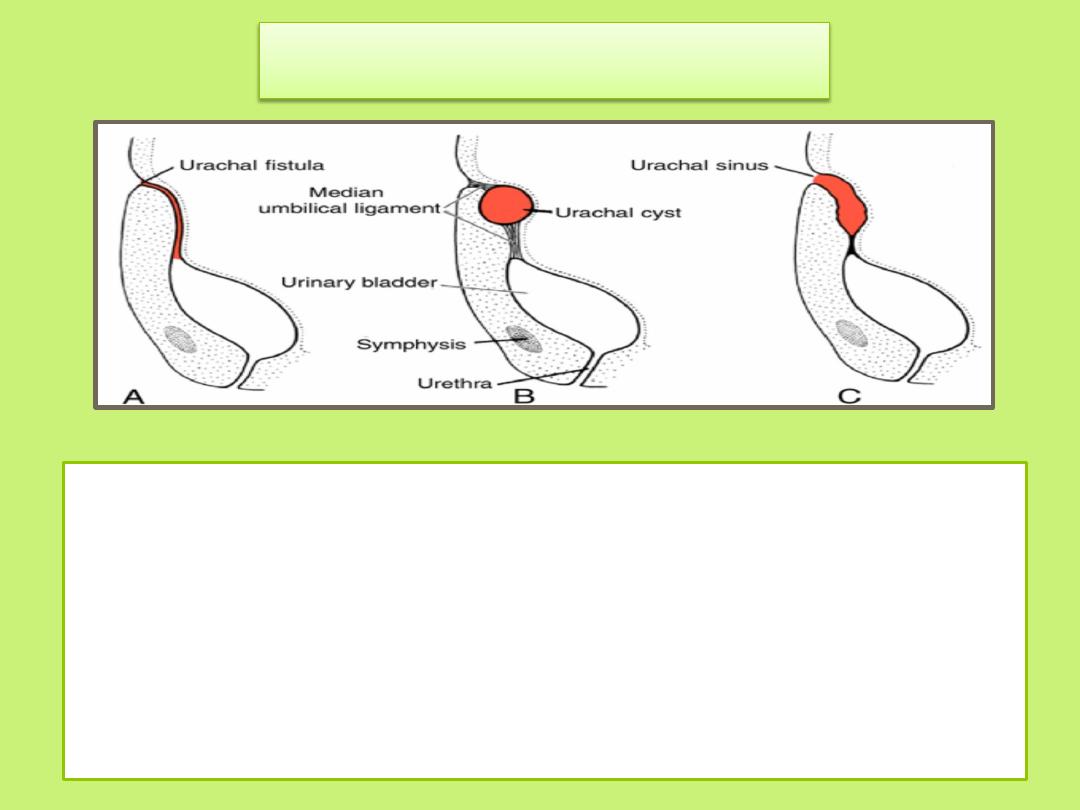
Bladder Defects
A: Urachal fistula occurs when the lumen of the
intraembryonic portion of the allantois persists . It may cause
urine to drain from the umbilicus
B:Urachal cyst If only a local area of the allantois persists,
secretory activity of its lining results in a cystic dilation
C: Urachal sinus occurs when the lumen in the upper part
persists
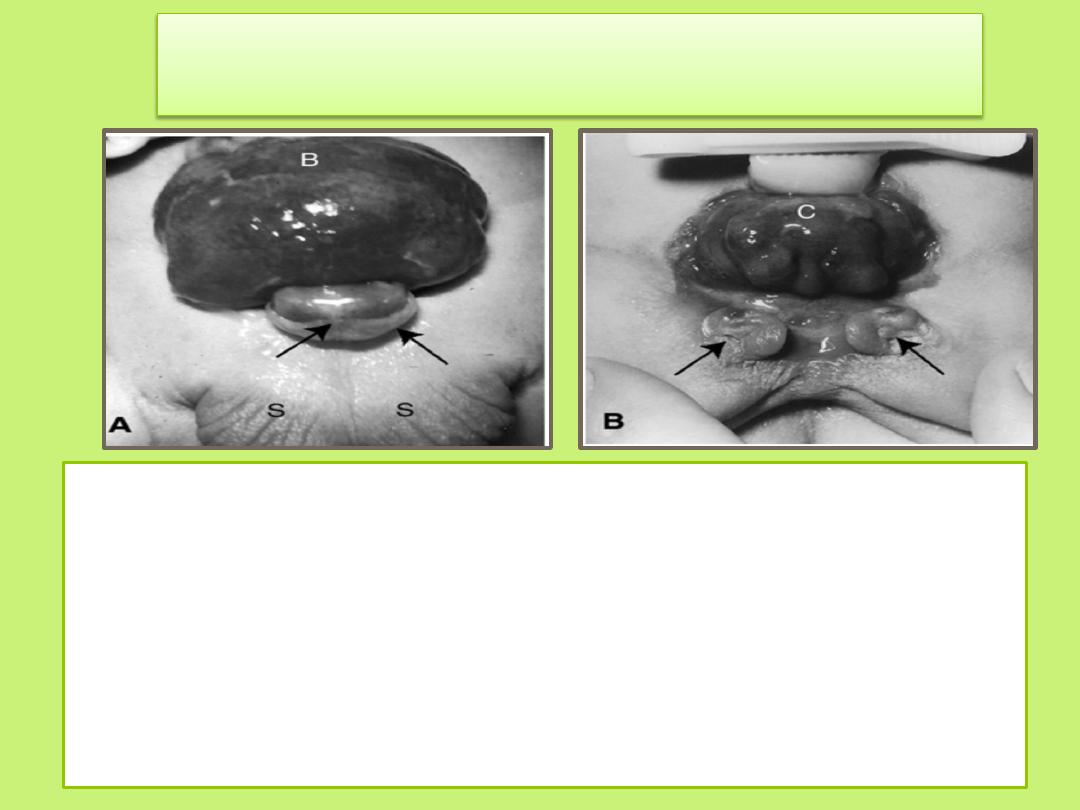
Exstrophy of the bladder
• is a ventral body wall defect in which the bladder mucosa is
exposed.
• Epispadias is a constant feature
• Exstrophy of the bladder may be caused by a lack of
mesodermal migration into the region between the umbilicus
and genital tubercle, followed by rupture of the thin layer of
ectoderm.
Summary
Embryologically and anatomically, both urinary and genital systems
are intimately interwoven. Both systems are derived from
intermediate mesoderm and their excretory ducts enter the
cloaca.
Three kinds of kidney systems appear during intrauterine life
pronephros: rudimentary and nonfunctional
mesonephros : may function for a short time during the early fetal
period
metanephros: forms the permanent kidney.
the kidney develops from two sources:
Metanephric mesoderm, which provides excretory units
Ureteric bud, which gives rise to the collecting system.
The upper part of urogenital sinus distinguished into urinary
bladder
The pelvic part of urogenital sinus gives rise to the prostatic and
membranous parts of the urethra.
The phallic part of the urogenital sinus differs greatly between the
two sexes
Thank you
Next Lecture: Genital system