Dr.Maan Alkhalisy Embryology lec. 9 & 10
1
Digestive system
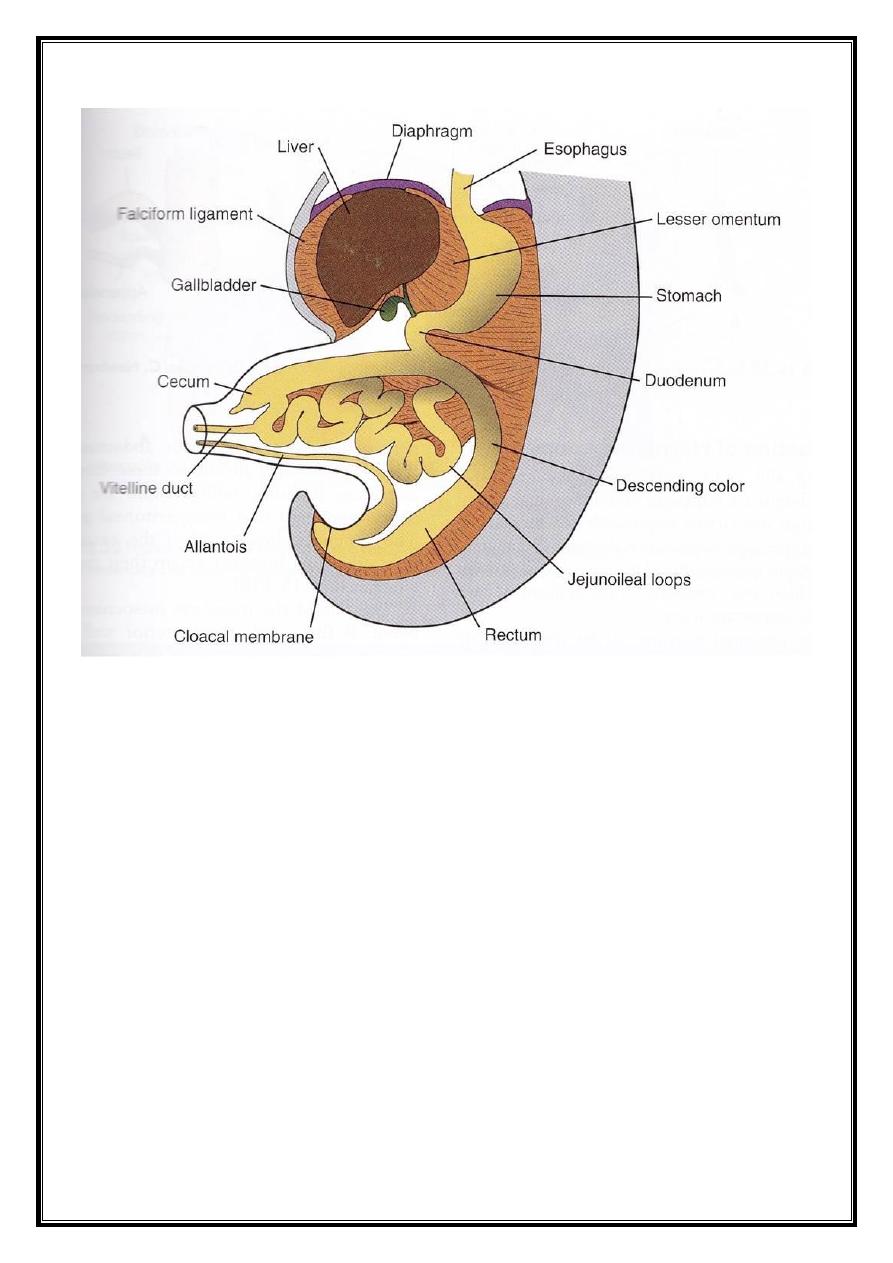
In the cephalic and caudal part of the embryo, the primitive
gut forms a blind-ending tube, the foregut and the hindgut. The
midgut remains connected to the yolk sac by the vitelline duct, or
the yolk stalk.
We can divide the G.I.T. according to its developmental
point of view into :-
1- The pharyngeal gut : extends from the oro-pharyngeal
membrane to the respiratory diverticulum. This is considered as a
part of the foregut.
2- The remainder of the foregut lies caudal to the previous part,
and extends to the liver outgrowth.
3- The midgut : begins caudal to the previous part and extends to
the junction of the right 2/3 and left 1/3 of the transverse colon.
4- The hindgut : extends from the left 1/3 of the transverse colon
to the cloacal membrane.
Dr.Maan Alkhalisy Embryology lec. 9 & 10
2
The endoderm forms the epithelial lining of the digestive
system, and gives rise to the specific cells (the parenchyma) of
glands, like the liver, pancreas, and other glands. While the stroma
of the glands, and the muscle, connective tissue, and peritoneal
components of the wall of the gut are derived from the visceral
mesoderm.
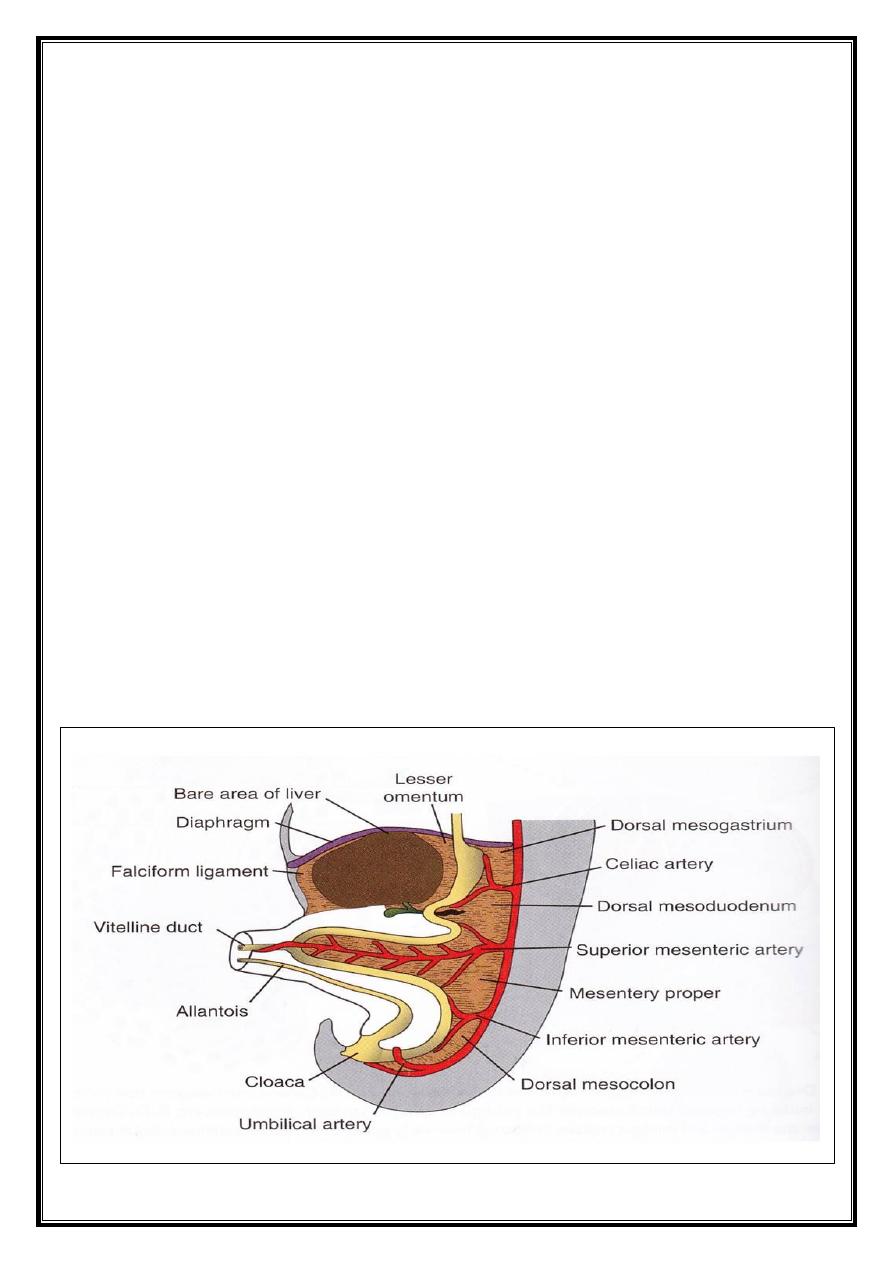
ــ Mesenteries :
Portions of the gut and its derivatives are suspended from
the dorsal and ventral mesenteries. This mesentery consists of 2
layers of peritoneum o enclose an organ of viscera. These parts of
the viscera are called intra-peritoneal organs, while any part that
has a sheath of peritoneum covering its anterior surface only, and
plastering it to the posterior abdominal wall, is called a retro-
peritoneal organ.
At the 5
th
week, the connecting tissue bridge has narrowed
and the caudal part of the foregut, the midgut, and a major part of
the hindgut are suspended from the abdominal wall by the dorsal
mesentery.
Ventral mesentery, which exists only in the region of the
terminal part of the oesophagus, the stomach, and the upper part
of the duodenum, is derived from the septum transversum.
Growth of the liver into the mesenchyme of the septum
transversum divides the ventral mesentery into:
a- the lesser omentum (gastro-hepatic omentum).
b- the falciform ligament which extends from the liver to the
ventral body wall.
Dr.Maan Alkhalisy Embryology lec. 9 & 10
3
ــ Foregut :
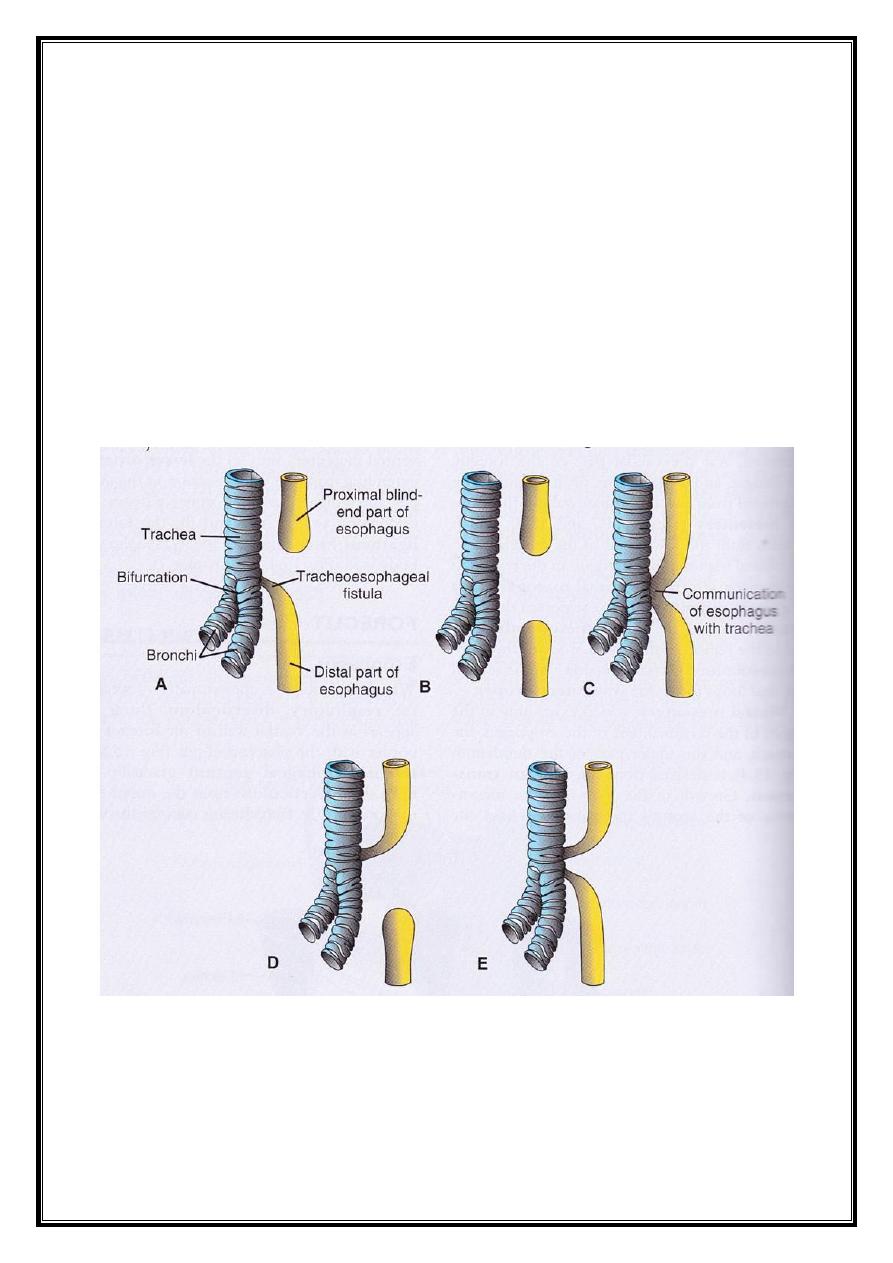
- Oesophagus :
At the 4
th
week of development, the lung bud appears from
the foregut. During this time, the trachea-oesophageal septum
gradually separates the oesophagus posteriorly (dorsal) from the
trachea anteriorly (ventral).
At first, the oesophagus is short, but with the development
of the heart and lung, the trachea and oesophagus descend
downward, so the oesophagus is lengthened.
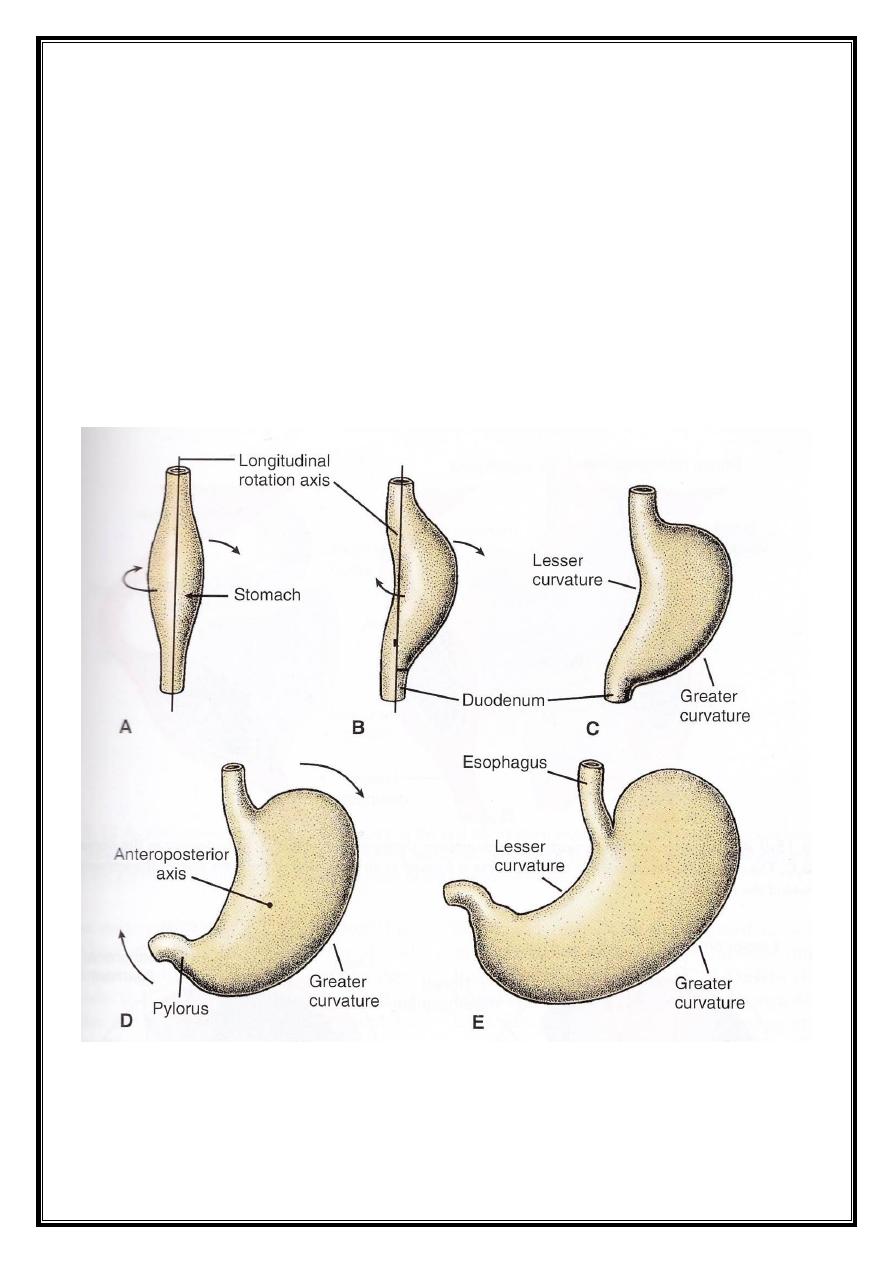
- Stomach :
It appears as a fusiform dilation in the 4
th
week of
Dr.Maan Alkhalisy Embryology lec. 9 & 10
4
development. This primitive shape of the stomach differs
gradually after the rotation and expansion of various parts of it.
The stomach rotates 90
o
clockwise around its longitudinal
axis, causing its left side to face anteriorly, and the right side to
face posteriorly. Accordingly, the right and left vagal trunks
become anterior and posterior vagal trunks.
The growth of the posterior wall of the stomach is much
greater than that of the anterior wall, leading to the formation of
the greater and lesser curvatures of the stomach.
Another rotation around the antero-posterior axis, the
pyloric region moves to the right side and the fundus moves to
the left side. With the enlargement of the stomach, the fundus
becomes large in size, and the same occurs to the pyloric region
(to a lesser extent).
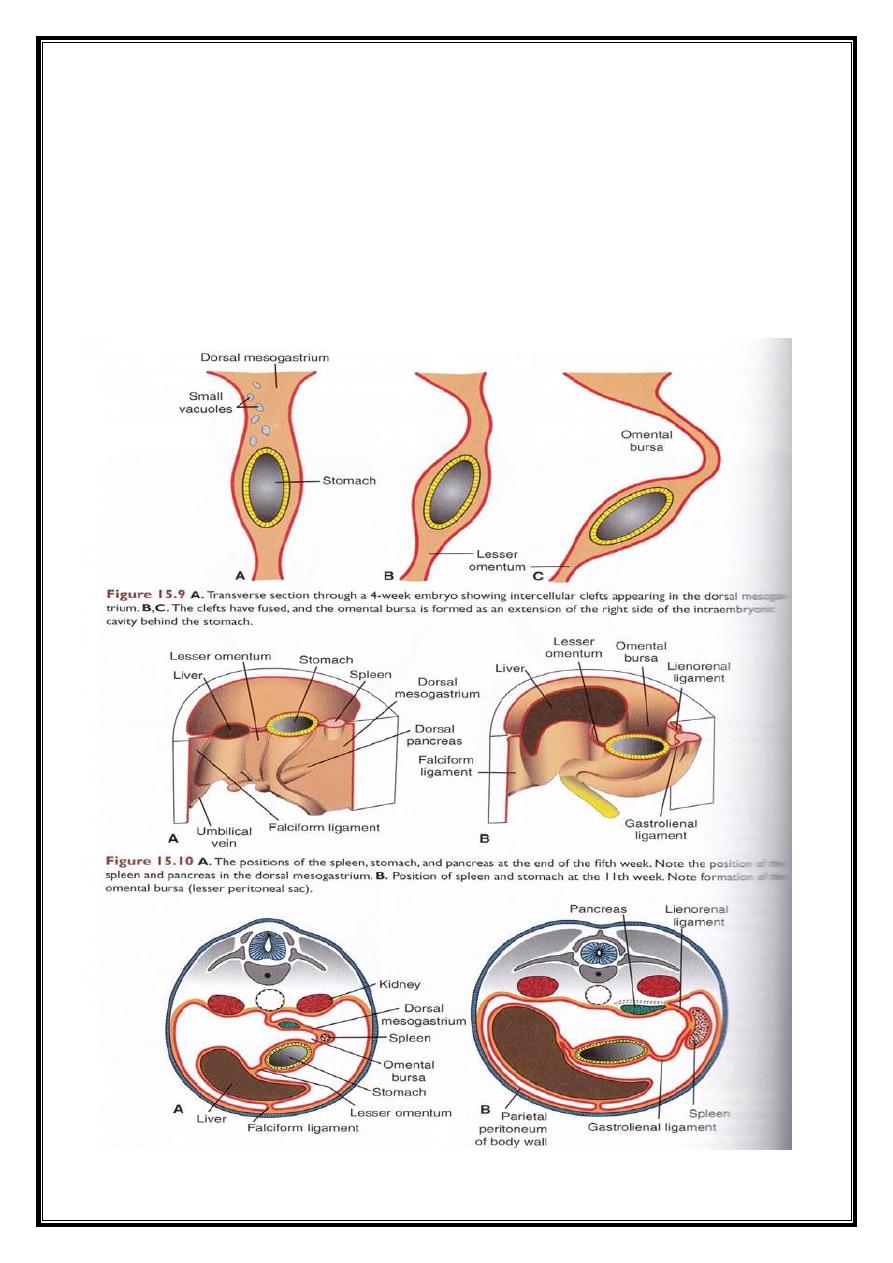
As a result of this rotation, the dorsal mesentery of the
leaving a space ehind the stomach called the omental bursa. With
this rotation, the peritoneum surrounds the spleen completely to
remain intraperitoneal. From the spleen, the lienorenal ligament
arises, connecting the spleen with the left kidney, and the
gastrosplenic ligament, which connects the spleen to the
stomach.
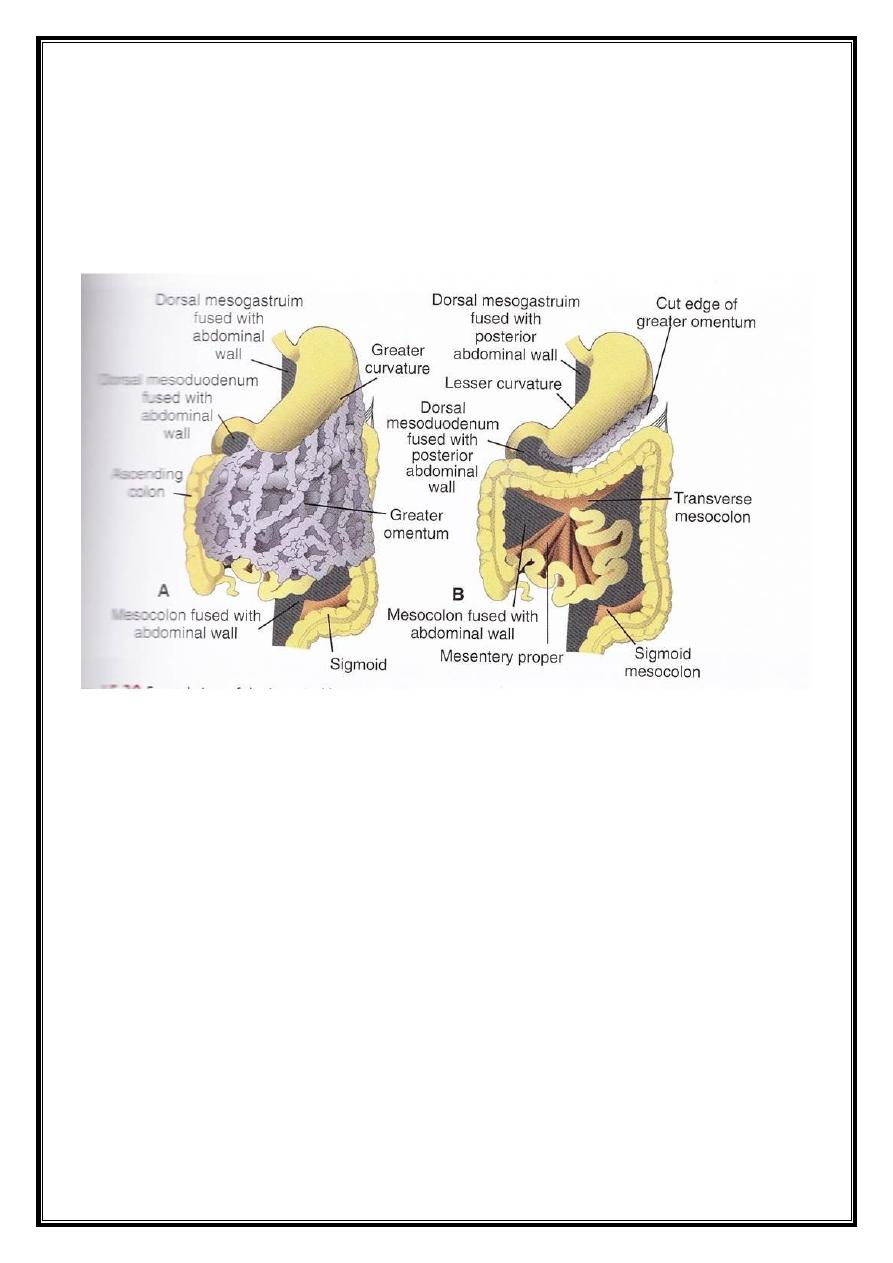
As a result of the rotation of the stomach, the dorsal
mesentery of the stomach bulges and continues to grow down
forming a double-layered sac extending over the transverse colon
and small intestine like an apron, this is called the greater
omentum. Later, the two layers of this apron will fuse forming a
single sheet hanging from the greater curvature of the stomach.
The posterior layer of the greater omentum also fuses with the
mensentery of the transverse colon.
Dr.Maan Alkhalisy Embryology lec. 9 & 10
5
The lesser omentum and falciform ligament form from the
ventral mesentery of the stomach (ventral mesogastrium), which
itself is derived from the mesoderm of the septum transversum.
When the liver grows into the septum, it thins to form :
a- the peritoneum of the liver.
b- the falciform ligament, extending from the liver to the anterio
body wall.
c- the lesser omentum, extending from the liver to the lesser
curvature of the stomach and the upper duodenum (1
st
inch)
The free margin of the falciform ligament contains the
umbilical vein, which is obliterated after birth to form ligamentum
teres (the round ligament of the liver).
Dr.Maan Alkhalisy Embryology lec. 9 & 10
6
The free edge of the lesser omentum connecting the liver to
the duodenum (hepatoduodenal ligament) will contain the portal
vein posteriorly, the bile duct anteriorly to the right side, and the
hepatic artery anteriorly to the left side (the portal triad). This free
edge also forms the roof of the epiploic foramen of Winslow,
which is the only connection between the lesser sac (omental
bursa) and the greater sac (the rest of the peritoneal cavity).
Dr.Maan Alkhalisy Embryology lec. 9 & 10
7
- Duodenum :
The landmark between the foregut and midgut is the
duodenum.
As the stomach rotates, the duodenum takes the form of a
C-shaped loop, and rotates to the right.
As a result of this rotation, and the enlargement of the
duodenum and pancreas, the duodenum becomes fixed in the
right side, and the head of pancreas develops in the concavity of
the duodenum. The duodenum and the head of pancreas will be
plastered to the posterior abdominal wall and become retro-
peritoneal, except for the 1
st
inch of the first part of the
duodenum.
The coeliac artery is the artery of the foregut, while the
superior mesenteric artery provides the blood supply to the
midgut.
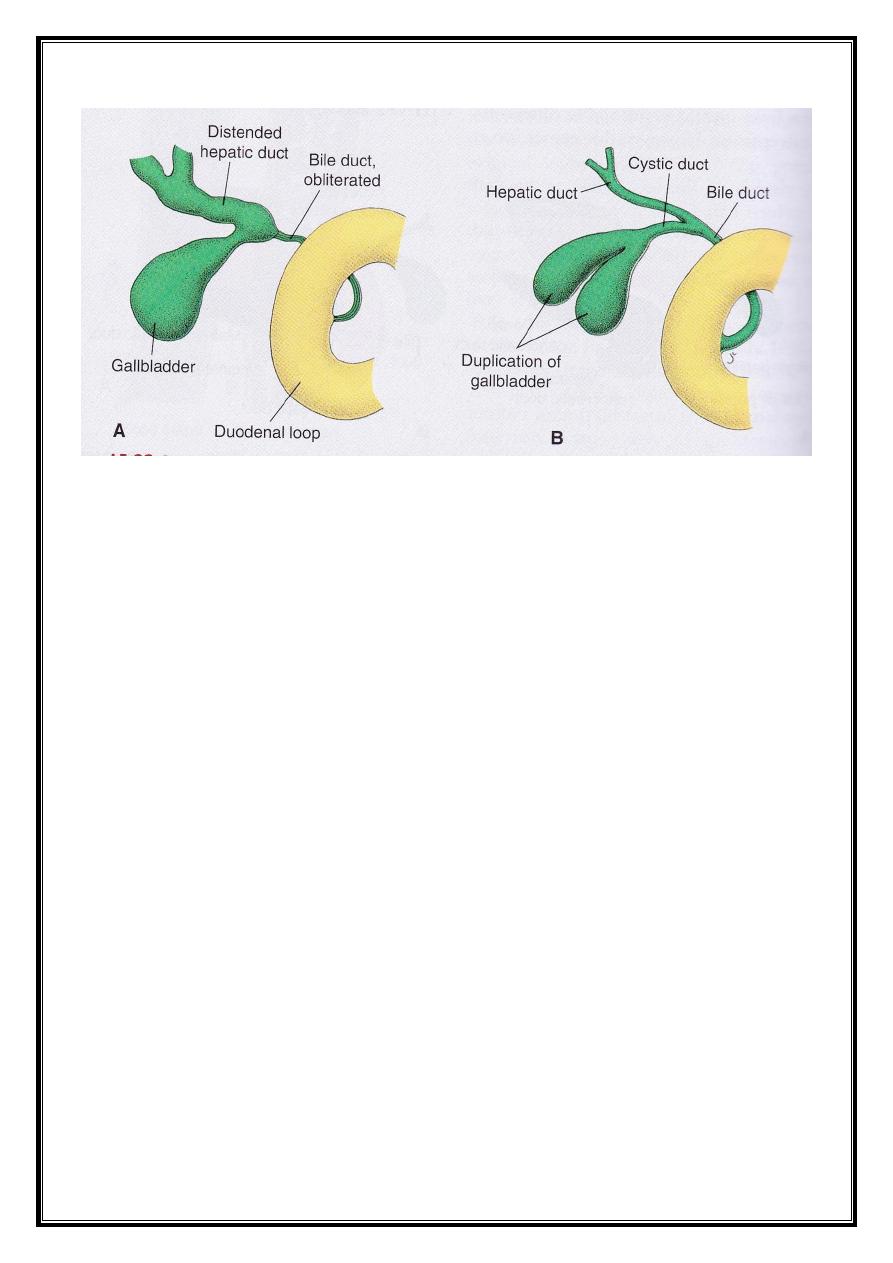
- Liver and gall bladder :
The liver primordium appears in the middle of the 3
rd
week
as an outgrowth of the endodermal epithelium at the distal part
of the foregut.
The live bud consists of rapidly proliferating cells that
penetrates the septum transversum.
The connection between the liver and the second part of the
duodenum narrows, forming the bile duct. An outgrowth from the
bile duct will form the gall bladder and the cystic duct.
As the liver cells have invaded the septum transversum, so
the liver bulges caudally into the abdominal cavity.
The mesoderm surrounding the liver differentiates into
visceral peritoneum except on its cranial surface which remains
uncovered (the bare area of the liver), where the liver is in close
contact with the central tendon of the diaphragm.
Dr.Maan Alkhalisy Embryology lec. 9 & 10
8
In the 10
th
week of development, the weight of the liver is
approximately 10% of the total body weight. The liver here has a
hematopoietic function.
In the 12
th
week of development, the liver begins to produe
bile, and when the biliary system is completely developed, the bile
will enter the gastro-intestinal tract.
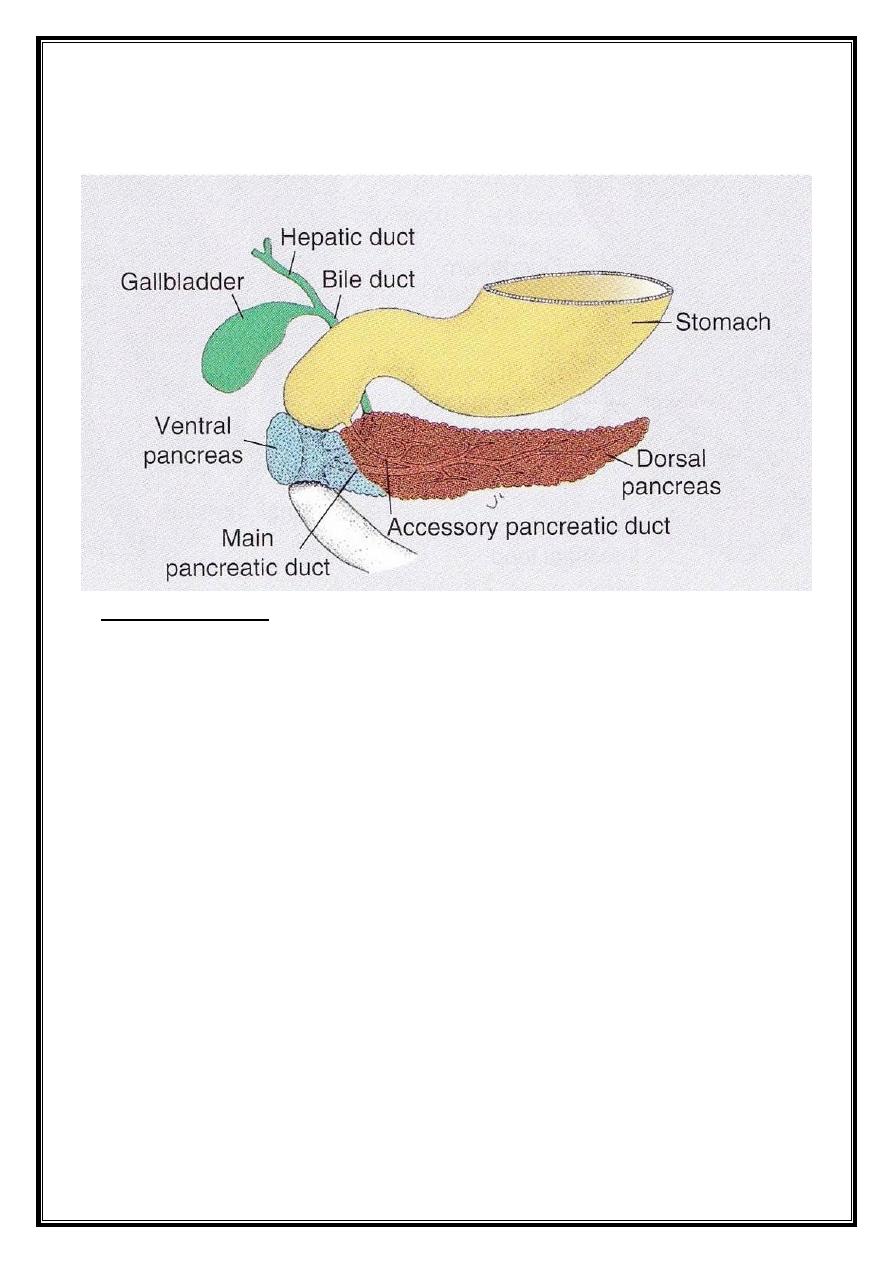
- Pancreas :
The pancreas is formed by two buds, a ventral and a dorsal
one, originating from the endothelial lining of the duodenum.
The ventral bud will form the uncinated process and the
inferior part of the head of pancreas, while the remaining part is
formed by the dorsal bud.
During the movement and rotation of the duodenum and
pancreas, the pancreas takes its own position (i.e. the head is
located in the concavity of the duodenum, and the remaining part
continues in its position as in the adult).
The pancreas opens together with the common bile duct
into the medial part of the duodenum.
Dr.Maan Alkhalisy Embryology lec. 9 & 10
9
In the 3
rd
month of foetal life, the pancreatic islets will be
formed, and by the 5
th
month, the insulin secretion begins.
* CLINICAL NOTE : any defect in the rotation of the pancreatic
parts will form the annular pancreas, in which the pancreas is a
circular structure around the duodenum, leading to a constriction
or narrowing of duodenal lumen.
ــ Midgut :
In the 5
th
week of development, the midgut has a short
dorsal mesentery, and is connected to the yolk sac by the vitelline
duct (yolk stalk) anteriorly. All the midgut is supplied by the
superior mesenteric artery.
The development of the midgut is characterized by the rapid
elongation of the gut forming the primary intestinal loop.
The cephalic limb of this loop develops to complete the
duodenum, jejunum, and ileum, while the caudal limb of this loop
will form the distal part of the ileum, the cecum, the appendix, the
ascending colon, and the proximal 2/3 of the transverse colon.
Dr.Maan Alkhalisy Embryology lec. 9 & 10
10
Physiological hernia :
The development of the primary intestinal loop is
characterized by rapid elongation, particularly of the cephalic
limb. As a result of the rapid growth and expansion of the liver,
the abdominal cavity temporarily becomes too small to contain all
the intestinal loops, so they enter the extra-embryonic cavity in
the umbilical cord during the 6
th
week of development
(physiological umbilical herniation).
Rotation of the midgut :
The primary intestinal loop rotates around an axis formed by
the superior mesenteric artery in counter-clockwise. This rotation
is about 270
o
. During the herniation, it rotates 90
o
, as well as
Dr.Maan Alkhalisy Embryology lec. 9 & 10
11
during the return of this loops inside the abdominal cavity (it
completes the remaining 180
o
of rotation).
Retraction of the herniated loops :
During the 10
th
week of development, the herniated loops
begin to return to the abdominal cavity. The cause behind this
return could be due to the presence of a space for the intestinal
loop after the regression of the mesonephric kidney, reduced
growth of the liver, and the expansion of the abdominal cavity.
The first part that starts to return back to the cavity is the
proximal portion of the jejunum, and it comes to lie on the left
side, while the last part that re-enters the abdominal cavity is the
cecal bud which appears at about the 6
th
week as a small conical
dilation of the caudal limb of the primary intestinal loop.
Temporarily, it lies in the right upper quadrant directly below the
right lobe of the liver. Form here, it descends into the right iliac
fossa, placing the ascending colon and the hepatic flexure on the
right side of the abdominal cavity. During this process, the distal
end of the cecal bud forms a narrow diverticulum, the appendix.
Mesentery of the intestinal loop :
The mesentery of the primary intestinal loop, the mesentery
proper, will undergo a lot of changes during the coiling and
rotation, till the dorsal mesentery presses against the posterior
abdominal wall. The net results are that the ascending and
descending colon will be plastered on the posterior abdominal
wall, while the mesentery of the transverse colon will be attached
to the posterior abdominal wall as the transverse mesocolon
which extends from the splenic flexure to the hepatic flexure.
Dr.Maan Alkhalisy Embryology lec. 9 & 10
12
The mesentery of the jejunum and ileum will be attached to
the posterior abdominal wall, taking an oblique line from the left
side, going downward to the right side.
ــ Hindgut :
Here the distal 1/3 of the transverse colon will have the
transverse mesocolon. The descending colon is plastered to the
posterior abdominal wall. The sigmoid colon gets its own
mesentery that is attached to the posterior abdominal wall.
The terminal portion of the hindgut enters the posterior
region of the cloaca (primitive anorectal canal), and the allantois
enters the anterior portion (primitive urogenital sinus).
There is a layer of mesoderm, the urorectal septum,
separates the region between the allantois and the hindgut. With
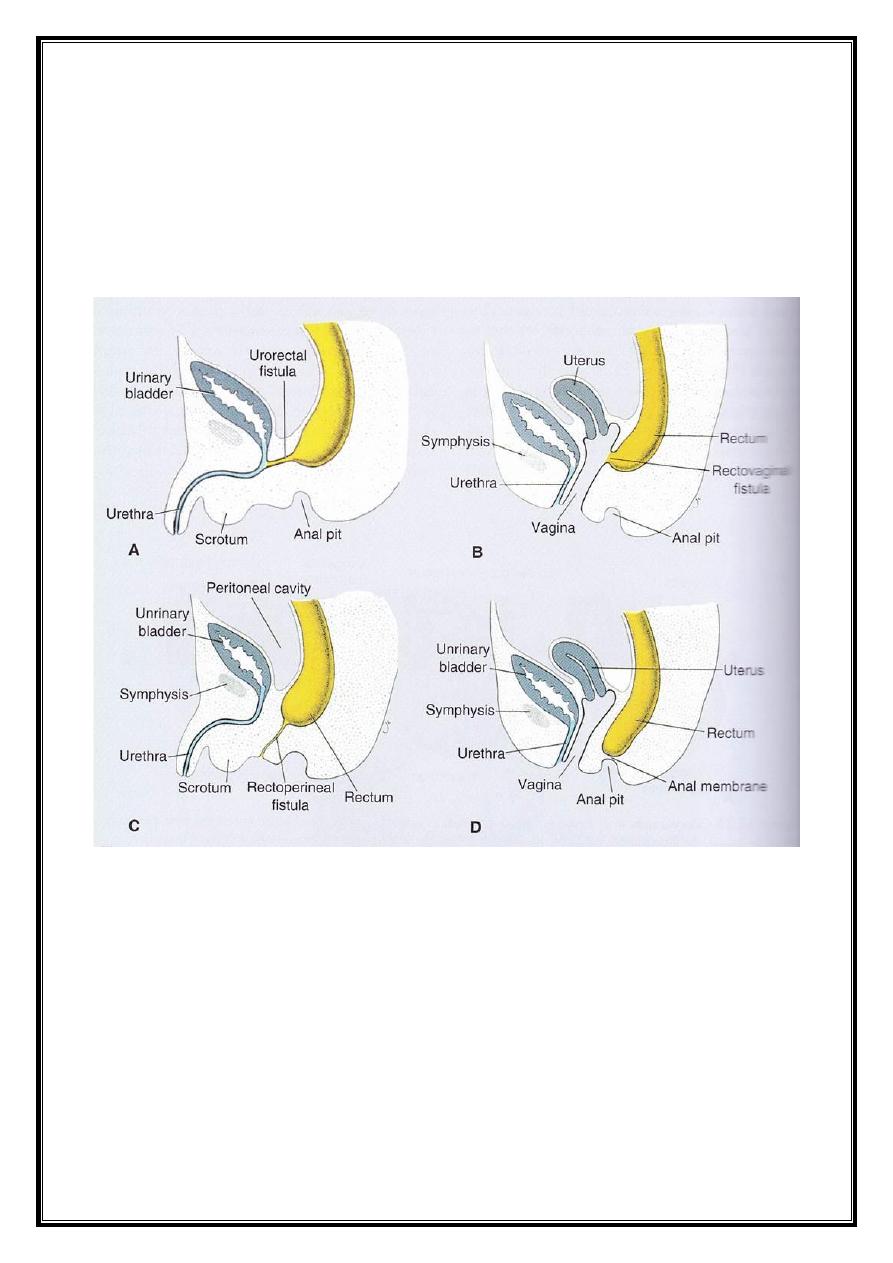
Dr.Maan Alkhalisy Embryology lec. 9 & 10
13
advanced development, the allantois and the hindgut become
nearer to each other.
At the end of the 7
th
week of development, the cloacal
membrane is ruptured creating the anal opening of the hindgut.
Dr.Maan Alkhalisy Embryology lec. 9 & 10
14