
1
Lymphoid System Dr.firdous
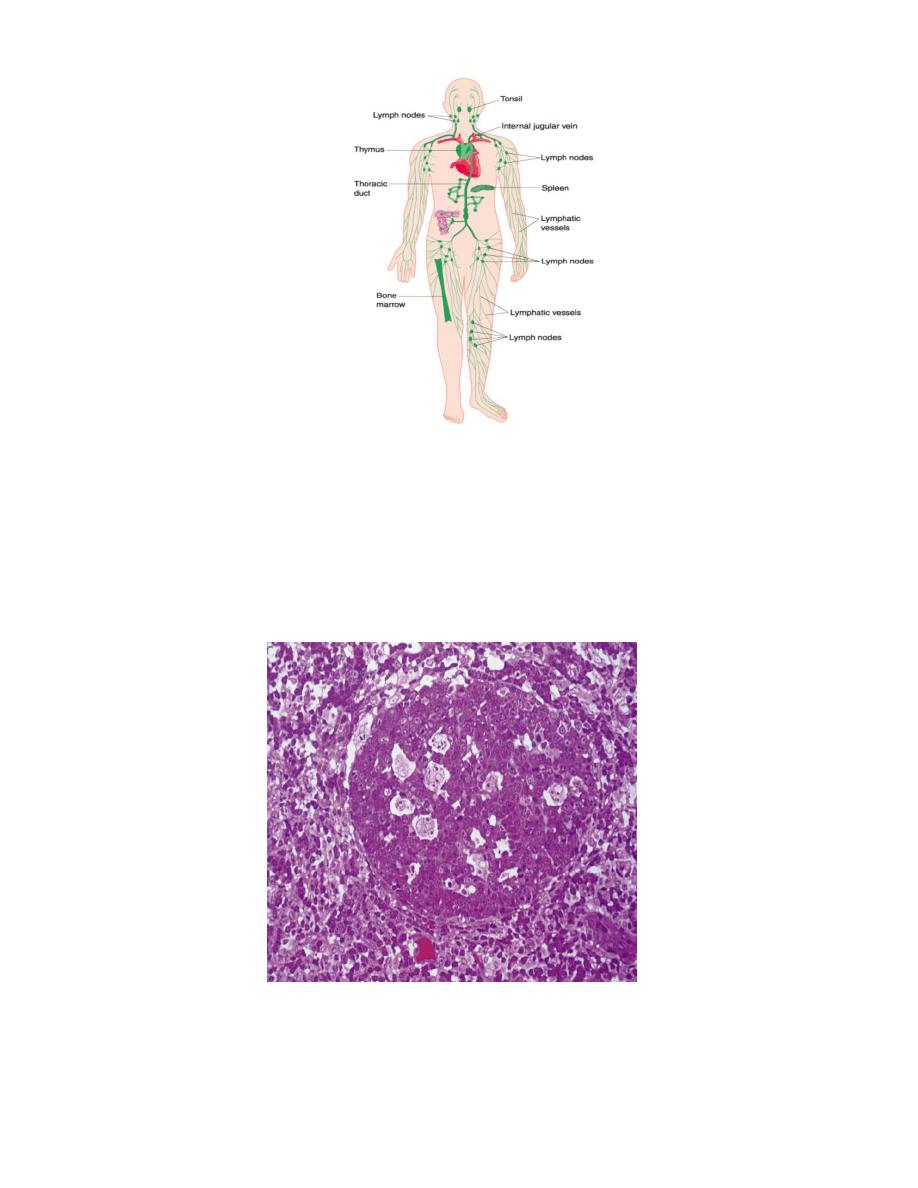
It consists of organs, whose tissues and cells play an important role in immunity; a
protective response of the internal environment of the body against microorganisms and
foreign substances. This system is distributed throughout the body.
Lymphoid tissue is found either in a form of:
1- Individual structure(reticular tissue),as in lymph nodes and spleen, which is
composed of reticular fibers and fixed cells(reticular cells and macrophages)
2- Free cells, as lymphocytes,granulocytes, and mononuclear phagocytic system.
3- Antigen-presenting cells, which are found, in addition to lymphoid tissue, in skin.
There are two types of lymphoid organs:
Central lymphoid organs: as the thymus and bone marrow, where lymphoid cells
precursors undergo antigen-independent prolipheration, to develop as T-lymphocyte(in
the thymus) , or B-lymphocyte(in the bone marrow).
Peripheral lymphoid organs: as the spleen, lymph node, tonsil, Peyer
’
s patches, and
lymphatic nodules in the wall of digestive,urinary,respiratory, and reproductive systems,
where lymphocytes migrate to them after leaving central lymphoid organs.
One of the primary causes of the immunodeficiency syndrome known as AIDS
involves the killing of helper T cells by the infecting retrovirus. This cripples patients'
immune systems rendering them susceptible to opportunistic infections by
microorganisms that usually do not cause disease in immunocompetent individuals.
Tissue grafts and organ transplants are classified as autografts, when the transplanted
tissues or organs are taken from the individual receiving them, isografts, when taken
from an identical twin, homografts ,when taken from an individual (related or unrelated)
of the same species, and heterografts ,when taken from an animal of a different species.
The body readily accepts autografts and isografts as long as an efficient blood supply is
established for the organ. There is no rejection in such cases, because the transplanted
cells are genetically identical to those of the host, and the organism recognizes the grafted
cells as self and does not react with an immune response.
Homografts and heterografts, on the other hand, contain cells whose membranes have
molecules that are foreign to the host; they are therefore recognized and treated as such.
Transplant rejection is a complex process due to the activity of T lymphocytes and
antibodies that react to and destroy the transplanted cells.
2
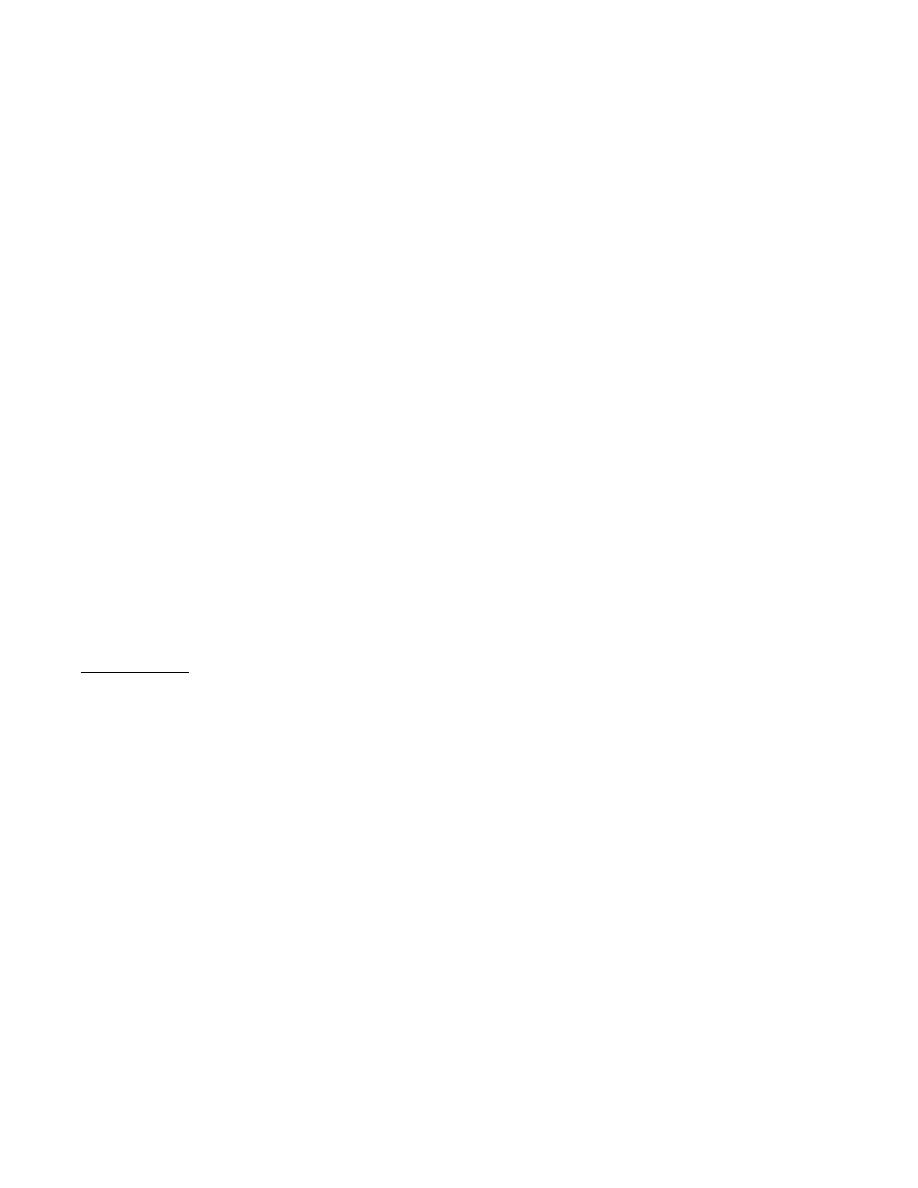
Lymphatic nodule:
Small collections of densely-packed lymphocytes, that appear strongly stained by
haematoxylin in histological section, due to their basophilic nuclei.
The inner region of the nodule shows a less stained area called germinal center, which
contains activated lymphocytes, with pale staining nuclei and larger amount of
cytoplasm. Most lymphocytes in the germinal center are in mitosis. These nodules with
germinal center are called secondary nodules, while those without germinal center are
called primary nodules.
3
There is certain lymphoid tissue present in association with body organs:
MALT(Mucosa Associated Lymphoid Tissue)
GALT(Gut = = = ); in tonsils, esophagus, Peyers
patches, and lymphatic nodules of appendix.
BALT(Bronchus Associated Lymphoid Tissue); in the sub mucosa of bronchus.
Thymus
It is a central lymphoid organ, situated in the mediastinum at the level of great vessels of
the heart.
Development:
Thymus has a dual embryological origin. Its lymphocytes arise from mesenchymal cells
that invade an epithelial primordiam that has developed from the endoderm of the third
and fourth pharyngeal pouches.
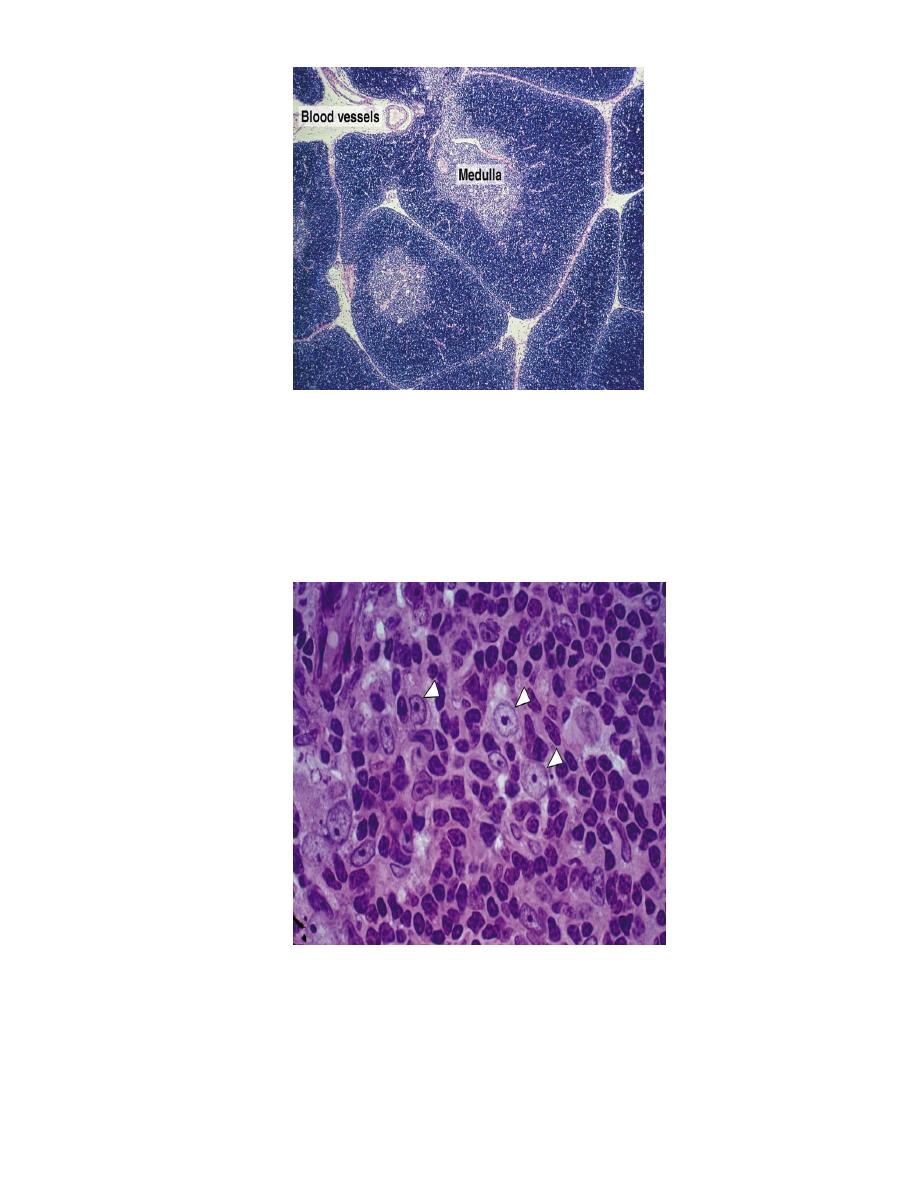
Structure of thymus
The thymus is surrounded by a connective tissue capsule that penetrate the parenchyma,
and divides it into lobules. Each lobule has a peripheral dark zone known as the cortex,
and a central lighter zone, the medulla. The cortical and medullary zones of adjacent
lobules are continuous with each other.
The cortex is composed of extensive population of T lymphocytes, which also known
as thymocytes,(so it stains more basophilic, and appear dark in histological section ),
dispersed epithelial reticular cells, which are called thymic nurse cells, and few
macrophages.
The developing T cells arise from CFU-Ls, which originate in bone marrow. As
development proceeds in the thymus, the cells derived from CFU-Ls pass through a
series of developmental stages that are reflected by their expression of different CD
molecules.
4
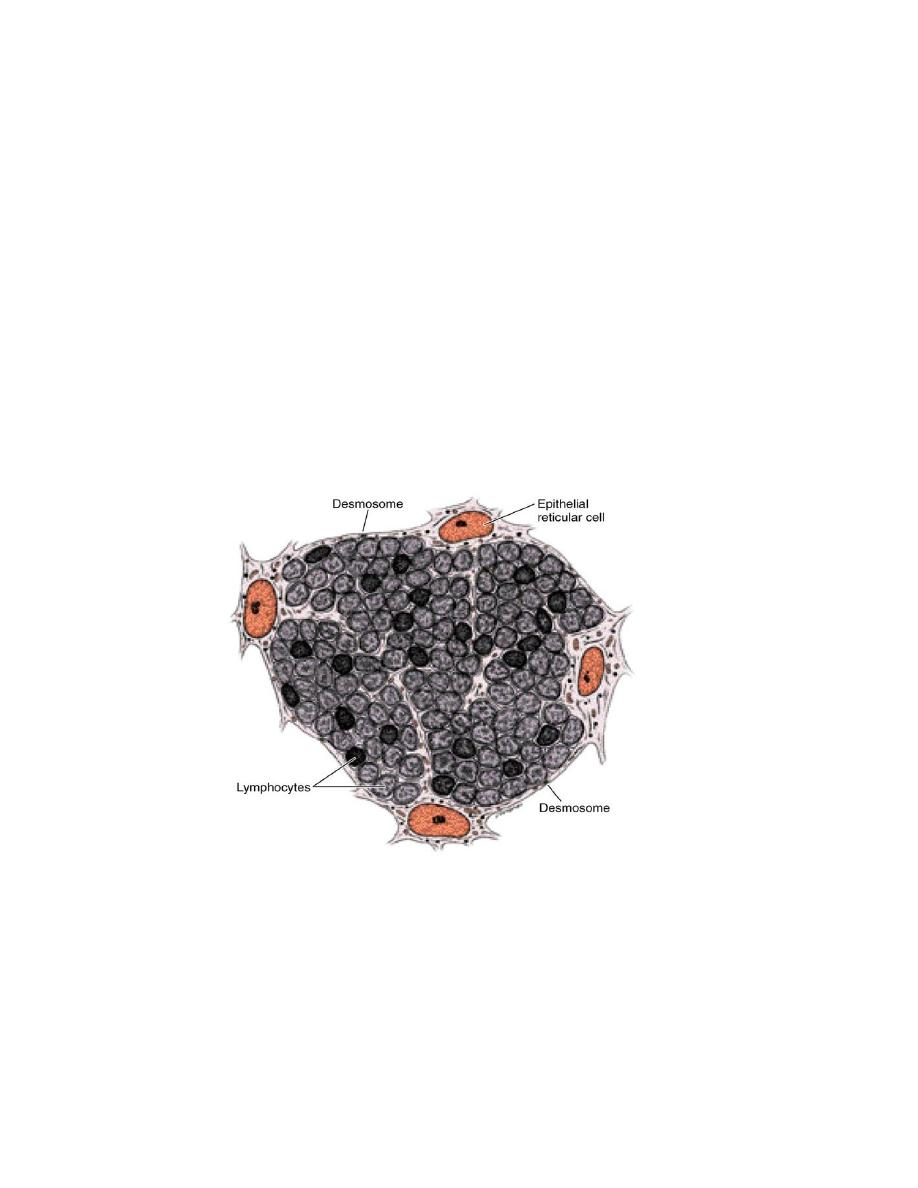
Epithelial reticular cells are stellate cells with light-staining oval nuclei, with one or
two nucleoli, and eosinophilic cytoplasm. Each cell has cytoplasmic processes that joined
to adjacent cell by desmosomes. Bundles of intermediate keratin filaments(tonofibrils) in
the cytoplasm is an evidence of their epithelial origin. The processes of epithelial
reticular cells envelope group of lymphocytes, isolating them from circulating antigen,
and form a complete covering at the periphery of the lobule and around the blood and
lymphatic vessels.
This continuous layer of epithelial reticular cells separates thymic cortical parenchyma
from other histological components of the organ, especially blood vessels, forming the
blood-thymic barrier.
5
This barrier is present only in the cortex, and consists of the following structures:
1- Blood capillary wall, which is of the continuous type, with no fenestrations, and a
very thick basal lamina. The cells are connected by occluding junctions. This will
prevent circulating antigens from reaching T lymphocytes in the cortex.
2- Cytoplasm of endothelial cell.
3- Small amount of connective tissue, with some macrophages.
4-
Basal lamina of epithelial reticular cell.
5- Cytoplasm of = = = .
There are four types of epithelial reticular cells:
1-
Subcapsular-cortical: form a continuous layer to invest blood vessels and septa
2-
Inner cortical: form a spongy like structure with extensive net work of spaces
occupied by lymphocytes.
3-
Medullary: form a sheets of cells which will form large and more solid structure
of the thymus.
4-
Hassall
’s
corpuscle cells: lie deep in the medulla forming a round structure;
Hassall
’
s corpuscle.
While the epithelioreticular cells of the thymic cortex play an important role in the
development of immunocompetent T cells, recent evidence shows that T cells at the
different stages of differentiation control the microarchirecture of the thymic
epithelioreticutar cells, a phenomenon called “crosstalk,” The developing lymphocytes
and epithelioreticular cells thus influence each other during T cell development.
The epithelial cells of the thymic cortex are the source of at least three thymic
hormones (thymosin, thymulin, and thymopoietin) and several other cytokines.
6
The cortex is the site of production of immature T lymphocytes. Most of them will die
and removed by macrophages, only a small number will migrate towards the medulla,
and through venules they will migrate to peripheral lymphoid organs as mature T
lymphocytes.
The medulla stains lightly because of the presence of large number of epithelial
reticular cells, with only 5% of mature lymphocytes .
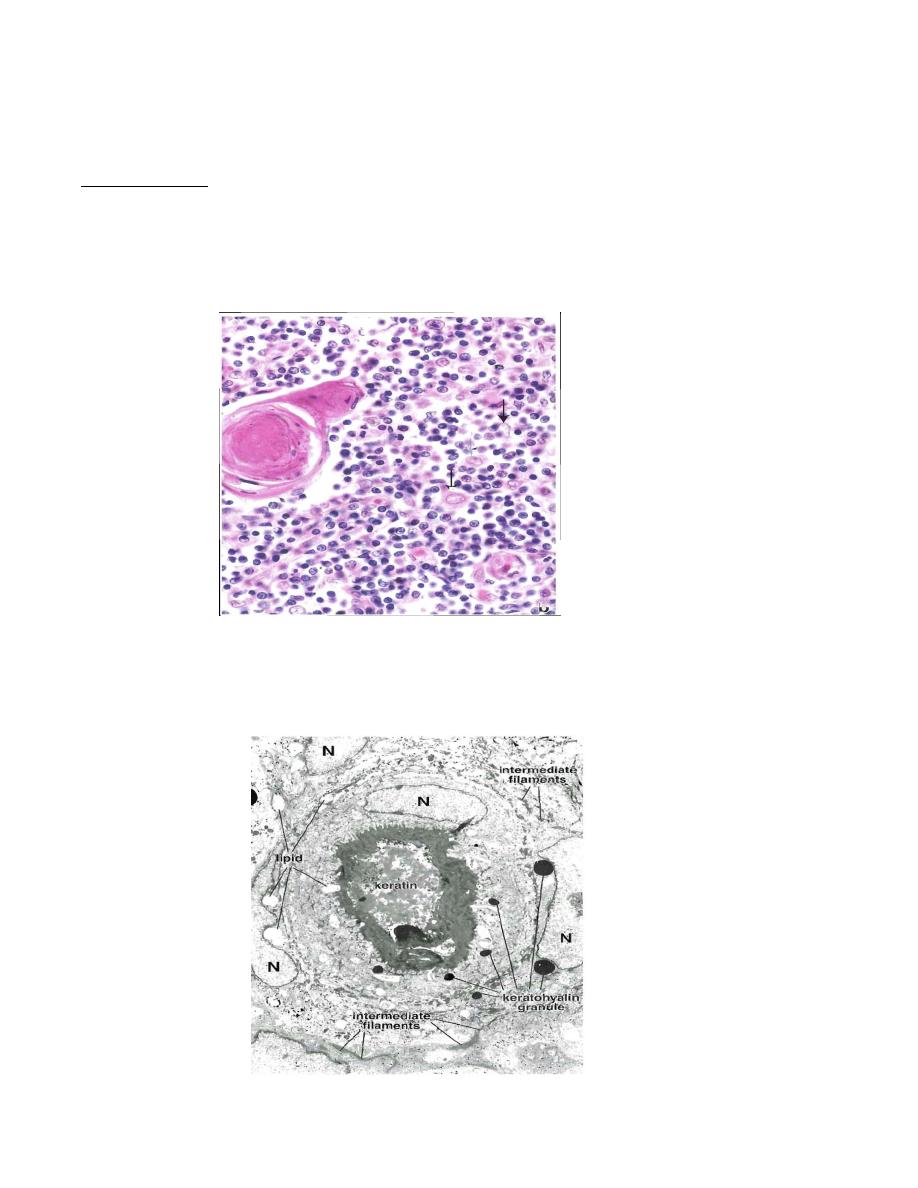
The medulla contains Hassall
’
s corpuscle, which is the characteristic feature of
thymus. It is about 30-150 µm in diameter, consists of concentrically arranged, flattened
epithelial reticular cells that become filled with keratin filaments, degenerate, and
sometimes calcify and die.
Electron microscopical studies of these cells reveal keratohyalin granules, bundles of
cytoplasmic intermediate filaments, and lipid droplets. The cells are joined by
desmosomes. The center of a thymic corpuscle may display evidence of keratinization,
not a surprising feature for cells developed from oropharyngeal epithelium.
7
Thymic corpuscles are unique, antigenically distinct, and functionally active
multicellular components of the medulla. Although the function of thymic corpuscles is
not fully understood, histochemical studies show that they produce thymic hormones
(e.g., thymosin and thymopoietin).
Hassall
’
s corpuscles usually increase in number and size through out life.
Vascularization:
Arteries enter the thymus through the capsule, penetrate deep through the septa, giving
rise to arterioles that supply the parenchyma along the border between cortical and
medullary zones. The arterioles give off capillaries that run in the cortex in an arched
course, finally reach the medulla.. These arterioles also supply the medulla directly by
capillaries. Both cortical and medullary capillaries will drain into venules, which carry
blood into medullary veins that penetrate the connective tissue septa and leave the
thymus through its capsule. The cortico-medullary region contains postcapillary venules
similar to those of the lymph nodes, which allow the passage of lymphocytes into and out
of the thymus.
The thymus has no afferent lymphatic vessels and dose not constitute a filter for
lymph. All lymphatic vessels are efferent, and located in the walls of blood vessels and
connective tissue septa of the capsule.
Secretion by the Thymus
The thymus produces several proteins that act as growth factors to stimulate
proliferation and differentiation of lymphocyte. They seem to be paracrine secretions,
acting in the thymus. At least four hormones have been identified: thymosin- ,
thymopoietin, thymulin, and thymus humoral factor.
Development and Involution of the thymus
The thymus shows its maximum development immediately after birth, then regress
after puberty. It is very sensitive to radiation, glucocorticoids, infectios, and diseases.
Involution begins at the cortical area, where it becomes thinner. Medulla begins its
involution at puperty. At old age, it consists only of reticular cells, Hassall
’
s corpuscles,
few lymphocytes, and large amount of connective tissue.
8
Thymectomy
Removal of the thymus in different stages of life gives different results.
If it is removed at birth, it will cause:
Absence of T lymphocytes in the circulation, with depletion of Thymus-dependant
areas.
Absence of cellular immune response.
Weakness and probable death.
If it is removed at adulthood, it will cause slight decrease in number of lymphocytes, with
slight decrease in weight of lymphoid organs.
Lymph node
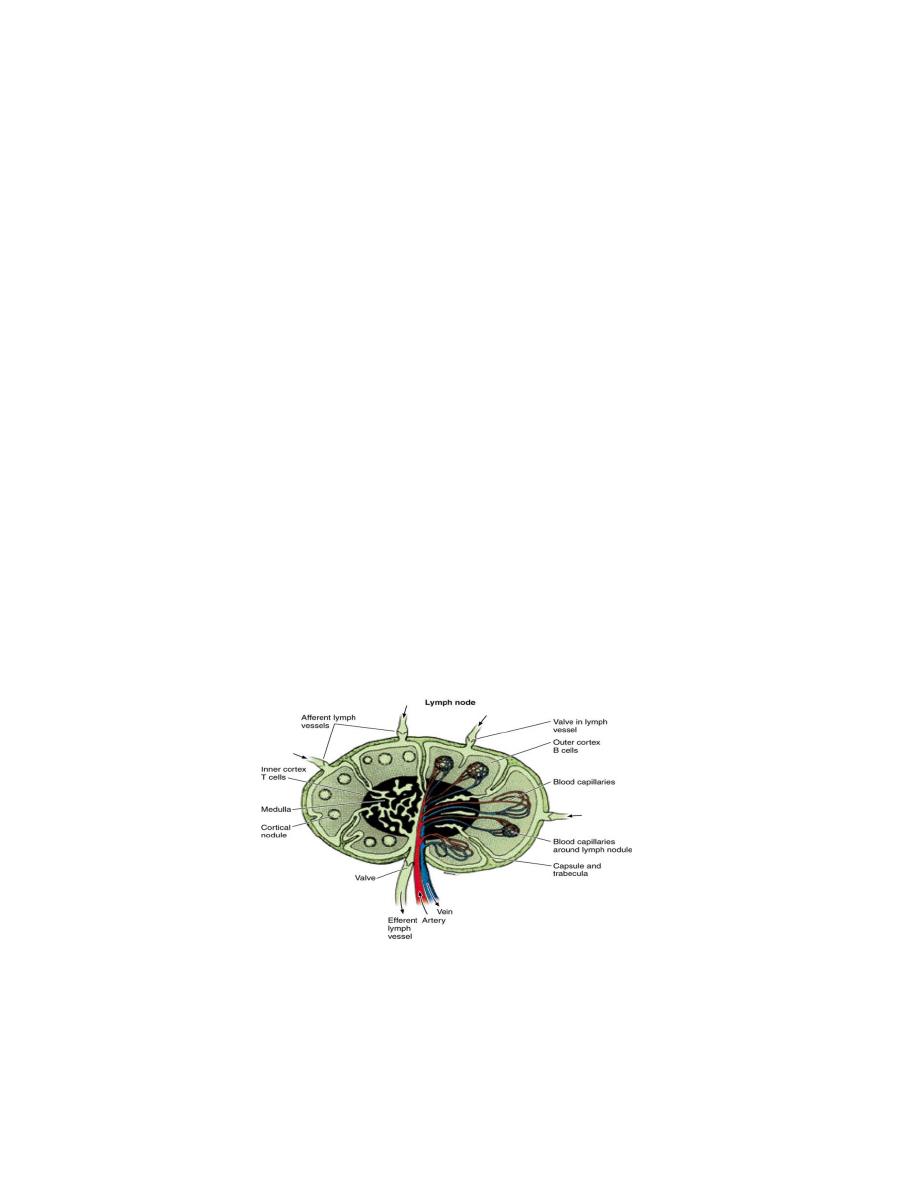
Lymph node is an encapsulated spherical or bean shaped organ, composed of lymphoid
tissue that distributed along the course of lymphatic vessels. Lymph nodes are found in
the axilla, groin, along the great vessels of the neck, thorax and abdomen,
Lymph nodes act as filters which is an important mechanism against microorganisms
and the spread of tumor cells.
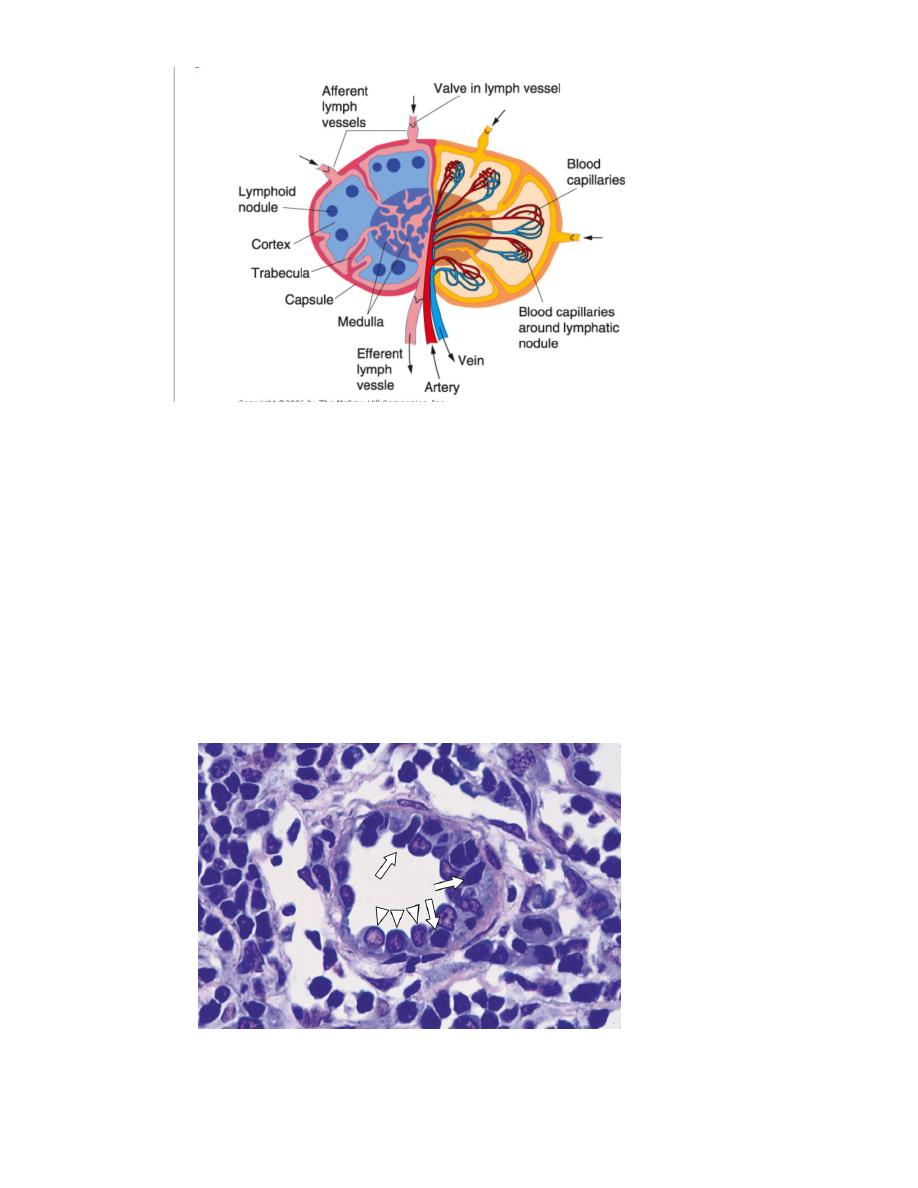
Structure of lymph node:
Each lymph node has a convex side and a concave depression; the hilum, through
which arteries and nerves enter, and veins and lymphatic vessels leave the organ. A
connective tissue capsule surrounds the node, sending trabeculae into the interior. Each
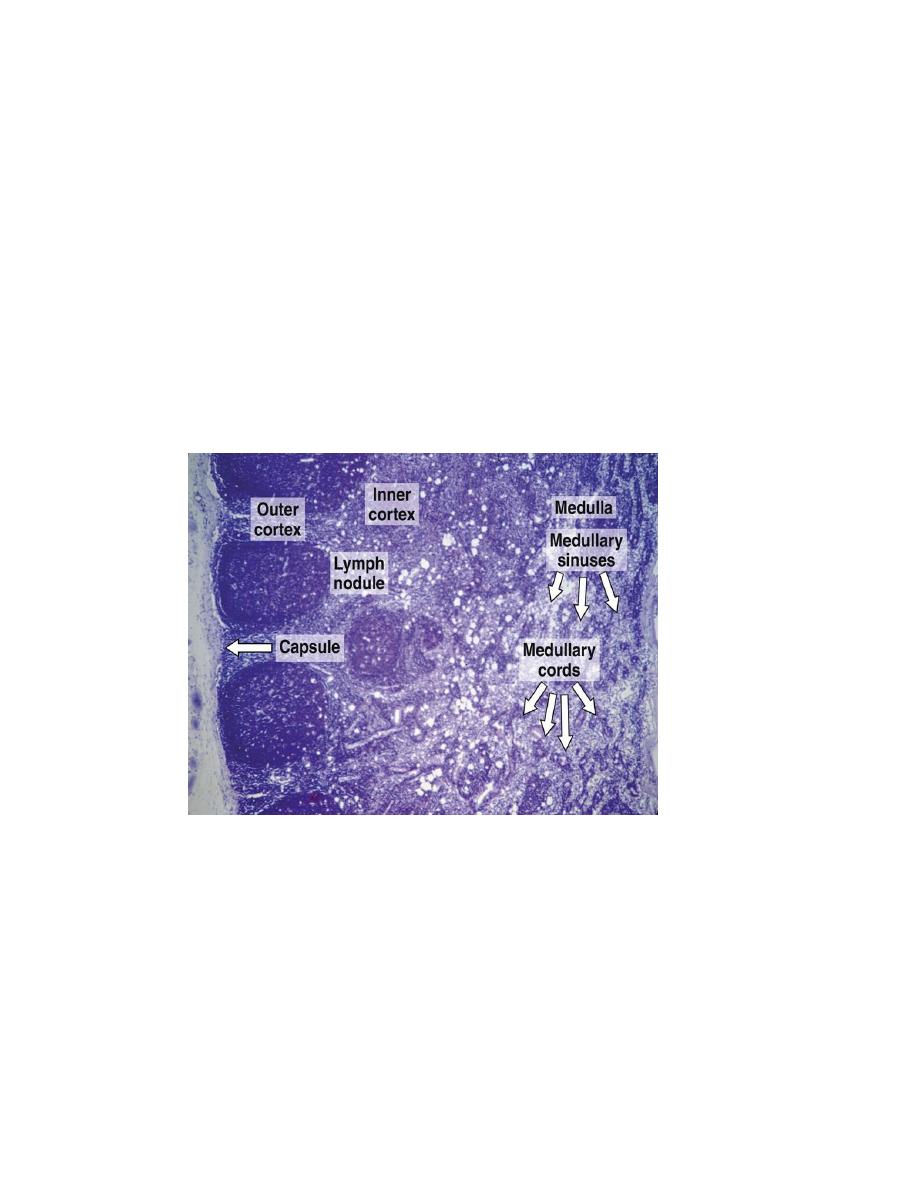
node contains an outer cortex, inner cortex, and medulla.
Cortex
The outer cortex, situated under the capsule, consists of the following components:
1. A diffuse population of cells composed mainly of T lymphocytes and reticular cells.
Macrophages and APCs are also present in this area. The reticular meshwork of
9
lymphatic tissues and organs (except the thymus) consists of cells of mesenchymal origin
and reticular fibers and ground substance produced by those cells, The cells of the
reticular meshwork appear as stellate or elongated cells with an oval euchromatic nucleus
and a small amount of acidophilic cytoplasm.
2. Lymphoid nodules, with or without germinative centers, formed mainly by B
lymphocytes, embedded in the diffuse population of cortical cells
3. Areas of loose lymphoid tissue whose reticular fibril meshes are situated immediately
beneath the capsule, called the subcapsular sinuses .They are composed of a loose
network of reticular cells and fibers. Lymph, containing antigens, lymphocytes, and
APCs, circulates around the spaces of these sinuses after being delivered into these
channels by the afferent lymphatic vessels
.
4. Intermediate or radial sinuses that run between lymphoid nodules. These sinuses arise
from and share the same structure with the subcapsular sinuses. They communicate with
the subcapsular sinuses through spaces similar to those present in the medulla
Follicular dendritic cells : have multiple, thin, hair-like branching cytoplasmic
processes that interdigitate between B lymphocytes in the germinal ceitrers
mAntigen—antibody complexes adhere to the dendritic cytoplasmic processes by means
of the antibody’s F receptors, and the cell can retain antigen on its surface for weeks or
months. Although this mechanism is similar to the adhesion of antigen—antibody
complexes to macrophages, the antigen is not generally endocytosed, as it is by the
macrophage.
10
The inner cortex or paracortical region does not have precise boundaries with the
outer cortex and contains few,
nodules but many T lymphocytes. It is a thymus dependant
area
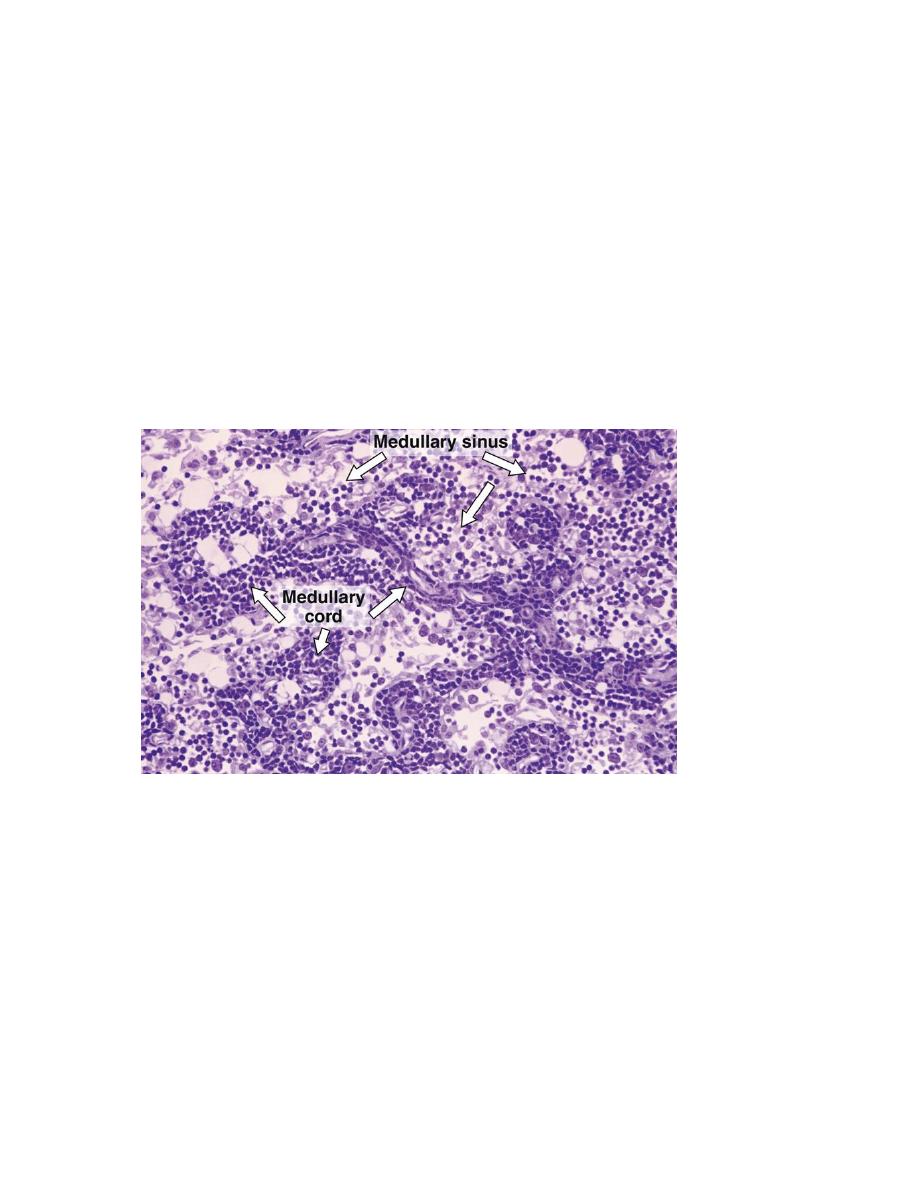
Medulla
The medulla has two components:
1. The medullary cords :are branched cordlike extensions of dense lymphoid tissue that is
continuous with the inner cortex. They contain primarily B lymphocytes and often
plasma cells and macrophages The medullary cords are separated by dilated spaces,
frequently bridged by reticular cells and fibers, called medullary sinuses.
2. medullary sinuses :they contain lymph, lymphocytes, often many macrophages,
sometimes even granulocytes if the lymph node is draining an infected region. These
sinuses (which arise from the intermediate sinuses) join at the hilum delivering the
lymph to the efferent lymph vessel of the lymph node.
Lymph and Blood circulation:
Afferent lymphatic vessel cross the capsule of the node and pour lymph into the sub
capsular sinus. From there, lymph pass through intermediate sinuses or trabecular
sinuses ,that run parallel to the trabeculae of the capsule and into the interior of the node,
where they reach medullary sinuses. After filtration of lymph by macrophages and
dendritic cells present in the sinuses, it will be collected by efferent lymphatic vessels at
the hilum.
11
Small arteries enter the node through the hilum, and form capillaries in the lymphoid
nodules, where small veins originate and exit at the hilum.
Lymphocytes leave the lymph node by efferent lymphatic vessels to reach blood
stream, then return back to lymph node by specific blood vessels; the post capillary or
high endothelial venules. These venules have an unusual endothelial lining of tall
cuboidal cells, and lymphocytes can travel between them. These venules also present in
the appendix, tonsils, and Peyer
’
s patches.
These specialized endothelial cells possess
receptors for antigen-primed lymphocytes. They signal lymphocytes to leave the
circulation and migrate into the lymph node. Both B and T cells leave the bloodstream
through high endothelial venules, crossing the endothelium by diapedesis, i.e., by
migrating between the endothelial cells. The T cells remain in the thymus-dependent
deep cortex; the B cells migrate to the nodular cortex. Most lymphocytes leave the lymph
node by entering lymphatic Sinuses from which they flow to an efferent lymphatic vessel.
Although plasma cells constitute only 1 – 3% of the cell population in resting nodes,
their numbers increase greatly in stimulated lymph nodes.
12
Enlargement of the lymph node is either due to an infection in the area they drain, as
in tonsillitis or pharyngitis , or due to an invasion of the lymph node itself by the
microorganism , as in tuberculosis, and toxoplasma gondii.
Another common cause of lymph node enlargement is malignant tumours , whether
primary malignancy as lymphoma and leukaemia, or as a secondary invasion by
metastasis.
Spleen
The spleen is the largest lymphoid organ in the body. It has an important defense
mechanism against microorganisms in the circulation because of the presence of
phagocytic cells. It is also the site of destruction of aged erythrocytes, and production of
activated lymphocytes. The spleen plays an important role in immunity and antibody
formation.
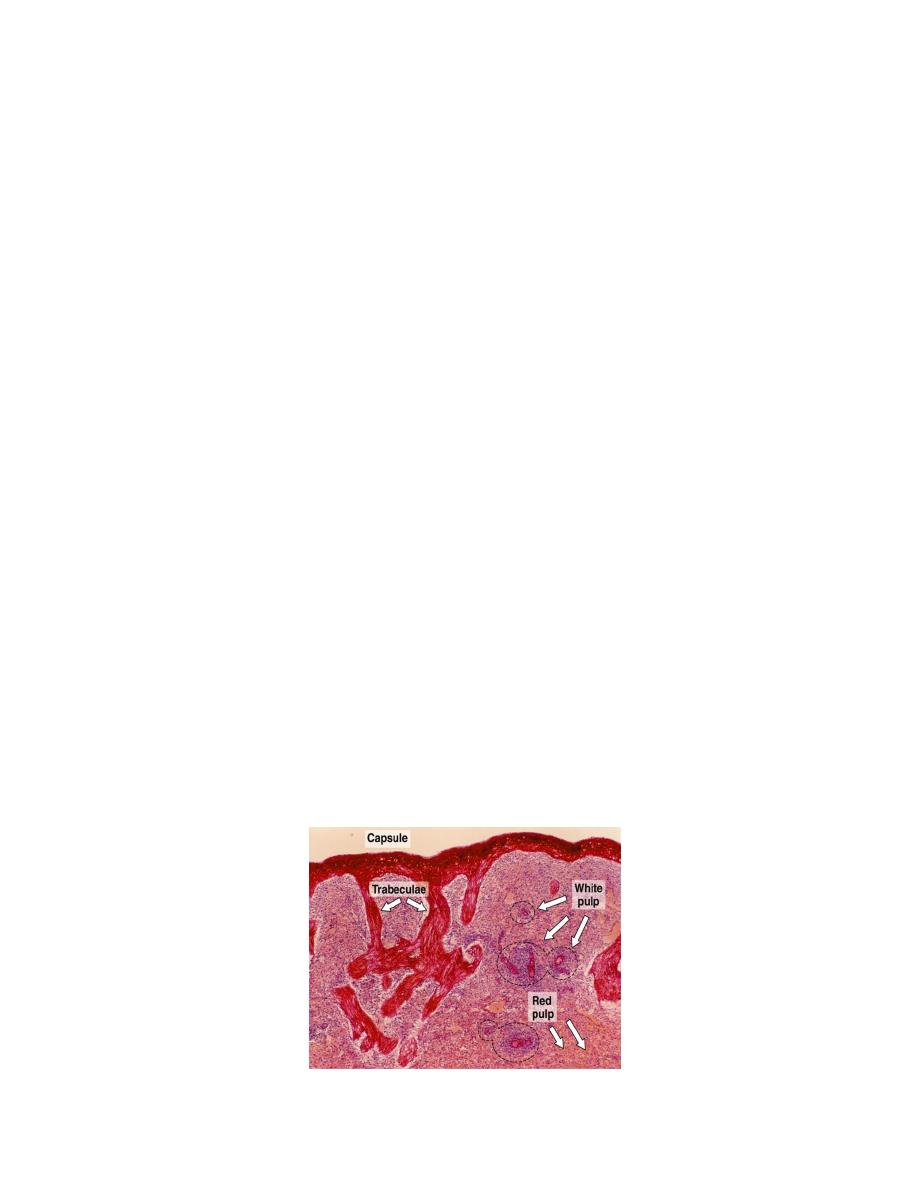
Structure of spleen:
The spleen is surrounded by a dense connective tissue capsule that sends trabeculae in
to the parenchyma, dividing it into incomplete compartments. The human spleen normaly
retains relatively little blood, but it has the capacity for contraction by means of the
contractile cells in the capsule and trabeculae.
The medial side of the spleen is invaginated as the hilum, where arteries and nerves
enter, and veins leave the organ. In humans, the connective tissue of the capsule and
trabeculae contains few smooth muscle cells. The structure of spleen is composed of
network of reticular tissue that contains lymphoid cells, macrophages, and antigen-
presenting cells(APC).
Splenic pulp:
In a fresh spleen, we can see white spots on the surface, which represent lymphoid
nodules(white pulp). These nodules are found within the red pulp, a dark red tissue that is
rich in blood.
13
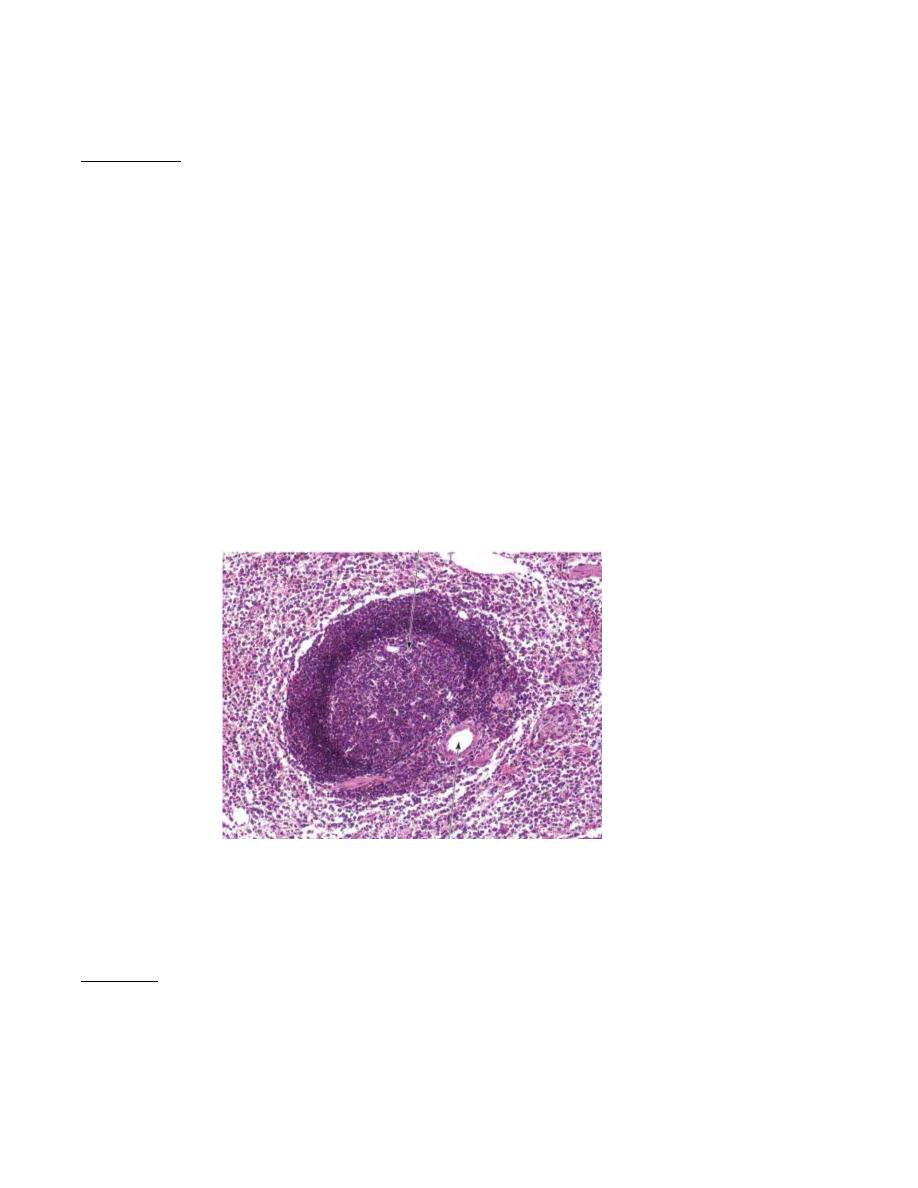
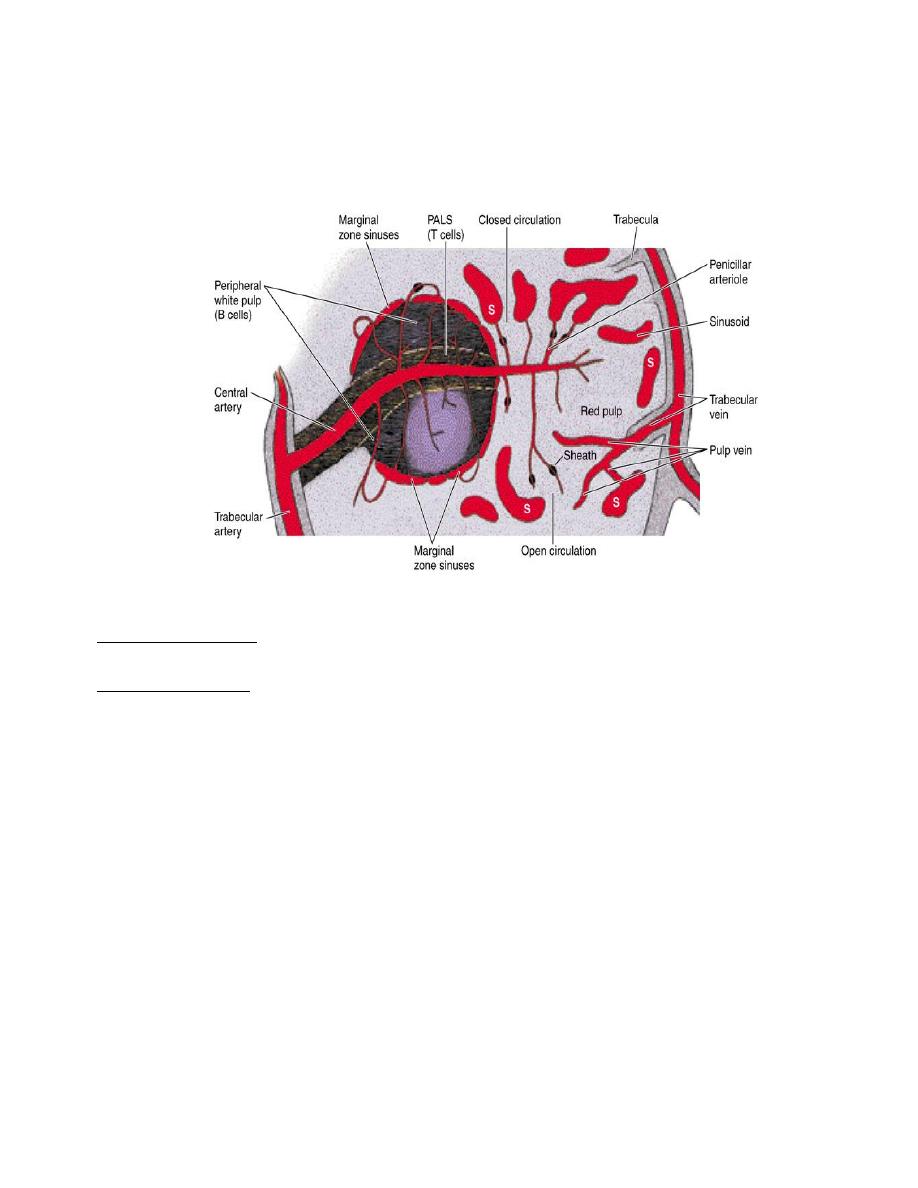
White pulp:
It consists of lymphoid tissue arranged in sheathes around central artery and lymphoid
nodules. The lymphoid cells that surround the central artery are mainly T-lymphocytes,
and form the peri arterial lymphatic sheath(PALS).
The PALS has a roughly cylindrical configuration that conforms to the course of the
central artery. In cross Sections, the PALS appears circular and may resemble a
lymphatic nodule. The presence of the central artery, however, distinguishes the PALS
from typical lymphatic nodules found in other- sites. Nodules appear as localized
expansions of the PALS and displace the central artery, so that it occupies an eccentric
rather than a central position.
Lymphatic nodule consists mainly of B-lymphocytes. The nodules usually contain
germinal centers, which, as in other lymphatic tissues, develop as B cells following their
activation. In humans, germinal centers develop within 24 hours after antigen exposure
and may become extremely large and visible with the naked eye. These enlarged nodules
are called splenic nodules or Malpighian corpuscles (not to be confused with the renal
corpuscles that have the same name).
Between white pulp and red pulp lies a marginal zone, consisting of many sinuses and
loose lymphoid tissue, rich in active macrophages and few lymphocytes. Marginal zone
contains an abundance of blood antigens , so plays a major role in immunity.
Lymphocytes of the central portion of PALS are thymus-dependant, while marginal
zone and lymphatic nodules (peripheral white pulp) are populated by B-lymphocytes.
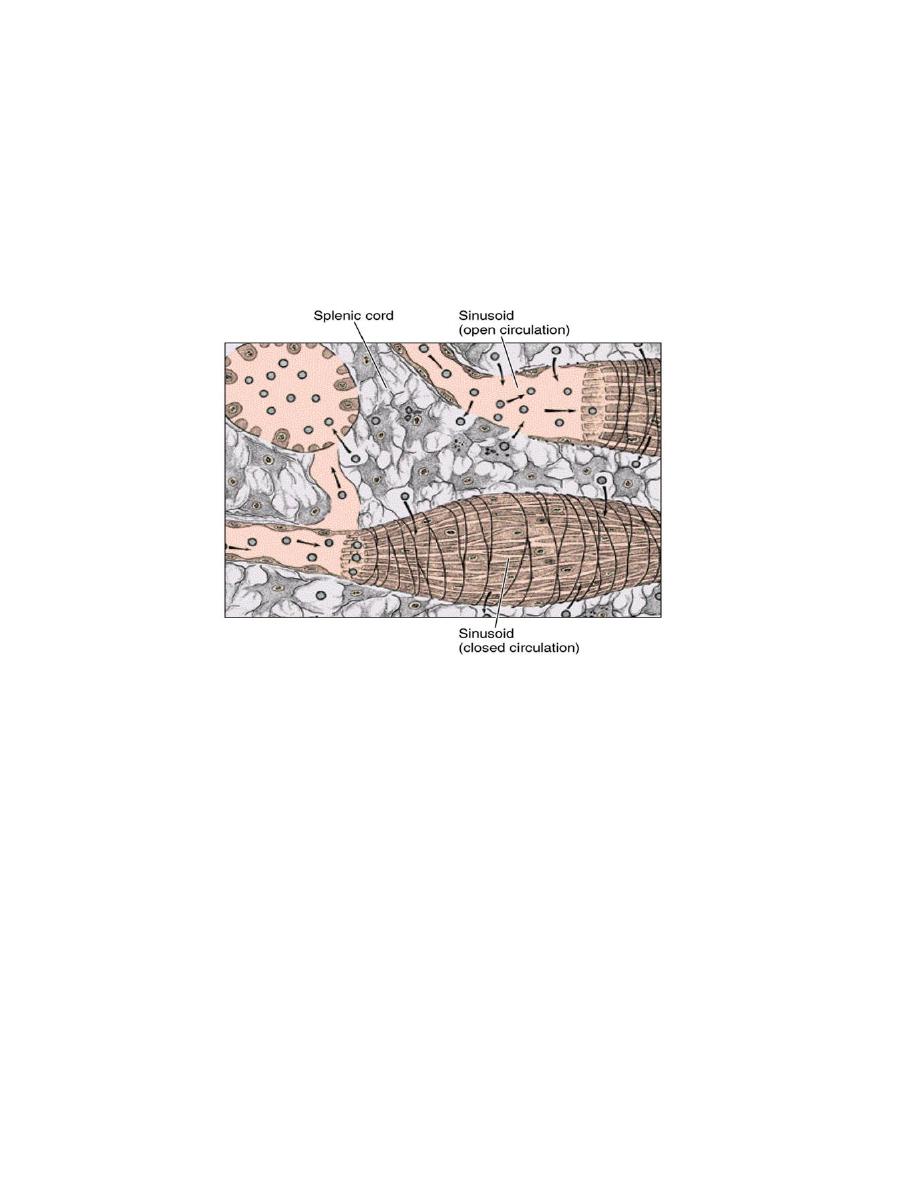
Red pulp:
It is a reticular tissue which is composed of splenic cords(Billroth
’
s cords), and
sinusoids.
14
Splenic cords are composed of loose network of reticular cells supported by reticular
fibers. They also contains macrophages, T and B-lymphocytes, plasma cells, and many
blood cells. These cords have variable thickness according to the local distention of the
sinusoids.
Splenic sinusoids are lined by an elongated endothelial cells, with their long axis
parallel to the long axis of the sinusoids. Endothelial cells are enveloped by reticular
fibers which arranged in a transverse direction like barrel hoops. Transverse and
longitudinal fibers join to form a network enveloping the sinusoid cells and macrophages
that occupy the spaces between endothelial cells. The sinusoids are covered by
incomplete basal lamina.
The space between endothelial cells is only 2-3 µm in diameter or smaller, allowing
flexible cells only to pass from red pulp cords to the lumen of sinusoids.
The zone of red pulp immediately surrounding the white pulp is devoid of sinuses,
having only sparse reticulin meshwork and large number of red and white blood
cells.This zone is known as perilymphoid or perifollicular zone.The blood flow slowly in
this area to enhance the interaction of blood cells, antigen, and antibody.
Blood circulation:
Splenic artery enters the hilum, divides into trabecular arteries, which are of variable
sizes that follow the course of trabeculae. After leaving trabecula, these arteries will enter
the parenchyma of spleen, and will be enveloped by a sheath of T-lymphocytes called
peri arterial lymphatic sheath (PALS). These arteries are called central arteries or white
pulp arteries. Although it is called central artery, it occupies an eccentric position in the
white pulp, where it divides into many radial branches that supply the surrounding
lymphoid tissue.
15
After leaving white pulp, central artery subdivides to form straight penicillar arterioles
with an outside diameter of 24µm. Near their termination, penicillar arterioles continues
as arterial capillaries, which may be surrounded by macrophages, and thus called
sheathed capillaries.
When they leave the sheath, these vessels carry blood to the red pulp sinusoids.
There are two theories to explain the flow of blood from capillaries to red pulp
sinusoids:
Closed circulation: where capillaries open directly into the sinusoids; the blood always
remains inside the vessels.
Open circulation: where blood pass through the spaces between the red pulp cord cells
and then collected by sinusoids; the circulation will open into the parenchyma of the red
pulp. Human circulation is of the open type.
Open circulation exposes the blood more efficiently to the macrophages of the red
pulp. Both transmission and scanning electron micrographs often show blood cells in
transit across the endothelium of the sinus, presumably reentering the vascular system
from the red pulp cords.
From sinusoids, blood will be collected by red pulp veins that join together and enter
the trabeculae as the trabecular veins, which will pour blood into splenic vein that leave
the spleen at the hilum. Trabecular vein wall is composed of the trabecular tissue, with no
muscular wall.
16
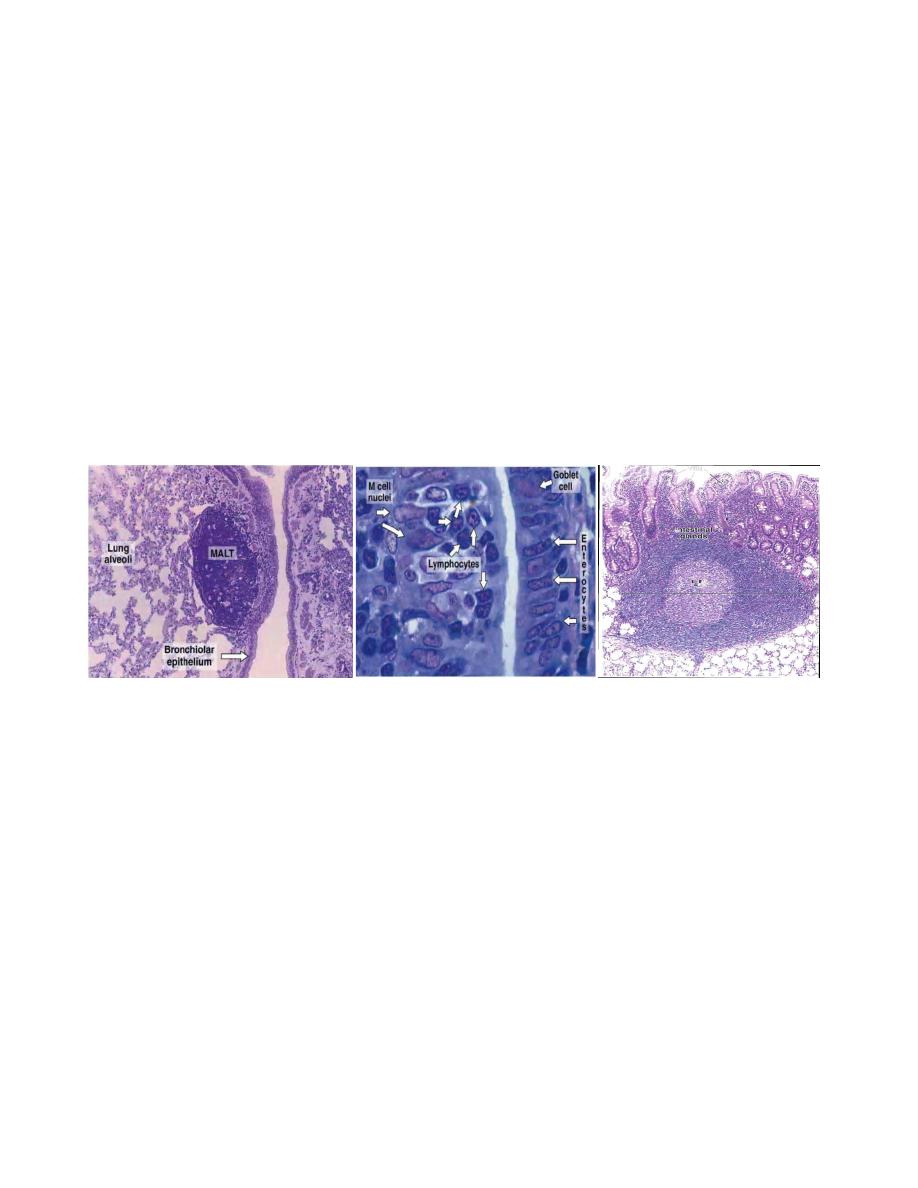
MUCOSA-ASSOCIATED LYMPHOID TISSUE & TONSILS
The digestive, respiratory, and genitourinary tracts are common sites of microbial
invasion because their lumens are open to the external environment.
. To protect the organism, the mucosa and submucosa of these tracts contain large
amount of diffuse collections of lymphocytes, IgA-secreting plasma cells, APCs, and
lymphoid . Most of the lymphocytes are B cells; among T cells, helper cells
predominate. In some places, these aggregates form conspicuous structures such as the
tonsils and the Peyer's patches in the ileum. Similar aggregates are found in the appendix.
In the Peyer's patches, some of the regular surface epithelial cells may be replaced by
special M cells.
The M cells do not have microvilli as do the regular cells that line the intestine. By
pinocytosis they actively capture and transport antigens from the intestinal lumen to the
connective tissues where APCs and B lymphocytes are usually present .The plasma cells
derived from these lymphocytes secrete mostly IgA, which is transported through the
epithelium toward the intestinal cavity.
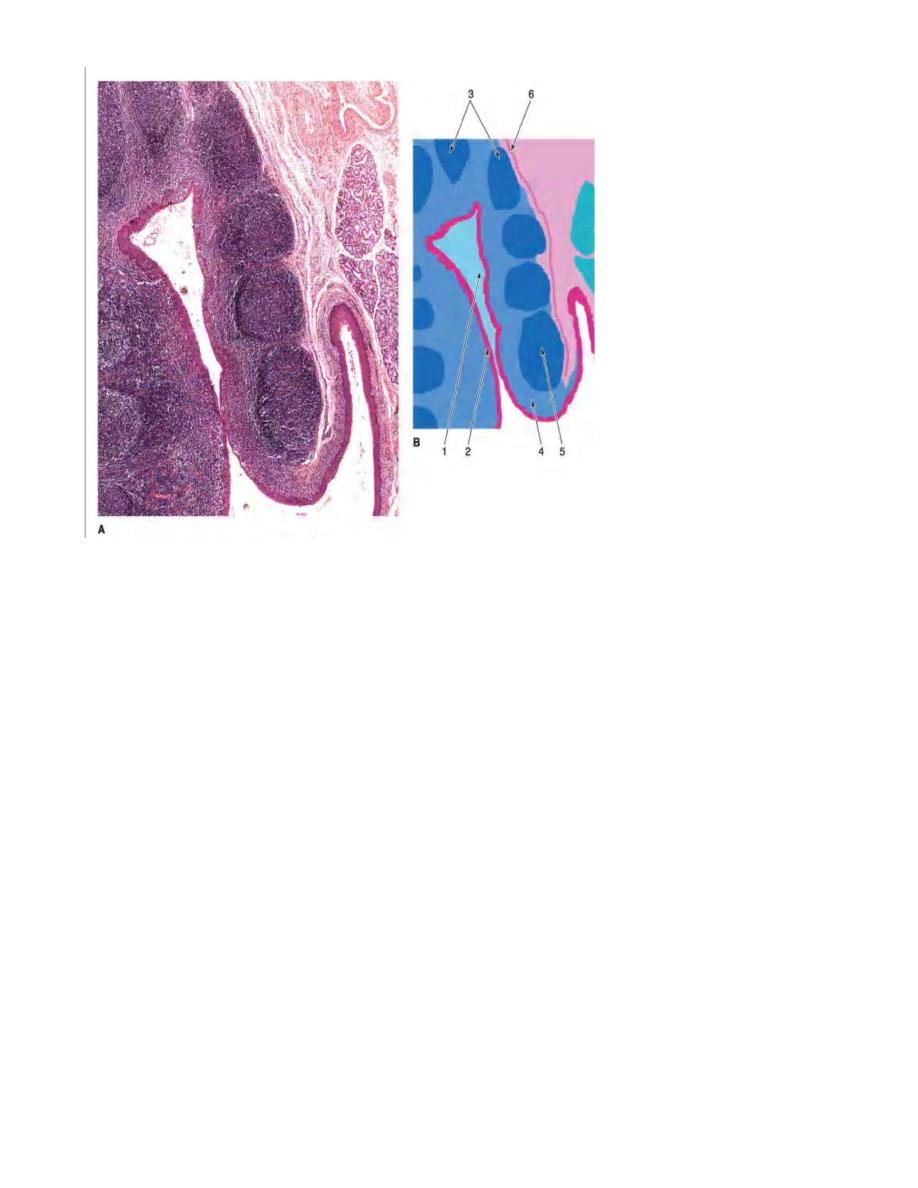
Tonsils
Tonsils are aggregates of incompletely encapsulated lymphoid tissue that lie beneath,
and in contact with, the epithelium of the upper part of digestive tract.
Palatine Tonsils:
There are two tonsils located in the lateral walls of the oral part of the pharynx. The
tonsil is covered by stratified sequamous epithelium, and composed of dense lymphoid
tissue in a form of lymphatic nodules, generally with germinal center. Each tonsil has
about 10-20 epithelial invaginations that penetrate the parenchyma deeply, forming
crypts, whose lumens contain desequamated epithelial cells, live and dead lymphocytes,
and bacteria. In tonsillitis, these crypts appear as purulent spots.
A thick connective tissue capsule separates lymphoid tissue of the tonsil from
underlying structures, preventing the spread of infection.
17
Pharyngeal tonsil:
Single tonsil located in the superior-posterior portion of the pharynx. It is covered by
ciliated pseudostratified columnar epithelium (respiratory epith.), with some areas of
stratified epithelium can be seen.
Pharyngeal tonsil consists of folds of mucosa and contains diffuse lymphoid tissue and
nodules. It has no crypt, and the capsule is thinner than that of palatine tonsil.
Adenoid is a hypertrophy of this tonsil resulting from chronic infection.
Lingual tonsils:
Small and multiple lymphoid tissue, located at the base of the tongue. They are covered
by stratified sequamous epithelium, and each tonsil has a single crypt.