
Obesity
Clinical assessment and investigations
• Quantify the problem
• Exclude an underlying cause
• Identify complications
• Reach a management plan.

Obesity
Quantify the problem
• (BMI)
the body mass index
• (waist circumference)
abdominal obesity
Bioimpedance
• CT SCAN
• Densitometry (under water weighing)

Obesity
BMI (kg/m
2
)
Classification
Risk of co morbidity
18.5-24.9
Normal range
Negligible
25.0-29.9
Overweight
Mildly increased
≥ 30.0
Obese
30.0-34.9
Class I
Moderate
35.0-39.9
Class II
Severe
≥ 40.0
Class III
very severe

Obesity
3. Exclude an underlying cause
The Obesity-Focused History
A dietary history obtained by a specialist
dietitian
The patient's current diet and physical activity
Drug-induced weight gain should also to be
considered
specific symptoms of secondary causes of
obesity

Obesity
The Investigation
• Thyroid function
tests
(all patient)
• Serum cortisol
(Cushing's syndrome)
– Dexamethasone suppression test
– 24-hour urine free cortisol
• Genetic counseling
Monogenic and 'syndromic' causes (children
presenting with severe obesity)

Obesity
3.Identify complications
Assessment of
cardiovascular risk factors
Blood pressure
measuring blood glucose
serum lipid profile
• Serum
transaminases
(NASH)

Obesity
Management plan
• The Goal of Therapy
improve obesity-related comorbid conditions
reduce the risk of developing future comorbidities.
• The target
initial weight-loss goal of 10% over 6 months .
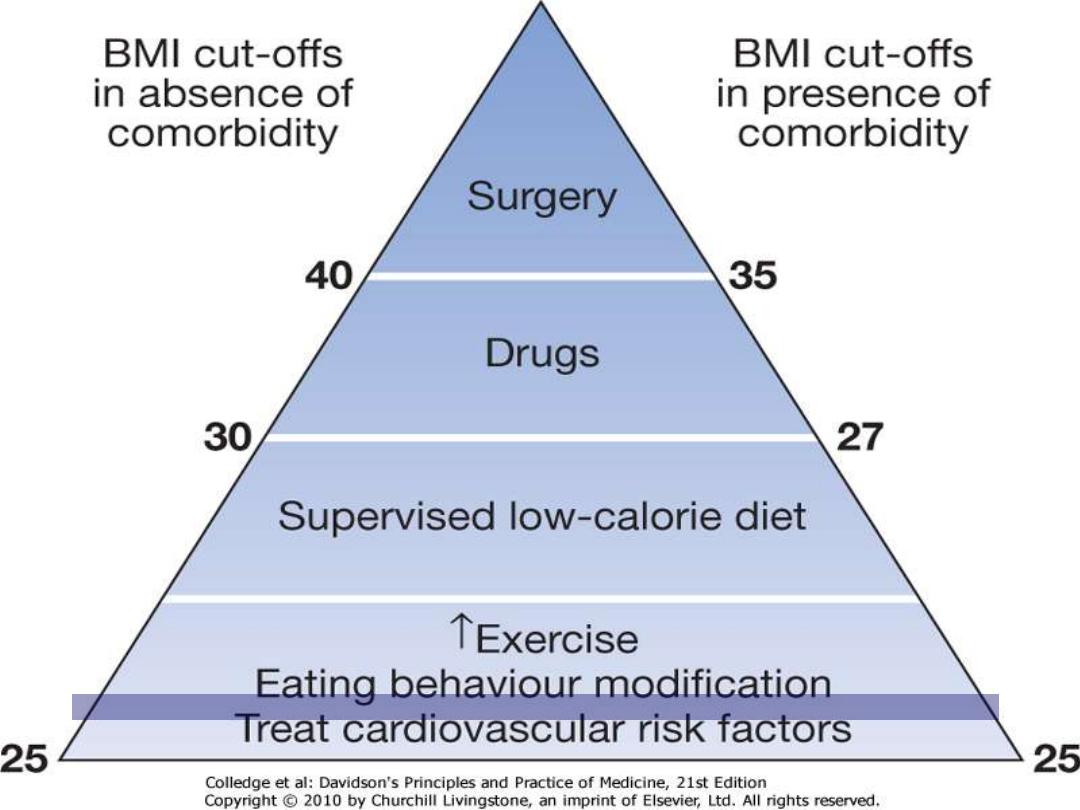
• The decision to treat depend
BMI
patient's risk status
Modalities
lifestyle management
pharmacotherapy
surgery
Downloaded from: StudentConsult (on 6 December 2011 05:10 PM)
© 2005 Elsevier

Obesity
Lifestyle management
Behavioral Therapy
new dietary and physical activity behaviors.
Strategies
:
• maximizing physical activity (e.g. walking
rather than driving to work)
• Changes in eating behavior including
food selection
portion size control
avoidance of snacking
regular meals to encourage satiety

Obesity
Physical activity
Exercise alone is only
moderately
effective for
weight loss
Moderate exercise( brisk walking) 60m./5
times/week/1 year produce minimal wt loss
Moderate intensive( treadmill walking,
bicycling)45m./5 times/week/1year produce
5kg loss
The most important role of exercise appears to
be in the
maintenance
of the weight loss.
Obesity
Weight loss diets
In obese patients, more active intervention is
usually required to lose weight before
conversion to 'weight maintenance' advice
low caloric diet
is the cornerstone of the
obesity treatment
They all involve a reduction of daily total
energy intake of (
500-1000 kcal
) from the
patient's normal consumption.
The goal is to lose
0.5 kg/week.
Obesity
Very low calorie diets
(VLCDs)
are
recommended for short-term rapid weight
loss, producing losses of 1.5-2.5 kg/week
Energy content should be a minimum of (
500
kcal
) in VLCD
There is no role for
starvation diets
, which risk
profound loss of muscle mass and the
development of arrhythmias

Obesity
Total Strategies:
choosing smaller portion sizes
selecting leaner cuts of meat and skimmed
dairy products
drinking water instead of caloric beverages.
reducing fried foods and other added fats and
oils
Eating
Low energy dense food
fruits and vegetables
Avoid high energy dense food
high-fat foods such as pretzels, cheese, egg
yolks, potato chips, and red meat.

Obesity
Pharmacotherapy:
Indications:
BMI
≥30 kg/m
2
BMI
≥27 kg/m
2
with concomitant comorbidities
Dietary and physical activity therapy
not
successful
Types:
1. Suppression of appetite via centrally active
medications
2. Second strategy is to reduce the absorption
of selective macronutrients such as fat.
3. Selective blocking of the endocannabinoid

Obesity
Centrally Acting Anorexia Medications
sibutramine (Meridia) : central serotonin and
norepinephrine reuptake inhibitor
Benefit:
loss of about 5
–9% of initial body weight at 12 month
maintain weight loss for up to 2 years.
Side effects:
headache, dry mouth, insomnia, and constipation.
dose-related increase in blood pressure and heart rate
Contraindications:
uncontrolled hypertension
congestive heart failure
symptomatic coronary heart disease
arrhythmias, or history of stroke

Obesity
Peripherally Acting Medications
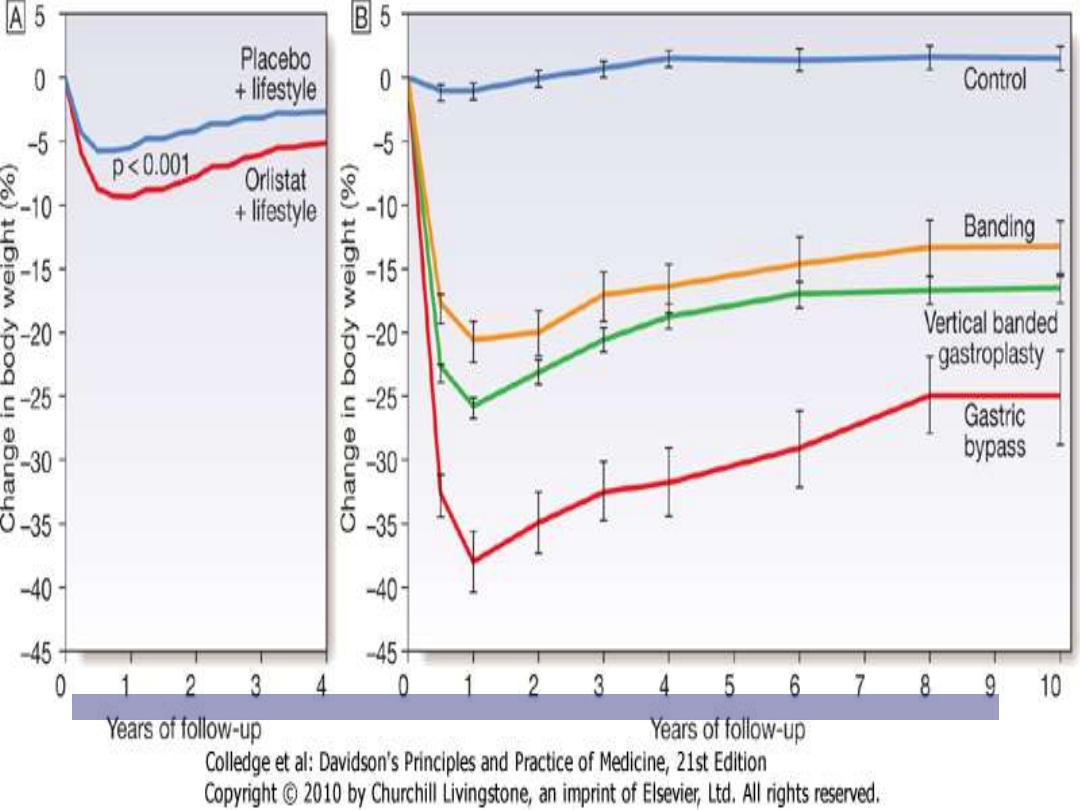
• Orlistat (Xenical) is a synthetic derivative of a naturally
occurring lipostatin( lipase inhibitor)
• slowly reversible inhibitor of pancreatic, gastric lipases
• orlistat blocks the digestion and absorption of about
30% of dietary fat.
• Benefit:
• orlistat produces a weight loss of about 9–10%,
GI tract adverse effects
• flatus
• fecal urgency, oily stool
• increased defecation
• Serum concentrations of the fat-soluble may be
reduced

Obesity
Cannabinoid receptor antagonist
• Rimonabant acts in the hypothalamus to
reduce appetite
• Side effects :
• exacerbate or induce depression
• associated with a small increased risk of
suicide

Obesity
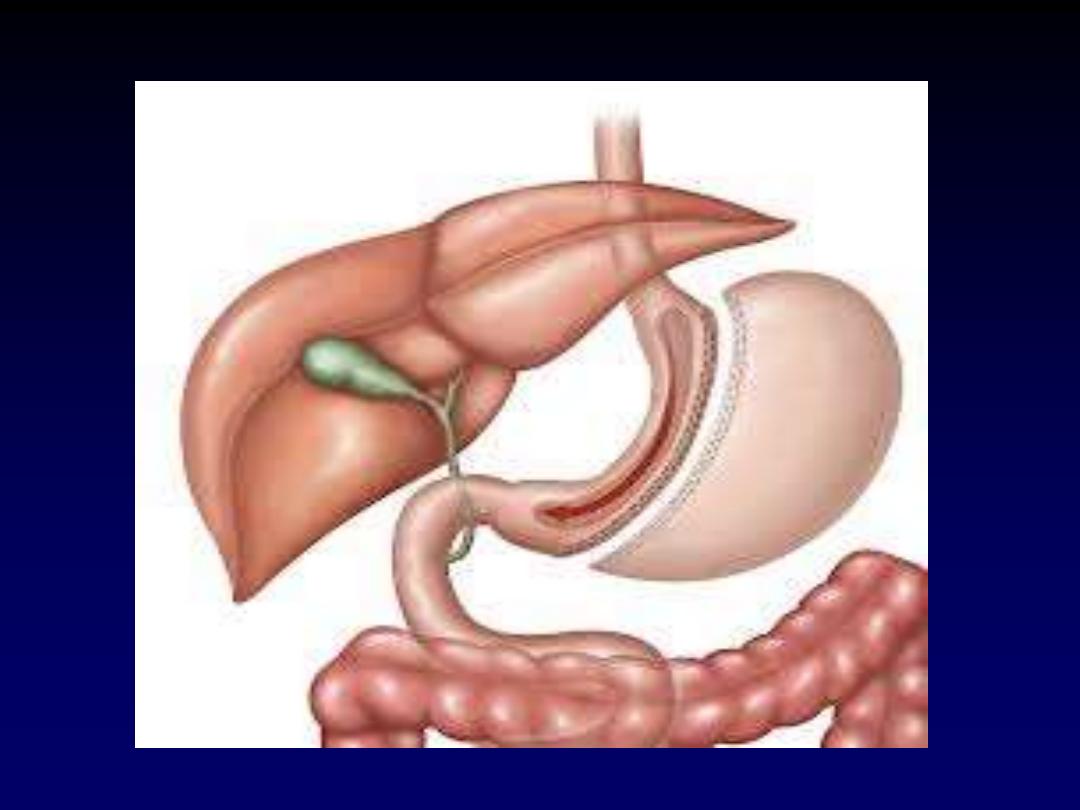
Surgery (Bariatric surgery )
most effective
weight-loss therapy for
severe
obesity.
produce
30
–35%
body weight loss that is
maintained in nearly
60%
of patients at 5
years.
weight loss
is greater after bypass than
gastric surgery
positive impact
on obesity-related morbidities
ass DM, HT and obstructive sleep apnea

Obesity
Indications:
BMI
> 40 kg/m
2
)
BMI
> 35 kg/m
2
) associated with a comorbidities.
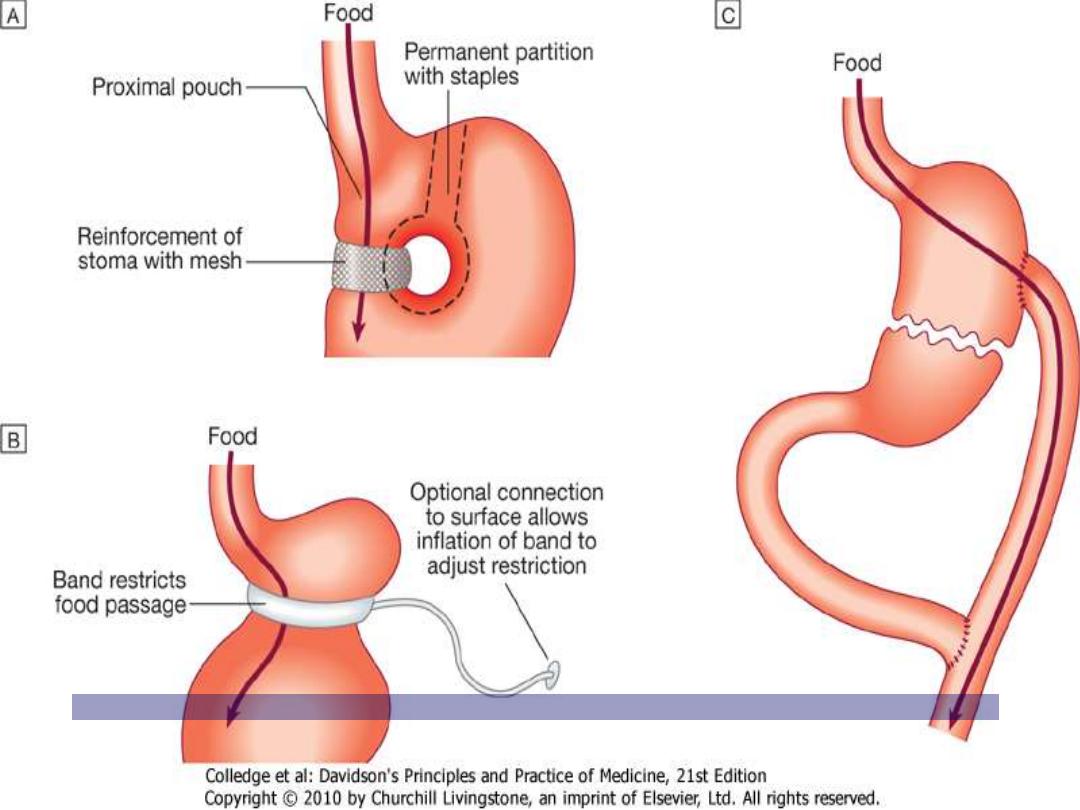
Weight-loss surgeries
:
• Restrictive
partial gastrectomy( sleeve gastroec).
Laparoscopic gastric banding
• Restrictive-malabsorptive
.
Roux-en-Y gastric bypass
Downloaded from: StudentConsult (on 6 December 2011 05:10 PM)
© 2005 Elsevier
Downloaded from: StudentConsult (on 6 December 2011 05:10 PM)
© 2005 Elsevier

Thanks