SURGERY
LEC. 22
Dr. Yasser Naif Qassim
Lec. 2
GRAFTS
Tues. 14 / 4 / 2015
DONE BY : Ali Kareem
مكتب اشور لالستنساخ
2014 – 2015

GRAFTS Dr. Yasser Naif Qassim
14-4-2015
2
GRAFTS
3
rd
year Dr. Yasser Naif Qassim
Plastic surgery
…………………………………………………………………...
A graft is a segment of tissue that is completely detached from its original site and
blood supply(donor site) and transferred to another new site(recipient site),hence
its survival depends on the blood supply of the recipient site.
Classifications:
1-According to the source:
a.Auto(homo) graft:taken from the same individual.
b.Allo(hetero) graft:taken from another individual but of the same species.
c.Xenograft:taken from another species(e.g. animals like pigs).
2-According to composition:
a.Simple graft:composed of a single type of tissue e.g. skin only, tendon only,
nerve only,…etc.
b.Composite graft:composed of more than one type of tissue e.g.
chondrocutaneous graft(skin and cartilage).
Skin graft:
A piece of skin of variable thickness transferred from the donor site to resurface
the recipient site when the primary wound closure can not be achieved due to
shortage of adjacent tissues for a reason or another.They could be:
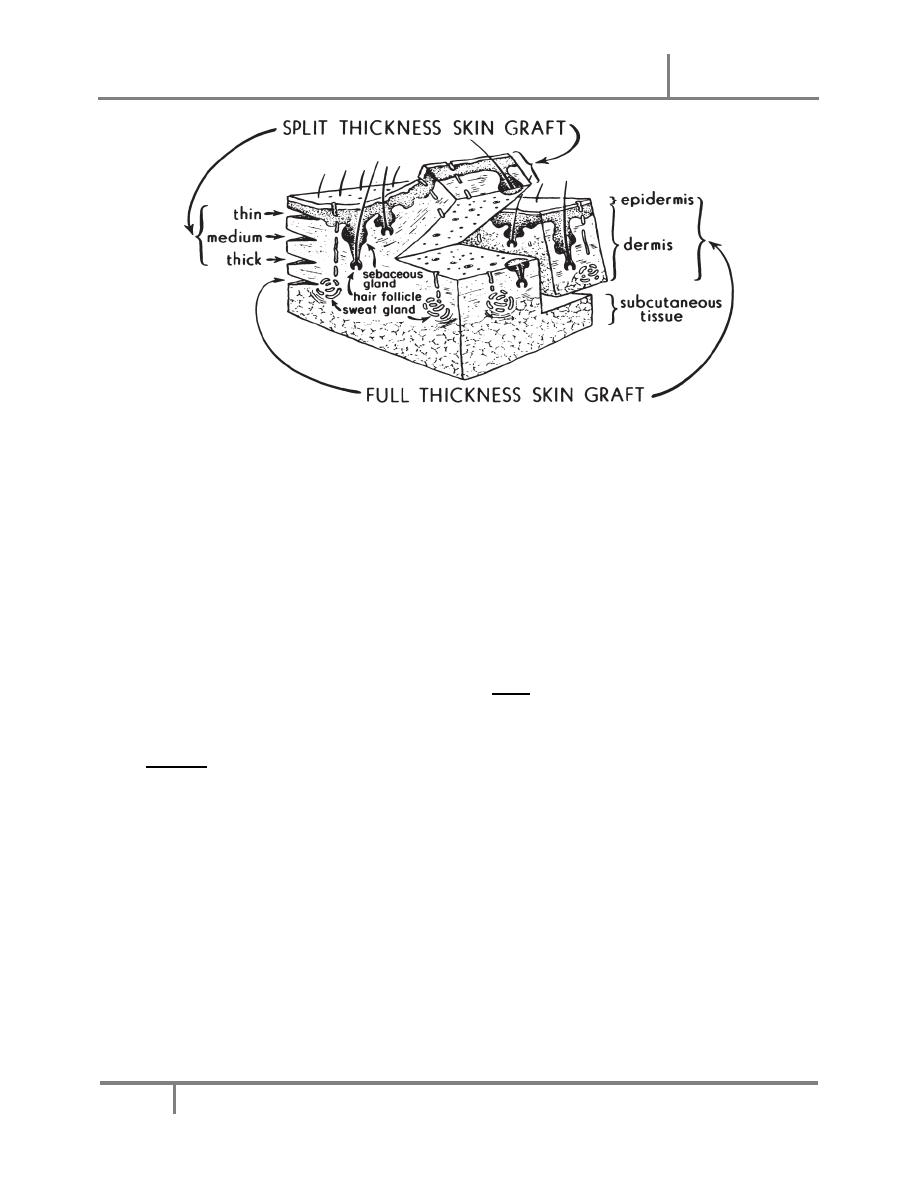
1. Full thickness (FTSGs): consist of full thickness skin (epidermis and dermis)
2. Split thickness (STSGs):consist of the epidermis and varying degrees of
dermis. They can be described as thin, intermediate,or thick according to the
amount of dermis.
FTSG provide better texture and colour matching.The sensation and the presence
of skin appendages are also better than STSG.
GRAFTS Dr. Yasser Naif Qassim
14-4-2015
3
All skin grafts undergo two contractions:
1-Primary contraction: immediately after removal from the donor site as a result
of the elastin in the dermis
→ thick graft has more primary contraction than thin
grafts.
2-Secondary contraction: after revascularization in the final recipient location.It
involves contraction of the healed graft and is probably a result of myofibroblast
activity.
Skin Graft Adherence:
There are two phases of graft adherence. The first is fibrinous deposition and
adhesion, begins with placement of the graft on the recipient bed,lasting about 72
hours.
The second involves the ingrowth of fibrous tissue and vessels into the graft.
Survival of skin grafts:
Skin grafts survive (take) by 3 mechanisms:
a. Serum imbibition:In the first 24-48 hours after grafting,skin grafts passively
absorb the nutrients in the wound bed by diffusion.
b. Inosculation:By day 3, the cut ends of the vessels on the underside of the
dermis begin to form connections with those of the wound bed
c. Angiogenesis:By day 5-7, new blood vessels grow into the graft and the graft
becomes vascularized.

GRAFTS Dr. Yasser Naif Qassim
14-4-2015
4
Hence,the requirements for graft survival are:
1-well vascularized bed
→any avascular recipient site like denuded bone(without
periostium),denuded cartilage(without perichondrium),denuded tendon(without
paratenon) are contraindicated for skin grafts.
2-Contact with the recipient bed
→any seroma,hematoma,pus,and lose graft
application to the bed can lead to graft failure.
3-Clean non infected recipient site
→heavy infection especially with streptococci
can lead to graft failure.
Harvesting skin grafts:
1-STSG
→by free hand knives (e.g. Humby knife, Blair knife, and a simple
scalpel) or by power-driven dermatomes (electric Brown dermatome ,air Zimmer
dermatome and Padgett dermatome).
2-FTSG
→by a simple scalpel.
Donor Sites:
Split-thickness skin grafts can be taken from any area on the body, including the
scalp,the Popular areas for split-thickness graft harvest include the thigh and trunk.
The donor site of a split-thickness skin graft generally heals by re-epithelialization
in 14-2l days so the dressing which is composed of fine mesh(tull) gauze
impregnated with a lubricant e.g antibiotic ointment is left in place for 2-3 weeks
without changing unless there are features of infection(persistant pain, bad
odour,fever,….).
Full-thickness skin grafts can be taken from the The upper eyelid, postauricular ,
preauricular, supraclavicular, antecubital,volar wrist and groin skin.The donor area
is closed by primary suturing unless the area is large
→ closed by STSG.
Recipient Sites:
The recipient site should be vascular and clean,and the graft is secured in place
using sutures or staples.the first layer of dressing sould be non adherent covered by
dry gauze and bandging.On the face and trunk, the graft is better to be secured to
the recipient bed by tie-over dressing.
The first post-operative inspection of the
skin graft is usually performed between 2–5 days postoperatively.

GRAFTS Dr. Yasser Naif Qassim
14-4-2015
5
Meshed versus sheet skin graft:
Skin grafts can be meshed using scalpel or mesher to increase the surface
area
→large area can be grafted in addition to that there is no or very little chance
for the hematoma or seroma to be collected underneath the meshed graft but they
have pebble appearance(aesthetically less acceptable) and liable to contract on
application to a joint area.
In contrast ,sheet graft provide superior aesthetic appearance and has less liability
for contruction on application on joint area but the risk of development of
hematoma and serome beneath it is more in addition to difficulty in resurfacing
large areas.
Skin graft failure is caused by :
a.Hematoma/seroma — Hematomas and seromas prevent contact of the graft to
the bed and inhibit revascularization. They must be drained by day 3 to ensure
―take‖.It is the most common cause of graft failure.
b.Infection .
c.Poor wound bed — Because skin grafts depend on the underlying vascularity of
the bed, wounds that are poorly vascularized with bare tendons or bone, or because
of radiation, will not support a skin graft.
d.Sheer forces separate the graft from the bed and prevent the contact necessary
for revascularization and subsequent ―take‖.
e.Upside down application of the graft.
Cultured skin graft:
Mainly used to cover large defect when the autologus skin is insufficient e.g.
extensive burns.Cultured skin grafts composed mainly of epithelium
→non
satisfactory mechanical nor aesthetic coverage.
Done by
Ali Kareem