Department of microbiology-Bacteriology
1
-The Haemophilus and Bordetella Species-
Lecturer: Yasmeen AlBayaa
Objectives:
1- To demonstrate genus Hemophilus and Bordetella and their spp.
2-To determine medically important gram negative rods associated with
respiratory tract Haemophilus influenzae and Bordetella pertussis
3- To predict their pathogenicity, clinical finding, antigenic structure, lab
diagnosis, epidemiology, immunity and treatment.
Genus Haemophilus, Introduction:
Haemo= blood , philus= loving
This is a group of small, gram-negative, pleomorphic bacteria that require enriched
media, usually containing blood or its derivatives, for isolation. Haemophilus
influenzae type b is an important human pathogen; Haemophilus ducreyi, a
sexually transmitted pathogen, causes chancroid; other Haemophilus species are
among the normal flora of mucous membranes and only occasionally cause
disease.
Haemophilus influenza:
Haemophilus influenzae is found on the mucous membranes of the upper
respiratory tract in humans, it can cause problems only when other factors(such as
viral infection or reduced immune function). It is an important cause of meningitis
in children and occasionally causes respiratory tract infections in children and
adults.
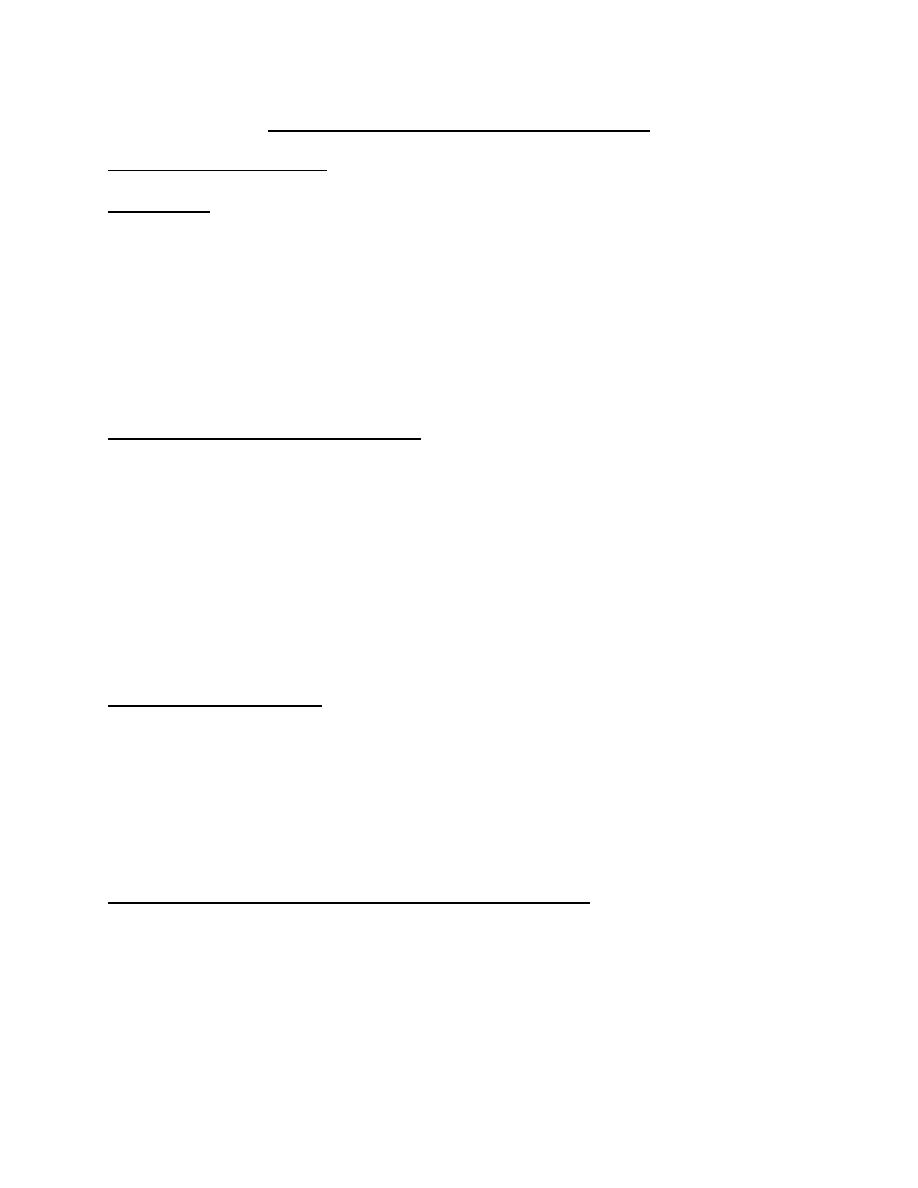
Morphology & Identification of aTypical Organisms:
In specimens from acute infections, the organisms are short (1.5 um) coccoid
bacilli, sometimes occurring in pairs or short chains. In cultures, the morphology
depends both on age and on the medium. At 6–8 hours in rich medium, the small
coccobacillary forms predominate. Later there are longer rods, lysed bacteria, and
very pleomorphic forms. So the m.o. described as pleomorphic m.o.
Department of microbiology-Bacteriology
2
Organisms in young cultures (6–18 hours) on enriched medium have a definite
capsule. The capsule is the antigen used for "typing" H influenzae.
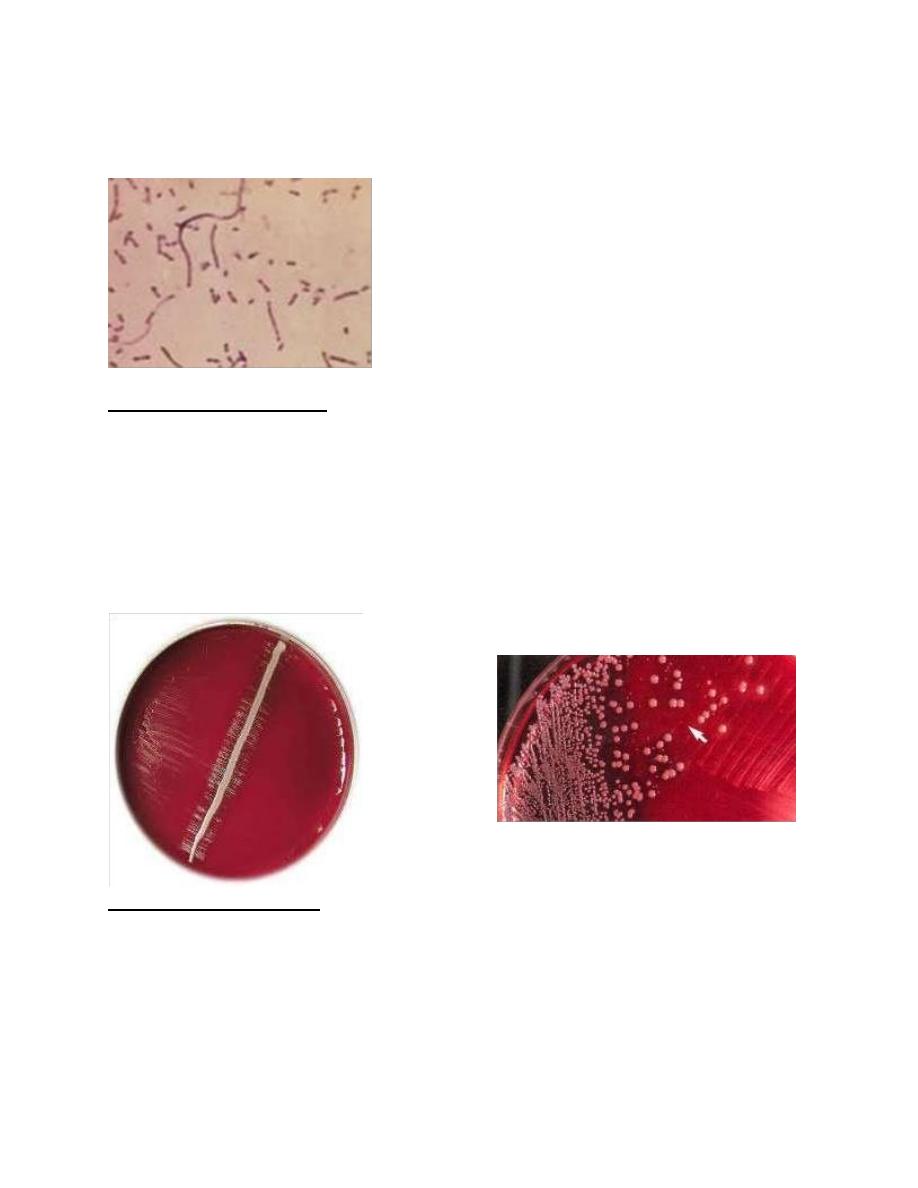
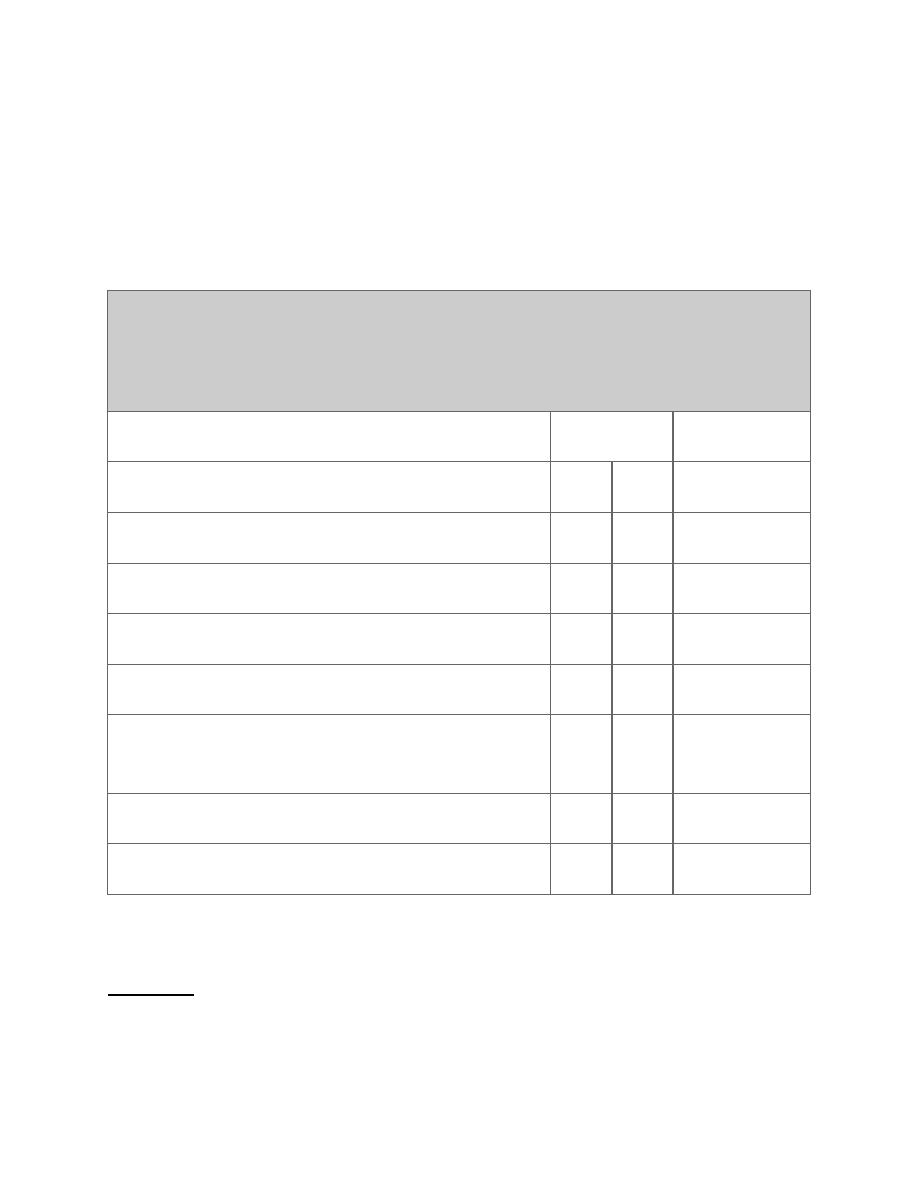
Cultural Characteristics
On chocolate agar, flat, grayish brown colonies with diameters of 1–2 mm are
present after 24 hours of incubation. IsoVitaleX in media enhances growth. H
influenzae does not grow on sheep blood agar except around colonies of
staphylococci ("satellite phenomenon") i.e (it grow in the hemolytic zone of
S.aureus ). H haemolyticus and H parahaemolyticus are hemolytic variants of H
influenzae and H parainfluenzae, respectively.
Growth Characteristics
Identification of organisms of the Haemophilus group depends in part upon
demonstrating the need for certain growth factors called X and V.
Factor X acts physiologically as hemin which is
heat stable needed in the synthesis
of respiratory enzymes like cytochrome oxidase, catalase and peroxidase ; factor V
Department of microbiology-Bacteriology
3
which is (heat labile)
needed for oxidation- reduction system, this factor can be
replaced or provided by nicotinamide adenine nucleotide (NAD) or other
coenzymes . Colonies of staphylococci on sheep blood agar cause the release of
NAD, yielding the satellite growth phenomenon. The requirements for X and V
factors of various Haemophilus species are listed in Table 1. Carbohydrates are
fermented poorly and irregularly.
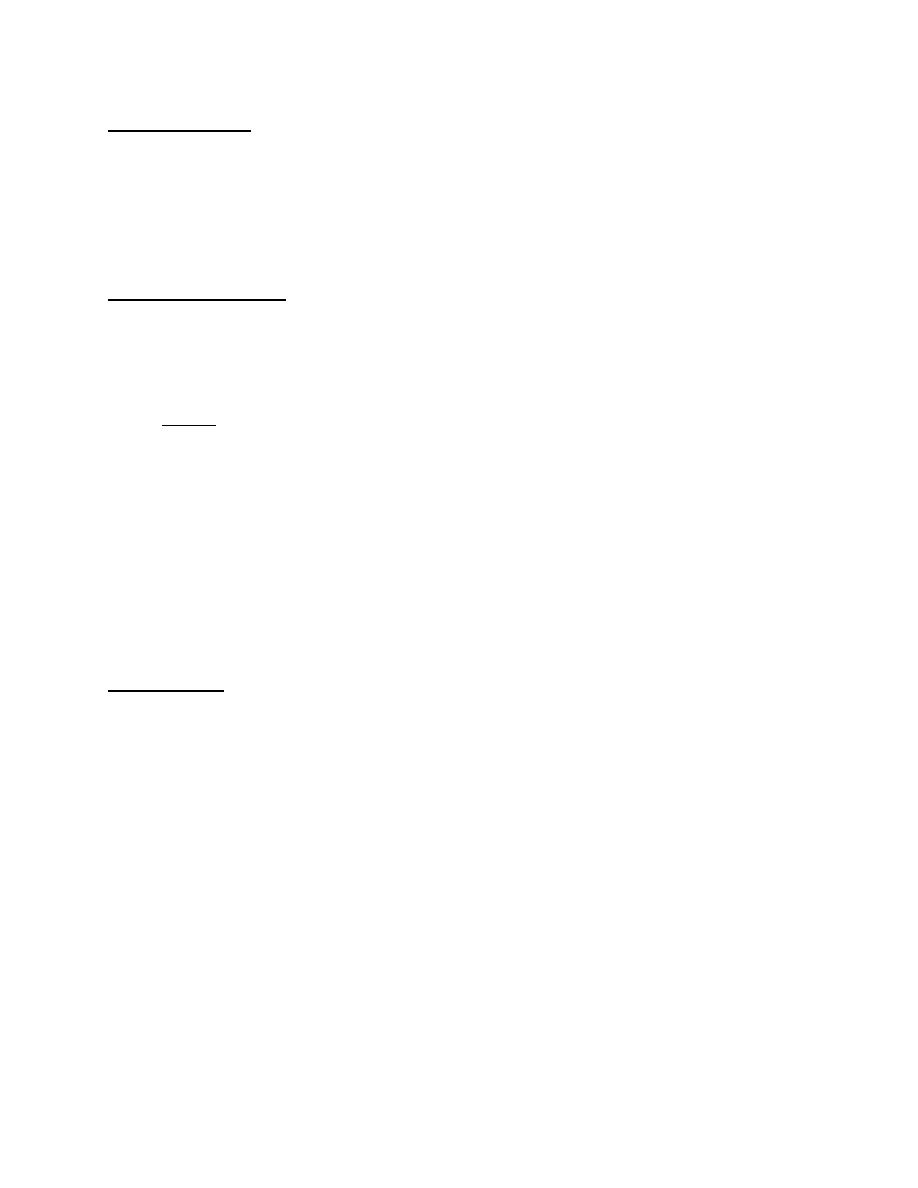
Table 1- Characteristics and Growth Requirements of the Haemophilus Species
Important to Humans
Requires
Species
X
V
Hemolysis
Haemophilus influenzae (H aegyptius)
+
+
–
Haemophilus parainfluenzae
–
+
–
Haemophilus ducreyi
+
–
–
Haemophilus haemolyticus
+
+
+
Aggregatibacter aphrophilus
a
–
–
–
Haemophilus paraphrophaemolyticus
–
+
+
Haemophilus segnis
–
+
–
X, heme; V, nicotinamide-adenine dinucleotide.
a Now called Aggregatibacter.
Variation
In addition to morphologic variation, H influenzae has a marked tendency to lose
its capsule and the associated type specificity.
Department of microbiology-Bacteriology
4
Transformation
Under proper experimental circumstances, the DNA extracted from a given type of
H influenzae is capable of transferring that type specificity to other cells
(transformation). Resistance to ampicillin and chloramphenicol is controlled by
genes on transmissible plasmids.
Antigenic Structure
1- Capsule: Encapsulated H influenzae contains capsular polysaccharides
(MW >150,000) of one of six types (a–f).
2- The capsular antigen of type b is a polyribose-ribitol phosphate (PRP).
Note: Encapsulated H influenzae can be typed by slide agglutination,
coagglutination with staphylococci, or agglutination of latex particles coated
with type-specific antibodies. A capsule swelling test with specific
antiserum is analogous to the quellung test for pneumococci. Typing can
also be done by immunofluorescence. Most H influenzae organisms in the
normal flora of the upper respiratory tract are not encapsulated.
3- The somatic antigens of H influenzae consist of outer membrane
proteins. Lipooligosaccharides (endotoxins) share many structures with
those of neisseriae.
Pathogenesis
H influenzae produces no exotoxin. The non-encapsulated organism is a regular member
of the normal respiratory microbiota of humans. The capsule is antiphagocytic in the
absence of specific anticapsular antibodies. The polyribose phosphate capsule of type b
H influenzae is the major virulence factor. Various strains of Haemophilus influenzae
produce IgA protease that can digest serum IgA thus facilitate attachment to the
respiratory mucosa.
-Type b H influenzae causes meningitis, pneumonia and empyema, epiglottitis,
cellulitis, septic arthritis, and occasionally other forms of invasive infection. The carrier
rate in the upper respiratory tract for H influenzae type b is 2–4%.
-Nontypeable H influenzae tends to cause chronic bronchitis, otitis media, sinusitis, and
conjunctivitis following breakdown of normal host defense mechanisms. The carrier rate
for nontypeable H influenzae is 50–80% or higher.
Department of microbiology-Bacteriology
5
-The carrier rate for the encapsulated types a and c–f is low (1–2%), and these capsular
types rarely cause disease.
Although type b can cause chronic bronchitis, otitis media, sinusitis, and conjunctivitis,
it does so much less commonly than nontypeable H influenzae. Similarly, nontypeable H
influenzae only occasionally causes invasive disease (about 5% of cases).
The blood of many persons over age 3–5 years is bactericidal for H influenzae, and
clinical infections are less frequent in such individuals. However, bactericidal antibodies
have been absent from 25% of adults in the United States, and clinical infections have
occurred in adults.
Clinical Findings
-H influenzae type b enters by way of the respiratory tract. There may be local extension
with involvement of the sinuses or the middle ear.
-H influenzae type b and pneumococci are two of the most common etiologic agents of
bacterial otitis media and acute sinusitis. The organisms may reach the bloodstream
and be carried to the meninges or, less frequently, may establish themselves in the joints
to produce septic arthritis.
-Prior to the use of the conjugate vaccine, H influenzae was the most common cause of
bacterial meningitis in children age 5 months to 5 years in the United States.
Clinically, it resembles other forms of childhood meningitis, and diagnosis rests on
bacteriologic demonstration of the organism.
Pneumonitis and epiglottitis due to H influenzae may follow upper respiratory tract
infections in small children and old or debilitated people. Adults may have bronchitis or
pneumonia due to H influenzae.
Diagnostic Laboratory Tests
Specimens: Specimens consist of nasopharyngeal swabs, pus, blood, and spinal
fluid for smears and cultures.
Direct Identification:
by (immunoflourescent technique or capsular swelling test)
Commercial kits are available for immunologic detection of H influenzae antigens
in spinal fluid. A positive test indicates that the fluid contains high concentrations
of specific polysaccharide from H influenzae type b.
Department of microbiology-Bacteriology
6
Culture: on chocolate agar with X and V factor
Specimens are grown on IsoVitaleX-enriched chocolate agar until typical colonies
appear. H influenzae is differentiated from related gram-negative bacilli by its
requirements for X and V factors and by its lack of hemolysis on blood agar .
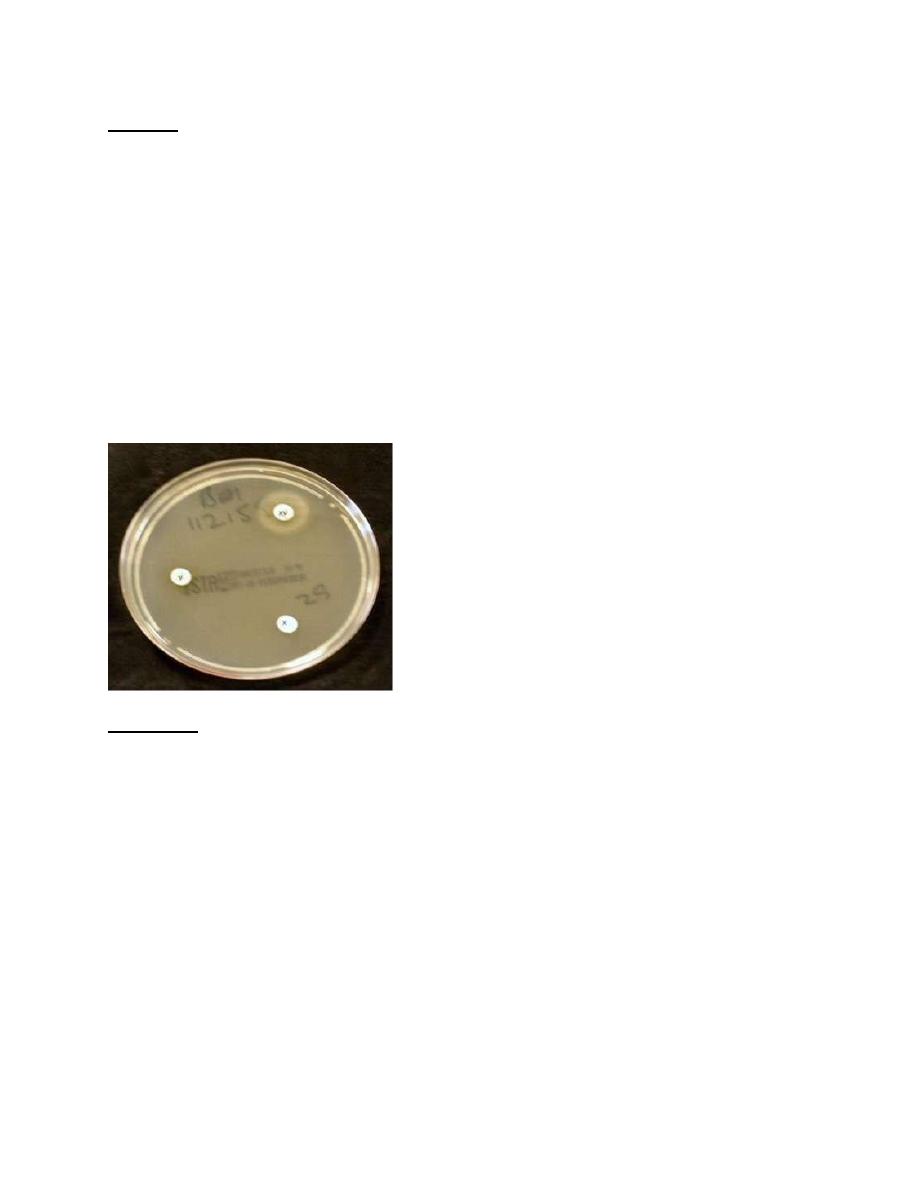
Tests for X (heme) and V (nicotinamide-adenine dinucleotide) factor requirements
can be done in several ways. The Haemophilus species that require V factor grow
around paper strips or disks containing V factor placed on the surface of agar that
has been autoclaved before the blood was added (V factor is heat-labile).
Alternatively, a strip containing X factor can be placed in parallel with one
containing V factor on agar deficient in these nutrients. Growth of Haemophilus in
the area between the strips indicates requirement for both factors.
Immunity
Infants under age 3 months may have serum antibodies transmitted from the
mother. During this time H influenzae infection is rare, but subsequently the
antibodies are lost. Children often acquire H influenzae infections, which are
usually asymptomatic but may be in the form of respiratory disease or meningitis.
H influenzae has been the most common cause of bacterial meningitis in children
from 5 months to 5 years of age. By age 3–5 years, many unimmunized children
have naturally acquired anti-PRP antibodies that promote complement-dependent
bactericidal killing and phagocytosis. Immunization of children with H influenzae
type b conjugate vaccine induces the same antibodies.
There is a correlation between the presence of bactericidal antibodies and
resistance to major H influenzae type b infections. However, it is not known
Department of microbiology-Bacteriology
7
whether these antibodies alone account for immunity. Pneumonia or arthritis due to
H influenzae can develop in adults with such antibodies.
Treatment
The mortality rate of untreated H influenzae meningitis may be up to 90%. Many
strains of H influenzae type b are susceptible to ampicillin, but up to 25% produce
-lactamase under control of a transmissible plasmid and are resistant. Essentially
all strains are susceptible to the third-generation
cephalosporins. Cefotaxime
given
intravenously gives excellent results. Prompt diagnosis and antimicrobial therapy
are essential to minimize late neurologic and intellectual impairment. Prominent
among late complications of H influenzae type b meningitis is the development of
a localized subdural accumulation of fluid that requires surgical drainage.
Epidemiology, Prevention, & Control
Encapsulated H influenzae type b is transmitted from person to person by the
respiratory route. H influenzae type b disease can be prevented by administration
of Haemophilus b conjugate vaccine to children. The series consists of three doses
at 2, 4, and 6 months of age or two doses given at 2 and 4 months. An additional
booster dose is given sometime between 12 and 15 months of age. Widespread use
of H influenzae type b vaccine has reduced the incidence of H influenzae type b
meningitis in children by over 95%. The vaccine reduces the carrier rates for H
influenzae type b.
Contact with patients suffering from H influenzae clinical infection poses little risk
for adults but presents a definite risk for nonimmune siblings and other
nonimmune children under age 4 years who are close contacts. Prophylaxis with
rifampin is recommended for such children.
Haemophilus aegyptius : Important in acute conjunctivitis which is highly
infectious called Koch week bacilli.
Aggregatibacter aphrophilus: Found in normal flora of mouth, it is important in
endocarditis and pneumonia.
Haemophilus ducreyi : causes chancroid i.e. soft chancher which is STD
(sexually transmitted disease) with irregular ulcer on genitalia, swelling, tender,
Department of microbiology-Bacteriology
8
lymphadenopathy, it should be differentiated from other STD e.g Syphlis, herpes
simplex. Diagnosis: scraping from ulcer, culture. Treatment:-cotrimoxazol,
erythromycin.
Other Haemophilus Species:
Haemophilus haemolyticus is the most markedly hemolytic organism of the
group in vitro; it occurs both in the normal nasopharynx and in association with
rare upper respiratory tract infections of moderate severity in childhood.
Haemophilus parainfluenzae resembles H influenzae and is a normal inhabitant
of the human respiratory tract; it has been encountered occasionally in infective
endocarditis and in urethritis.
The Bordetellae
Introduction
There are several species of Bordetella. Bordetella pertussis, a highly
communicable and important pathogen of humans, causes whooping cough
(pertussis). Bordetella parapertussis can cause a similar disease (mild).
Bordetella bronchiseptica (Bordetella bronchicanis) causes diseases in animals
such as kennel cough in dogs and snuffles in rabbits, and only occasionally causes
respiratory disease and bacteremia in humans, primarily in immunocompromised
hosts.
Bordetella pertussis:
Morphology & Identification of Typical Organisms:
The organisms are gram-negative coccobacilli resembling H influenzae. With
toluidine blue stain, bipolar metachromatic granules can be demonstrated. A
capsule is present.
Culture: Primary isolation of B pertussis requires enriched media. Bordet-
Gengou medium (potato-blood-glycerol agar) that contains penicillin G, 0.5
g/mL, can be used; however, a charcoal-containing medium similar to that used for
Legionella pneumophila is preferable. The plates are incubated at 35–37°C for 3–7
days in a moist environment (eg, a sealed plastic bag). The small, faintly staining
Department of microbiology-Bacteriology
9
gram-negative rods are identified by immunofluorescence staining. B pertussis is
nonmotile.
Growth Characteristics
The organism is a strict aerobe and forms acid but not gas from glucose and
lactose. It does not require X and V factors on subculture. Hemolysis of blood-
containing medium is associated with virulent B pertussis.
Variation
When isolated from patients and cultured on enriched media, B pertussis is in the
hemolytic and pertussis toxin-producing virulent phase. There are two
mechanisms for B pertussis to shift to nonhemolytic, nontoxin-producing
avirulent forms. Reversible phenotypic modulation occurs when B pertussis is
grown under certain environmental conditions (eg, 28°C versus 37°C, the presence
of MgSO4 , etc). Reversible phase variation follows a low-frequency mutation in
the genetic locus that controls the expression of the virulence factors. It is possible
that these mechanisms play a role in the infectious process, but such a role has not
been demonstrated clinically.
Antigenic Structure
1- filamentous hemagglutinin mediates adhesion to ciliated epithelial cells.
2- Pertussis toxin promotes lymphocytosis, sensitization to histamine, and
enhanced insulin secretion.
Note:The filamentous hemagglutinin and pertussis toxin are secreted proteins
and are found outside of the B pertussis cells.
3- Adenylate cyclase toxin, dermonecrotic toxin, and hemolysin
4- The tracheal cytotoxin inhibits DNA synthesis in ciliated cells.
Department of microbiology-Bacteriology
10
Note: Pili probably play a role in adherence of the bacteria to the ciliated
epithelial cells of the upper respiratory tract. The lipopolysaccharide in the cell
wall may also be important in causing damage to the epithelial cells of the upper
respiratory tract.
Pathogenesis:
B pertussis survives for only brief periods outside the human host. There are no
vectors. Transmission is largely by the respiratory route from early cases and
possibly via carriers. The organism adheres to and multiplies rapidly on the
epithelial surface of the trachea and bronchi and interferes with ciliary action. The
blood is not invaded. The bacteria liberate the toxins and substances that irritate
surface cells, causing coughing and marked lymphocytosis. Later, there may be
necrosis of parts of the epithelium and polymorphonuclear infiltration, with
peribronchial inflammation and interstitial pneumonia. Secondary invaders like
staphylococci or H influenzae may give rise to bacterial pneumonia.
Clinical Findings : (3 stages)
After an incubation period of about 2 weeks, the "catarrhal stage" develops, with
mild coughing and sneezing. During this stage, large numbers of organisms are
sprayed in droplets, and the patient is highly infectious but not very ill. During the
"paroxysmal" stage, the cough develops its explosive character and the
characteristic "whoop" upon inhalation. This leads to rapid exhaustion and may be
associated with vomiting, cyanosis, and convulsions. The "whoop" and major
complications occur predominantly in infants; paroxysmal coughing predominates
in older children and adults. The white blood count is high (16,000–30,000/L),
with an absolute lymphocytosis. Convalescence stage is slow. B pertussis is a
common cause of prolonged (4–6 weeks) cough in adults. Rarely, whooping cough
is followed by the serious and potentially fatal complication of encephalitis.
Several types of adenovirus and Chlamydia pneumoniae can produce a clinical
picture resembling that caused by B pertussis.
Diagnostic Laboratory Tests
Specimens: A saline nasal wash is the preferred specimen. Nasopharyngeal
swabs or cough droplets expelled onto a "cough plate" held in front of the
Department of microbiology-Bacteriology
11
patient's mouth during a paroxysm are sometimes used but are not as good as the
saline nasal wash.
Direct Fluorescent Antibody Test:
immunoflorescent assay
The fluorescent antibody (FA) reagent can be used to examine nasopharyngeal
swab specimens. However, false-positive and false-negative results may occur; the
sensitivity is about 50%. The FA test is most useful in identifying B pertussis after
culture on solid media.
Culture
The saline nasal wash fluid is cultured on solid medium agar
(Bordet-Gengou
medium).
The antibiotics in the media tend to inhibit other respiratory flora but
permit growth of B pertussis. Organisms are identified by immunofluorescence
staining or by slide agglutination with specific antiserum.
Polymerase Chain Reaction
PCR is the most sensitive method to diagnosis pertussis. Primers for both B
pertussis and B parapertussis should be included. When available, the PCR test
should replace the direct fluorescent antibody tests.
Serology
Serologic tests on patients are of little diagnostic help because a rise in
agglutinating or precipitating antibodies does not occur until the third week of
illness. A single serum with high titer antibodies may be helpful in diagnosing the
cause of a long-term cough, one of several weeks' duration.
Immunity
Recovery from whooping cough or immunization is followed by immunity. Second
infections may occur but are mild; reinfections occurring years later in adults may
be severe. It is probable that the first defense against B pertussis infection is the
antibody that prevents attachment of the bacteria to the cilia of the respiratory
epithelium.
Department of microbiology-Bacteriology
12
Treatment
B pertussis is susceptible to several antimicrobial drugs in vitro. Administration of
erythromycin during the catarrhal stage of disease promotes elimination of the
organisms and may have prophylactic value. Treatment after onset of the
paroxysmal phase rarely alters the clinical course. Oxygen inhalation and sedation
may prevent anoxic damage to the brain.
Prevention
Every infant should receive three injections of pertussis vaccine during the
first year of life followed by a booster series for a total of five doses. There
are multiple acellular pertussis vaccines licensed in the United States and
elsewhere. Use of these vaccines is recommended because it
has few side
effects than the killed vaccine (whole cell vaccine) that contain inactivated
organism
(pertussis toxin) that used in the past.
The acellular vaccines
that contain purified proteins from the organism
(pertussis toxoid) have at least two of the following antigens: inactivated
pertussis toxin, filamentous hemagglutinin, fimbrial proteins, and pertactin.
Pertussis vaccine is usually administered in combination with toxoids of
diphtheria and tetanus (DTaP). Five doses of pertussis vaccine are recommended
prior to school entry. The usual schedule is administration of doses at 2, 4, 6, and
15–18 months of age and a booster dose at 4–6 years of age. In 2005, it was
recommended by the Advisory Committee on Immunization Practices that all
adolescents and adults receive a single booster dose of tetanus-diphtheria-acellular
pertussis (Tdap) to replace the booster dose of tetanus and diphtheria toxoids alone
(Td). Prophylactic administration of erythromycin for 5 days may also benefit
unimmunized infants or heavily exposed adults.
Epidemiology & Control
Whooping cough is endemic in most densely populated areas worldwide and also
occurs intermittently in epidemics. The source of infection is usually a patient in
the early catarrhal stage of the disease. Communicability is high, ranging from
30% to 90%. Most cases occur in children under age 5 years; most deaths occur in
the first year of life. Control of whooping cough rests mainly on adequate active
immunization of all infants.
Department of microbiology-Bacteriology
13
Bordetella parapertussis: This organism may produce a disease similar to
whooping cough, but it is generally less severe. The infection is often subclinical.
Bordetella parapertussis grows more rapidly than typical B pertussis and produces
larger colonies. It also grows on blood agar. B parapertussis has a silent copy of the
pertussis toxin gene.
Summary:
1- Hemophilus spp. is a group of small, gram-negative, pleomorphic bacteria
that require enriched media (chocolate agar), usually containing blood;
require X and V factors for their growth.
2- Identification of organisms of the
Haemophilus group or species
depends in
part upon demonstrating the need for certain growth factors called X and V.
3- H influenza is the most common cause of bacterial meningitis in children;
also cause otitis media, acute sinusitis, septic arthritis, pneumonitis,
epiglottitis and upper respiratory tract infections.
4- H influenzae type b disease can be prevented by administration of
Haemophilus b conjugate vaccine to children.
5- Bordetella Spp. is gram-negative coccobacilli resembling H influenzae.
bipolar metachromatic granules can be demonstrated. A capsule is present.
It requires enriched media (Bordet-Gengou medium). It does not require X
and V factors on subculture.
6- Bordetella pertussis causes whooping cough ( pertussis) mostly in
children under 5 years. To prevent the disease; every infant should receive
three injections of pertussis vaccine (DTaP). Followed by a booster series
for a total of five doses.
7- Finally the two medically important gram negative rods associated with
respiratory tract are Haemophilus influenzae and Bordetella pertussis