Dr. Ali A. Allawi
Lec. 2
Electrolyte Balance
Wed
26 / 11 / 2014
Published by : Ali Kareem
5102
-
5102
مكتب اشور لالستنساخ
Electrolyte Balance Dr. Ali A. Allawi
26-11-2014
2
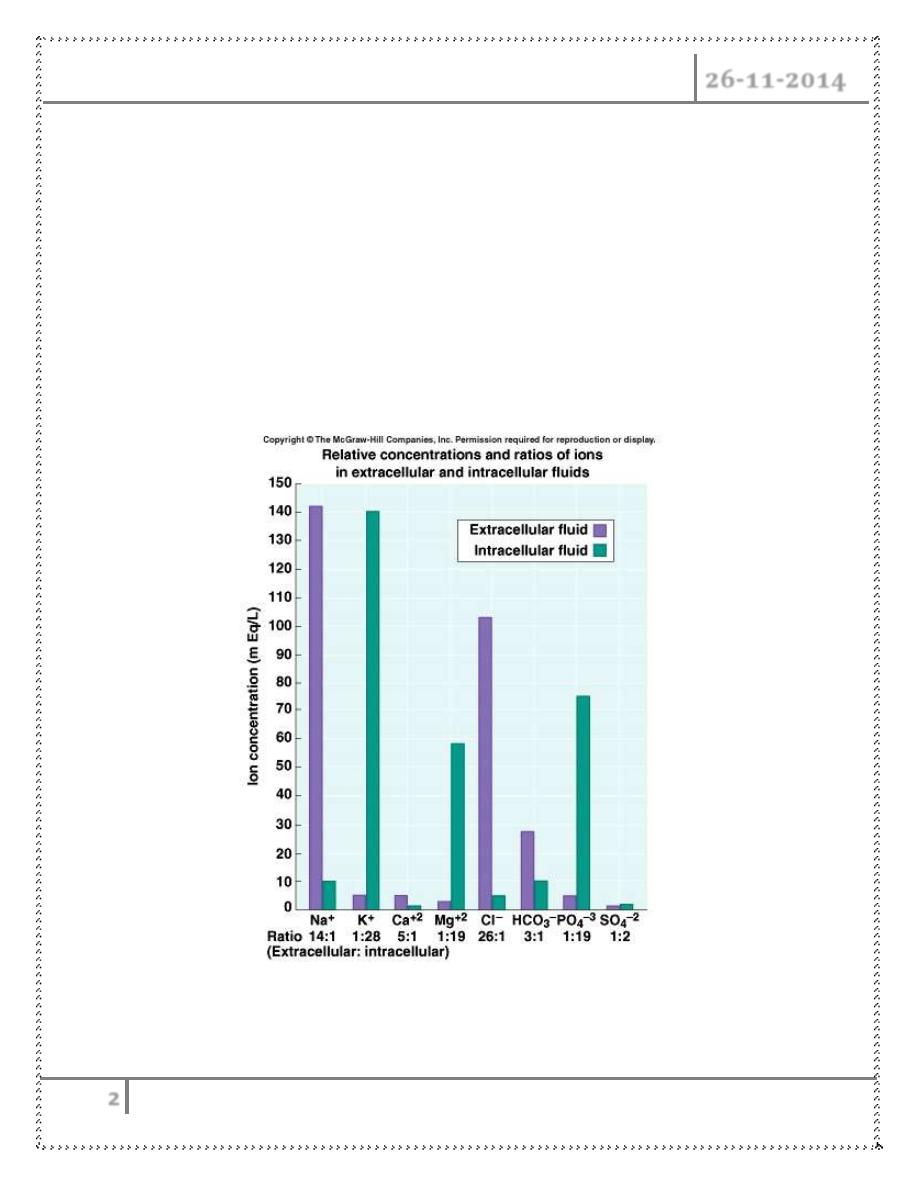
ELECTROLYTE BALANCE
Na
+
(Sodium)
– 90 % of total ECF cations
– 136 -145 mEq / L
– Pairs with Cl
-
, HCO
3
-
to neutralize charge
– Low in ICF
– Most important ion in regulating water balance
– Important in nerve and muscle function
Regulation of Sodium
• Renal tubule reabsorption affected by hormones :
Electrolyte Balance Dr. Ali A. Allawi
26-11-2014
3
– Aldosterone
– Renin/angiotensin
– Atrial Natriuretic Peptide (ANP)
Potassium
– Major intracellular cation
– ICF conc. = 150- 160 mEq/ L
– Resting membrane potential
– Regulates fluid, ion balance inside cell
– pH balance
Regulation of Potassium
• Through kidney
– Aldosterone
– Insulin
Isotonic alterations in water balance
Occur when TBW changes are accompanied by = changes in electrolytes
Loses plasma or ECF
Isotonic fluid loss
– ↓ECF volume, weight loss, dry skin and mucous membranes, ↓ urine
output, and hypovolemia ( rapid heart rate, flattened neck veins, and
normal or ↓ B.P. – shock)
Isotonic fluid excess
– Excess IV fluids
– Hypersecretion of aldosterone
– Effect of drugs – cortisone
Get hypervolemia – weight gain, decreased hematocrit, diluted plasma
proteins, distended neck veins, ↑ B.P.
Can lead to edema (↑ capillary hydrostatic pressure) pulmonary edema and
heart failure
Electrolyte Balance Dr. Ali A. Allawi
26-11-2014
4
Electrolyte imbalances : Sodium
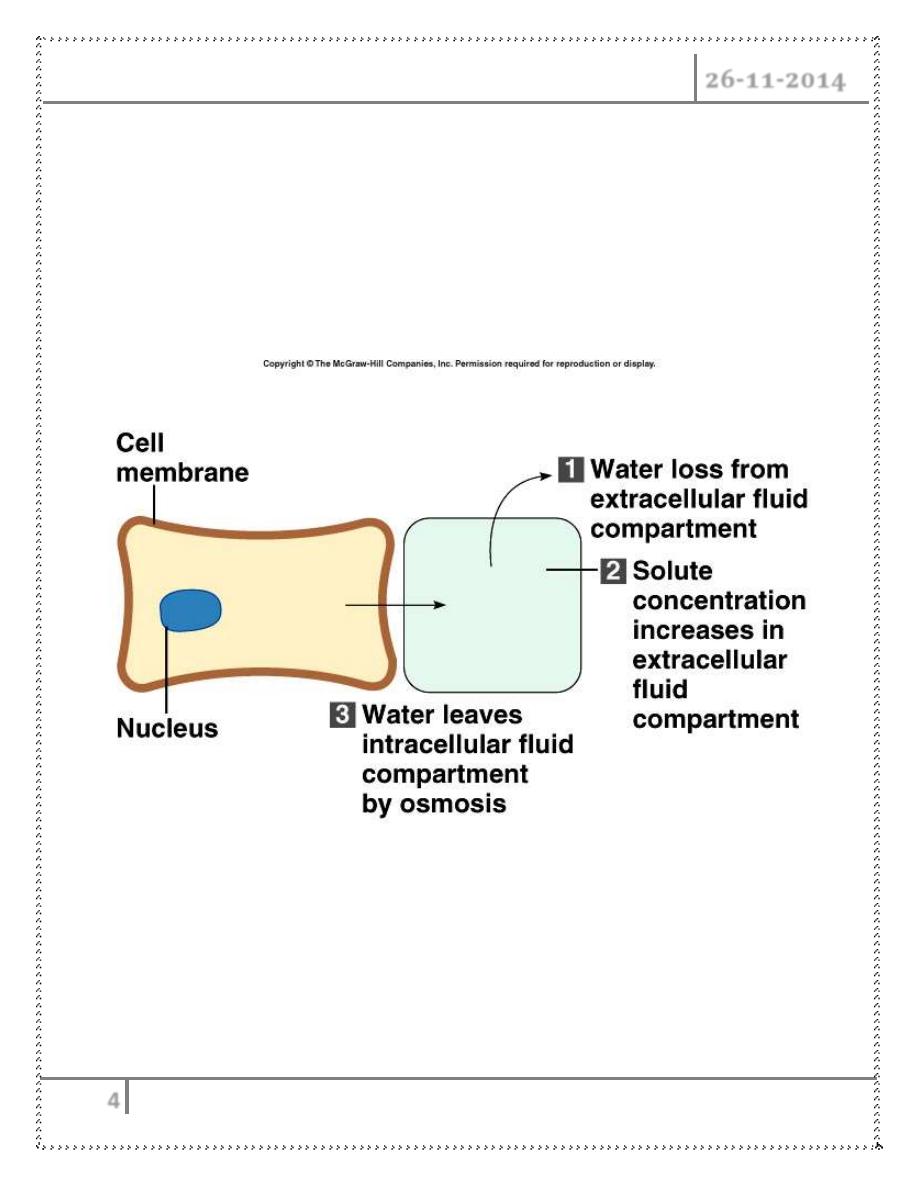
Hypernatremia (high levels of sodium)
– Plasma Na+ > 145 mEq / L
– Due to ↑ Na + or ↓ water
– Water moves from ICF → ECF
– Cells dehydrate
• Hypernatremia Due to :
– Hypertonic IV soln.
– Over secretion of aldosterone
– Loss of pure water
Electrolyte Balance Dr. Ali A. Allawi
26-11-2014
5
o Long term sweating with chronic fever
o
Respiratory infection → water vapor loss
o Diabetes
– polyuria
– Insufficient intake of water (hypodipsia)
Causes of hypernatraemia :
ADH deficiency Diabetes insipidus
latrogenic
Administration of hypertonic sodium solutions
Insensitivity to ADH (nephrogenic diabetes insipidus)
Lithium ,Tetracyclines, Amphotericin B
Acute tubular necrosis
Osmotic diuresis
Total parenteral nutrition
Hyperosmolar diabetic coma PLUS Deficient water intake
Clinical manifestations of Hypernatremia
• Thirst
• Lethargy
• Neurological dysfunction due to dehydration of brain cells
• Decreased vascular volume
Treatment of Hypernatremia
• in ADH deficiency, replace ADH in the form of desmopressin, a stable non-
pressor analogue of ADH
• remember to withdraw nephrogenic drugs where possible and replace water
either orally or, if necessary, intravenously.
• In severe (> 170 mmol/L) hypernatraemia, 0.9% saline (150 mmol/L) should
be used initially. Avoid too rapid a drop in serum sodium concentration; the
aim is correction over 48 hours, as over-rapid correction may lead to
cerebral oedema.
Electrolyte Balance Dr. Ali A. Allawi
26-11-2014
6
• In less severe (e.g. > 150 mmol/L) hypernatraemia, the treatment is 5%
dextrose or 0.45% saline; the latter is obviously preferable in hyperosmolar
diabetic coma. Very large volumes - 5 L a day or more - may need to be
given in diabetes insipidus.
Hyponatremia
– Overall decrease in Na+ in ECF
– Two types: depletional and dilutional
Depletional Hyponatremia
Na+ loss :
– diuretics, chronic vomiting
– Chronic diarrhea
– Decreased aldosterone
– Decreased Na+ intake
• Dilutional Hyponatremia :
o
Renal dysfunction with ↑ intake of hypotonic fluids
o
Excessive sweating→ increased thirst → intake of excessive amounts
of pure water
o Syndrome of Inappropriate ADH (SIADH) or oliguric renal failure,
severe congestive heart failure, cirrhosis all lead to:
Impaired renal excretion of water
o Hyperglycemia – attracts water
Causes of hyponatraemia with normal extracellular volume
Abnormal ADH release
– Vagal neuropathy (failure of inhibition of ADH release)
– Deficiency of adrenocorticotrophic hormone (ACTH) or
glucocorticoids (Addison's disease)
Electrolyte Balance Dr. Ali A. Allawi
26-11-2014
7
– Hypothyroidism
– Severe potassium depletion
Syndrome of inappropriate antidiuretic hormone
Major psychiatric illness
– 'Psychogenic polydipsia‘
– Nonosmotic ADH release?
– Antidepressant therapy
Increased sensitivity to ADH
– Chlorpropamide, Tolbutamide
ADH-like substances
– Oxytocin
– Desmopressin
Unmeasured osmotically active substances stimulating osmotic ADH
release
– Glucose
– Chronic alcohol abuse
– Mannitol
– Sick-cell syndrome (leakage of intracellular ions)
Causes of hyponatraemia with decreased extracellular volume
• Gut
– Vomiting
– Diarrhoea
– haemorrhage
• Kidney
– Osmotic diuresis (e.g. hyperglycaemia, severe uraemia)
– Excessive use of diuretics
– Adrenocortical insufficiency
– Tubulo-interstitial renal disease
– Unilateral renal artery stenosis
– Recovery phase of acute tubular necrosis
Electrolyte Balance Dr. Ali A. Allawi
26-11-2014
8
Causes of hyponatraemia with increased extracellular volume
• Heart failure
• Liver failure
• Oliguric renal failure
• Hypoalbuminaemia
Clinical manifestations of Hyponatremia
• Neurological symptoms
– Lethargy, headache, confusion, apprehension, depressed reflexes,
seizures and coma
• Muscle symptoms
– Cramps, weakness, fatigue
• Gastrointestinal symptoms
– Nausea, vomiting, abdominal cramps, and diarrhea
• Tx – limit water intake or discontinue meds
Done by
Ali Kareem