1
Physiology
Dr. Basim Mohamad Alwan
Lecture (7)
THE THALAMUS
The two thalami are large avoid masses of gray matter situated at the lateral
walls of the third ventricle, one on each side. They are interconnected by a
short communicating bar of white matter (Massa intermedia) which
traverses the third ventricle. Thalamus operates in close association with
cerebral cortex, so both are sometimes called thalamo-cortical system.
All the nervous signals which go to the cerebral cortex pass first through
and relay in the thalamus. That is why the thalamus is sometimes called
the "secretary of the cerebral cortex ".
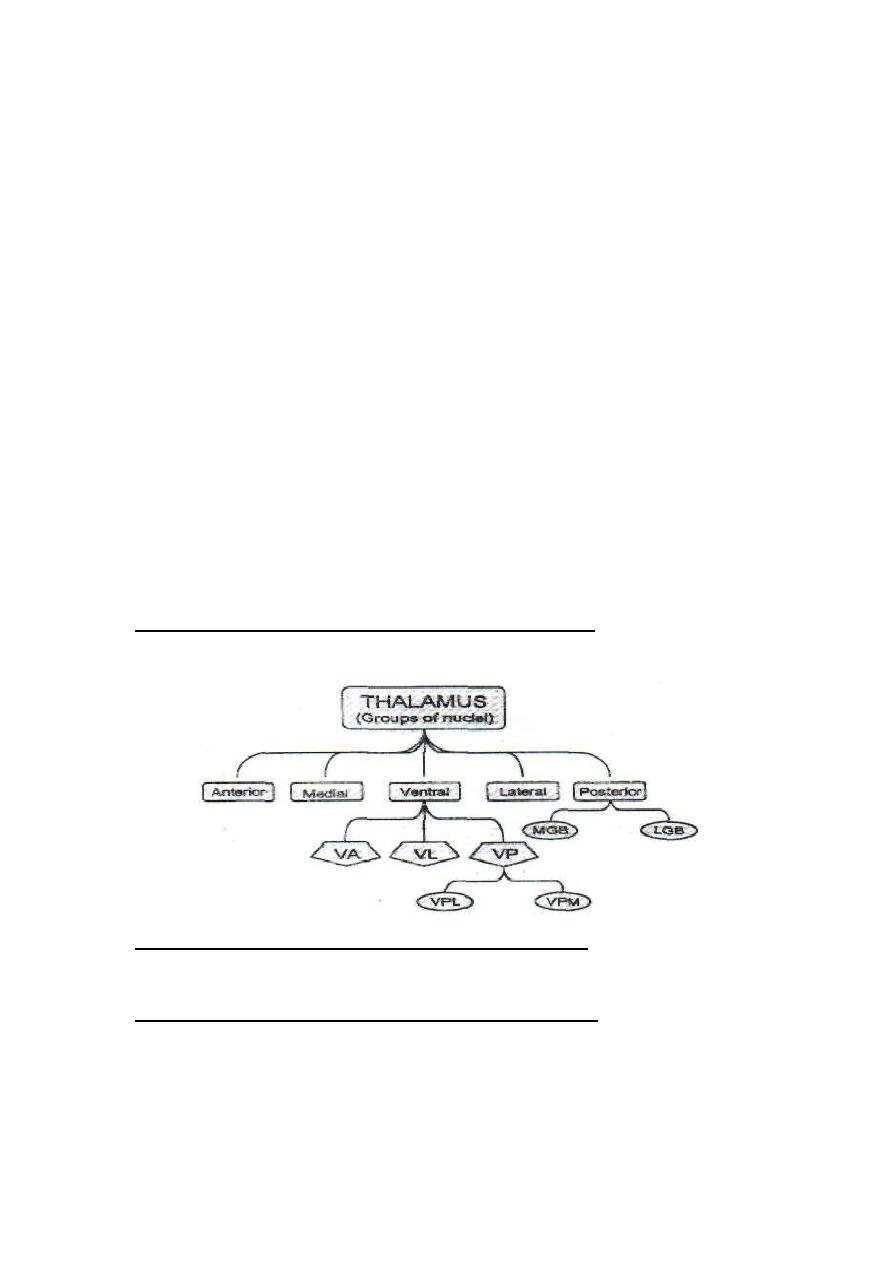
ANATOMICAL DIVISIONS OF THE THALAMUS
In each thalamus there are 5 groups of nuclei:
FUNCTIONAL DIVISIONS OF THE THALAMUS
Functionally, the thalamic nuclei could be classified into four categories:
[I] Specific projection nuclei (cortical relay nuclei):
a. Ventral posterolateral nucleus (VPL), which is the site of
relay of the somatic sensory pathways from the trunk and limbs
b. Ventral posteromedial nucleus (VPM), which is the site
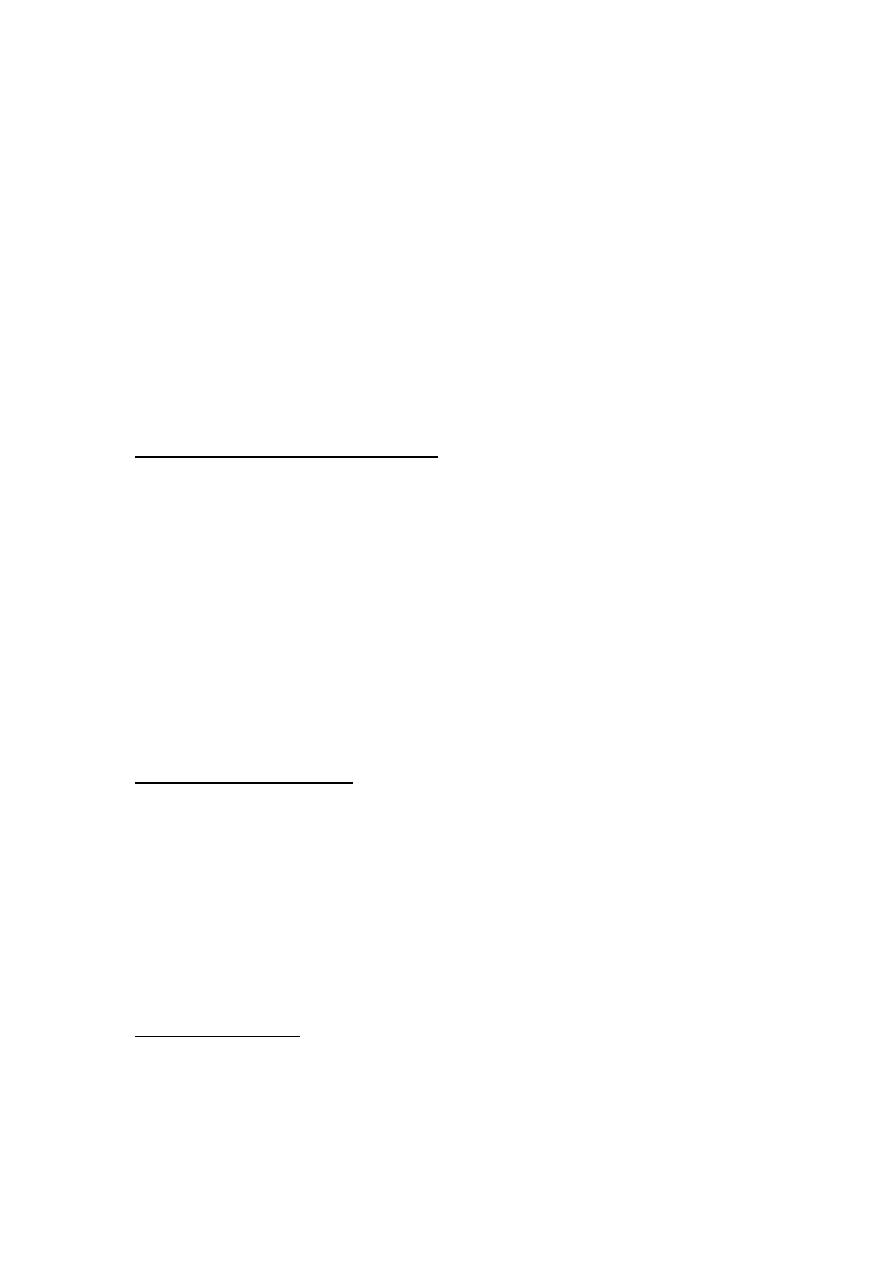
2
of relay of the trigeminal sensory pathway from the head.
c. Medial geniculate body (MGB); site of relay of the auditory
pathway.
d. Lateral geniculate body (LGB): site of relay of the visual pathway.
AFFERENT CONNECTIONS: From the medial, spinal and trigeminal
lemnisci, optic tract, auditary pathways.
EFFERENT CONNECTIONS: Specific thalamic projection system to
specific points in the somatic audio and visual sensory areas of the
cerebral cortex.
[II] Nonspecific projection nuclei:
a. Intralaminar and midline nuclei.
b. Ventroanterior nucleus.
c.
Anterior nuclei.
AFFERENT CONNECTIONS: From the ascending reticular activating
system (ARAS), and the paleospinothalamic tracts.
EFFERENT CONNECTIONS: Nonspecific thalamic projection fibers to
all parts of the cerebral cortex. The anterior nuclei are connected to the
hypothalamus and limbic system.
[III] Association nuclei:
a. Dorsolateral nucleus.
b. Posterolateral nucleus.
AFFERENT CONNECTIONS: From other thalamic nuclei
EFFERENT CONNECTIONS: Posterolateral nucleus projects to
prefrontal cortical area, while the dorsolateral nucleus projects to the
cortical association areas.
[IV] Motor nuclei:
The most important of these is the ventrolateral nucleus VL
AFFERENT CONNECTIONS: From the basal ganglia and cerebellum.
EFFERENT CONNECTIONS: The motor cortex.
3
FUNCTIONS OF THE THALAMUS
1. It is a relay station for all the sensory pathways in their way to the
cerebral cortex except olfaction. Sensory signals are processed in the
thalamus before reaching the cortex (thalamus is the secretary of the
cortex).
2. It acts as a final sensory center for conscious perception of some
sensations: i.e. slow pain, high or low grades of temperature and crude
touch.
3. Facilitation of the cerebral cortex, raising its excitability up to the
4
level necessary to do all cerebral functions. Without the thalamus, the
cerebral cortical functions are markedly depressed. The cerebral cortex
and thalamus are sometimes considered as one unit called "the
thalamocortical system".
4. Identification of the stimulus affect (pleasant or unpleasant), and
controlling the emotional and motor reactions to it. This is done in
collaboration with the cerebral cortex, the limbic system and
hypothalamus
5. It is part of the limbic circuit which is concerned with recent memory
and memory search.
6. It is part of the caudate and putamen circuits which control the
motor activity
7. It is involved in control of high intellectual cortical functions and
the behavior and personality through its connections with the cortical
association areas and with the prefrontal cortical areas respectively.
THE THALAMIC SYNDROME
(The thalamic hypersthetic anesthesia)
The most common cause of this syndrome is thrombosis of the
thalamogeniculate artery which is a branch of the posterior cerebral artery.
This leads to degeneration of the posterior and ventral parts of the
thalamus. The manifestations which appear on the contralateral side of
the lesion include:
SENSORY EFFECTS
First, there is complete hemi anesthesia at the onset of the disease except the
upper part of face sensation is retained. Few weeks later protopathic
sensation (primitive sensations which include crude touch, slow pain
and high or low temperatures) are recovered. The threshold of pain is
elevated but gives very unpleasant severe agonizing pain when it is reached,
5
exaggerated central effect. Epicritic sensations (fine sensations, which
include fine touch, proprioceptive sensations and intermediate grades
of temperature) are permanently and irreversibly lost.
MOTOR EFFECTS
The damage of the ventrolateral nucleus (main motor nucleus) leads to loss
of cereberllar and basal ganglion control on the motor cortical areas. There is
hemiparesis (weakness of the muscles), hemiataxia and choreoathetoid
movements.
SENSORY FUNCTIONS OF THE CEREBRAL CORTEX
The cerebral cortex is the highest center for conscious perception of fine
sensations. Crude sensations such as slow pain, temperature and crude
touch can be perceived at a lower level in the thalamus. Somatic
sensations are perceived in the parietal lobe, visual sensations are
perceived in the occipital lobe and auditory sensations in the temporal lobe.
There are three somatic sensory areas in the cerebral cortex;
The primary somatic sensory area (SI), the secondary somatic
sensory area (SII) and the somatic sensory association area.
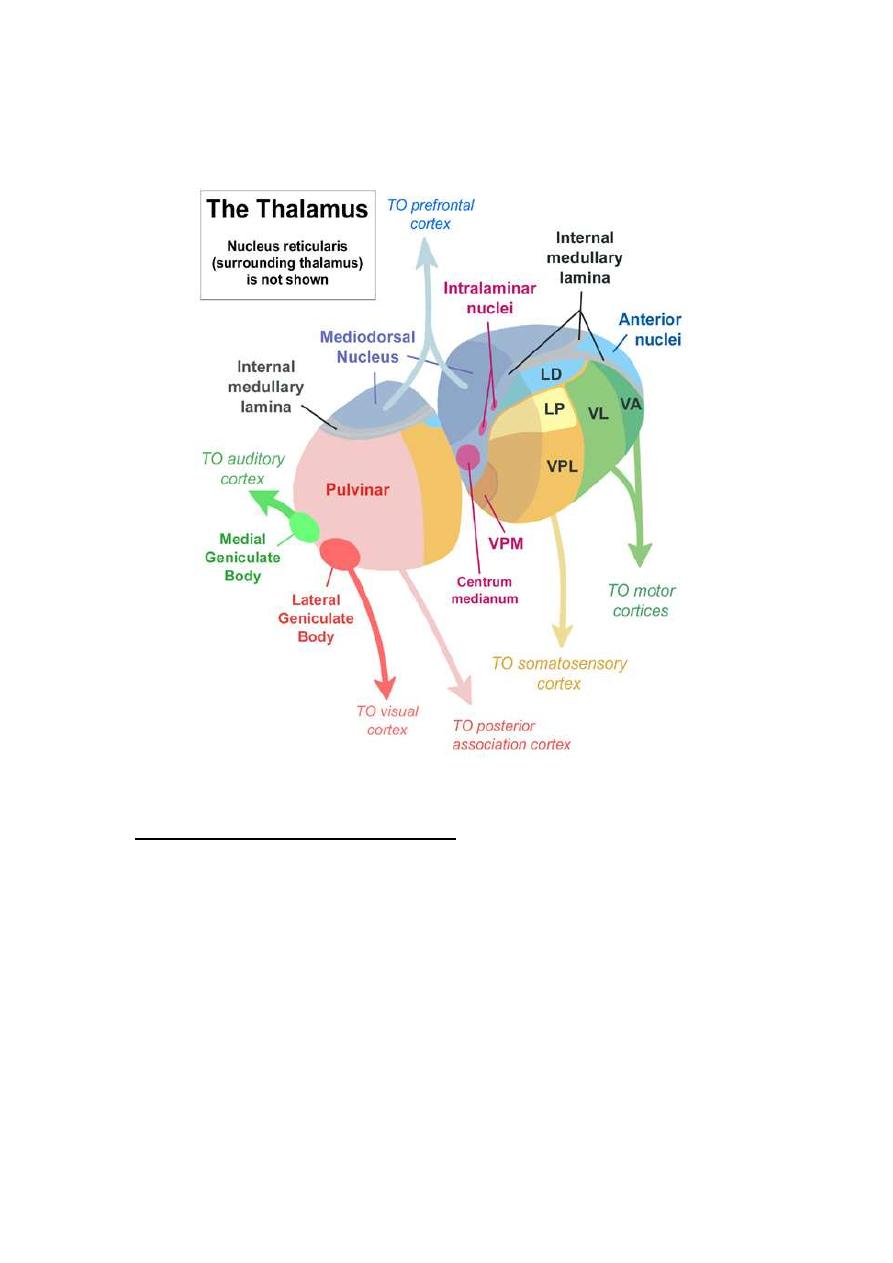
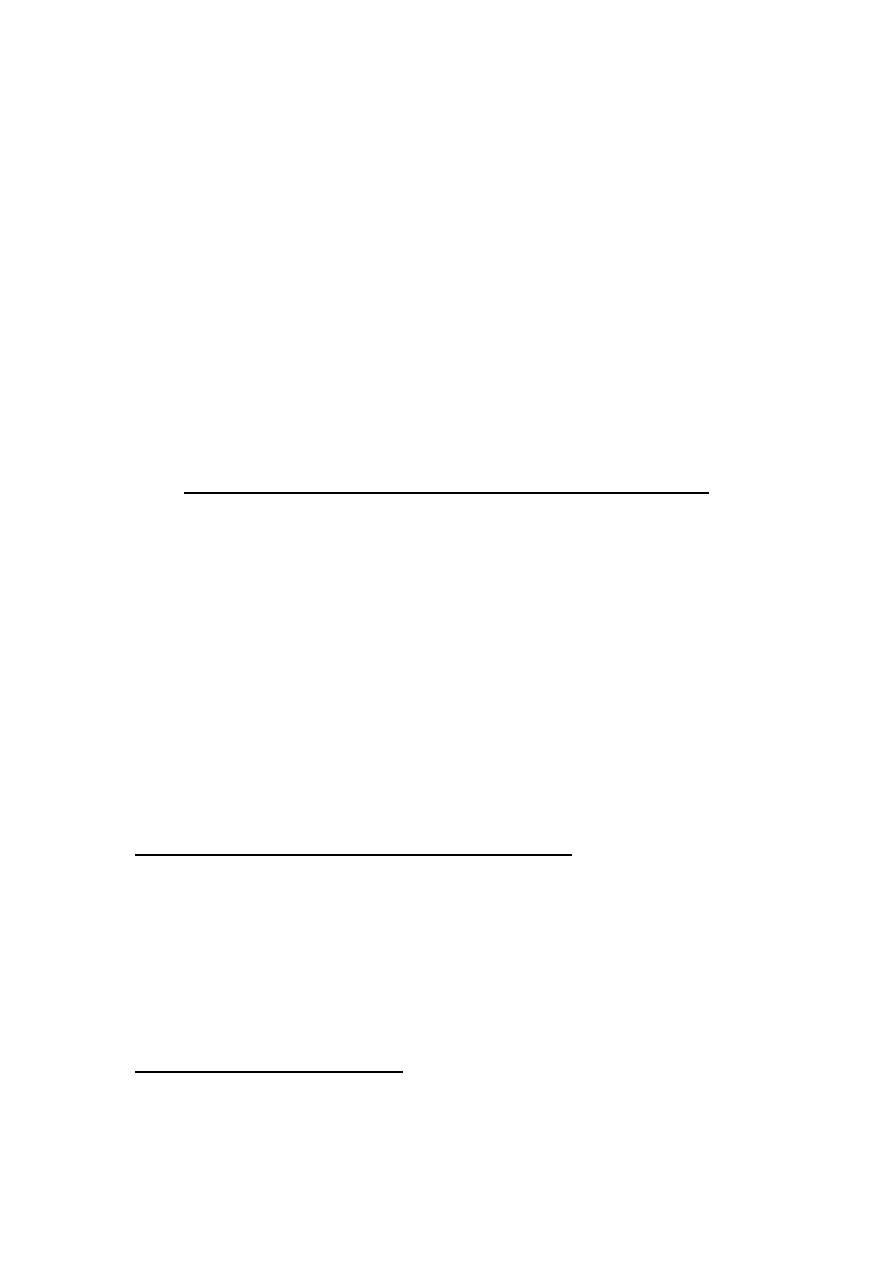
THE PRIMARY SOMATIC SENSORY AREA (SI):
This area is located in the post central gyrus of the parietal lobe
(Brodmann areas 3, 1 and 2) (Fig. 7-1). It receives projection fibers from
the ventrobasal complex of the thalamus (VPLN and VPMN).
In this area, there are the final sensory neurons of the somatic sensory
pathways of fine sensations.
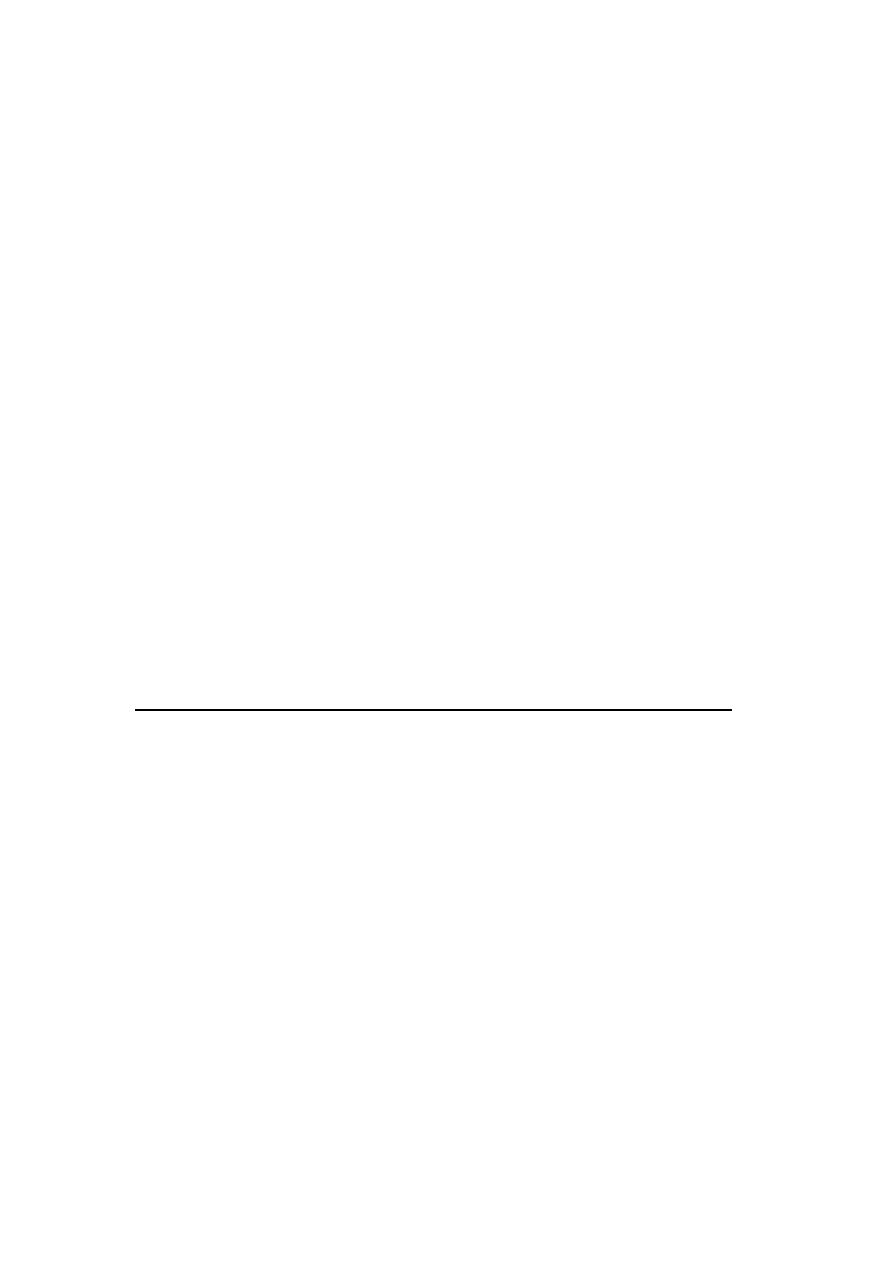
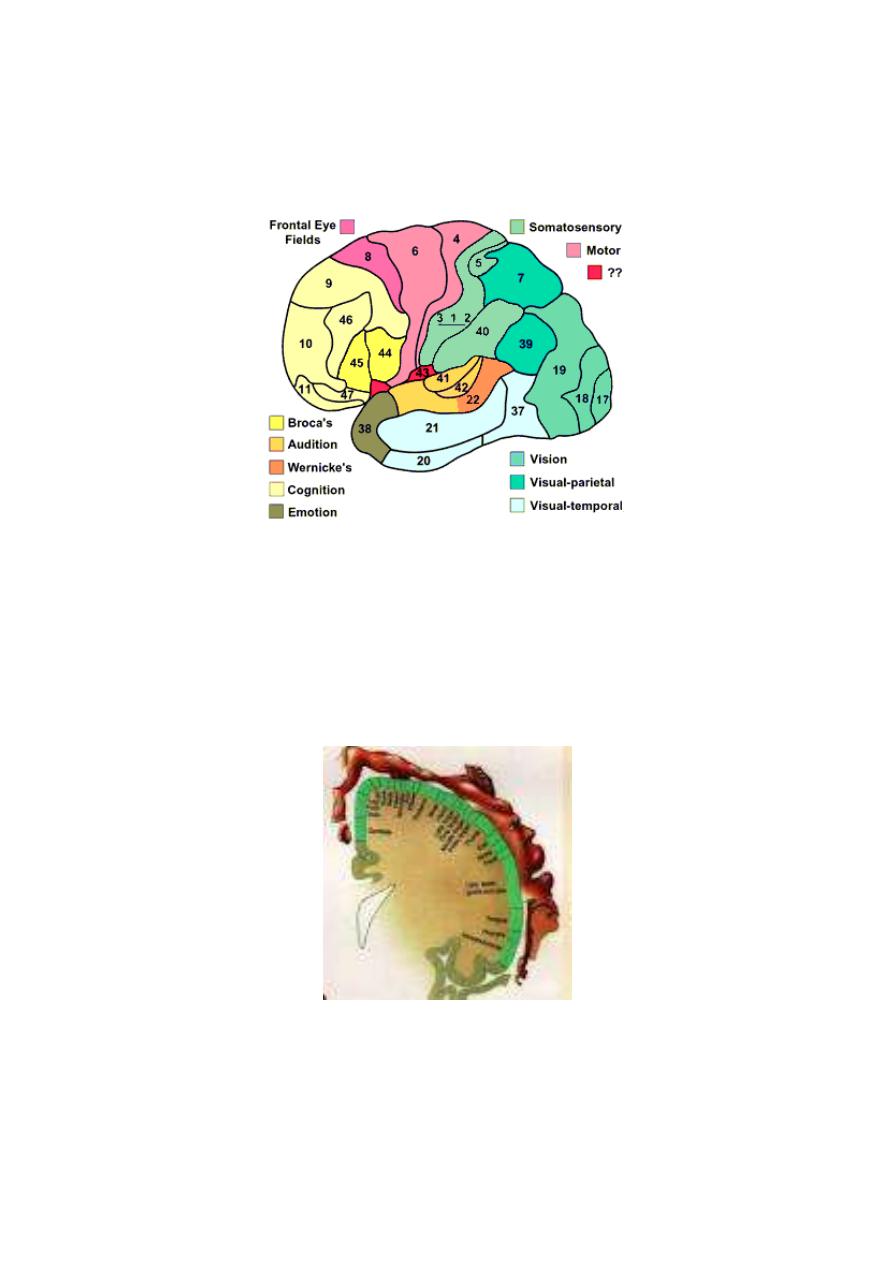
BODY REPRESENTATION: It is crossed and inverted representation
(Fig. 7-2). The upper half of the face is bilaterally represented.
Crossed representation means that each half of the body is represented on the
6
contralateral cerebral hemisphere.
Inverted representation means that upper parts of the body are represented in the
lower part of the cortex and lower parts of the body in upper part of the cortex.
Figure 7-1: Map of Brodmann areas of the cerebral cortex
.
The area of representation of each part is proportional to the number of
receptors in this part, not to its size, e.g. the lips and thumb are
represented by relatively large areas, whilst the trunk is represented by
relatively small area.
Figure 7 - 2: Body representation in the postcentral sensory gyrus
Cells in the sensory cortex are arranged in columns projecting inwards from
the surface. Points in the cortex that represent a certain area of the body
contain several columns each column is specialized in perception of a
7
specific sensory modality. So, modality representation is included within
the topographic representation.
Topographic areas of representation are not permanent or unchangeable,
but can be changed and modified so if a finger is amputated, the cortical
representation of the neighboring fingers creep into the area of the
amputated finger.
FUNCTIONS: The primary somatic sensory area is essential for the
perception of:
1. Fine touch sensation, i.e. tactile localization and discrimination.
2. Localization of pain and temperature sensations, SI is not essential for
the perception of pain and temperature sensations, it is only needed for their
accurate localization.
3. Intensity discrimination of different stimuli.
4. Texture of material.
5. Proprioception; static and dynamic.
SI area projects connection fibers to the secondary somatic sensory area (SII)
and to the somatic sensory association area for interpreting the meaning and
significance of the sensory information; e.g stereognosis.
THE SECONDARY SOMATIC SENSORY AREA (SII)
LOCATION: In the supramarginal gyrus (Brodmann area 40), behind the
lower part of SI.
BODY REPRESENTATION: Bilateral representation with poor
topographic representation. The head area is generally in the anterior part
and the leg area in the posterior part.
SII receives connection fibers which convey input signals from SI, the visual
and auditory cortical sensory areas, and the thalamic nuclei on both sides of
the body.
FUNCTIONS: SII is a potentiator of SI. It cannot work independent of SI.
8
SI, however, can carry out its functions without SII. So, SI can work
without SII, but the opposite is not true.
SOMATIC SENSORY ASSOCIATION AREA
(SOMATIC INTERPRETATIVE AREA)
LOCATION: In the posterior parietal cortex (Brodmann areas 5 and 7),
behind SI and above SII.
CONNECTIONS: It receives sensory signals from SI, SII, and the thalamus.
FUNCTIONS:
1. It combines all sensory signals to give meaning to the complex sensory
input.
2. Stereognosis. This area is the center of stereognosis.
3. Spatial orientation of the body with its surroundings. The person
recognizes the position of each part of the body relative to other
parts and to the surrounding objects.
4. Memory. This area is the memory store of previous sensory
experience. Stimulation of this area produces sensory hallucinations.
EFFECT OF
LESION
: A lesion in the somatic sensory association area
results in:
1. Astereognosis, i.e. inability to identify objects by their touch, shape,
weight and texture.
2. Autotopagnosia, loss of recognition of part or whole contralateral side
of the body. The patient does not acknowledge the existence of the
affected part and fails to include it in planning of voluntary movement. E.g.
he does not swing the arm of the affected side during walking, he puts
clothes on one side of the body and ignores the other or he shaves only one
side of his beard.
3. Impaired memory and decreased intelligence.