Dr. Abdulla Al-Farttoosi
Lec. 5
Cestodes
Mon 6/ 4 / 2015
2014 – 2015
ﻣﻜﺘﺐ ﺍﺷﻮﺭ ﻟﻼﺳﺘﻨﺴﺎﺥ
CESTODES Dr. Abdulla Al-Farttoosi
6-4-2015
1
CESTODES
Cestodes, or tapeworms, are segmented worms. The adults reside in the
gastrointestinal tract, but the larvae can be found in almost any organ. Two major
clinical groups.
Humans are the definitive hosts, with the adult tapeworms living in the
gastrointestinal tract (Taenia saginata, Diphyllobothrium, Hymenolepis, and
Dipylidium caninum).
Humans are intermediate hosts, with larval-stage parasites present in the tissues;
diseases in this category include echinococcosis, sparganosis, and coenurosis.
Taenia solium, the human may be either the definitive or the intermediate host.
The ribbon-shaped tapeworm attaches to the intestinal mucosa by means of
sucking cups or hooks located on the scolex.
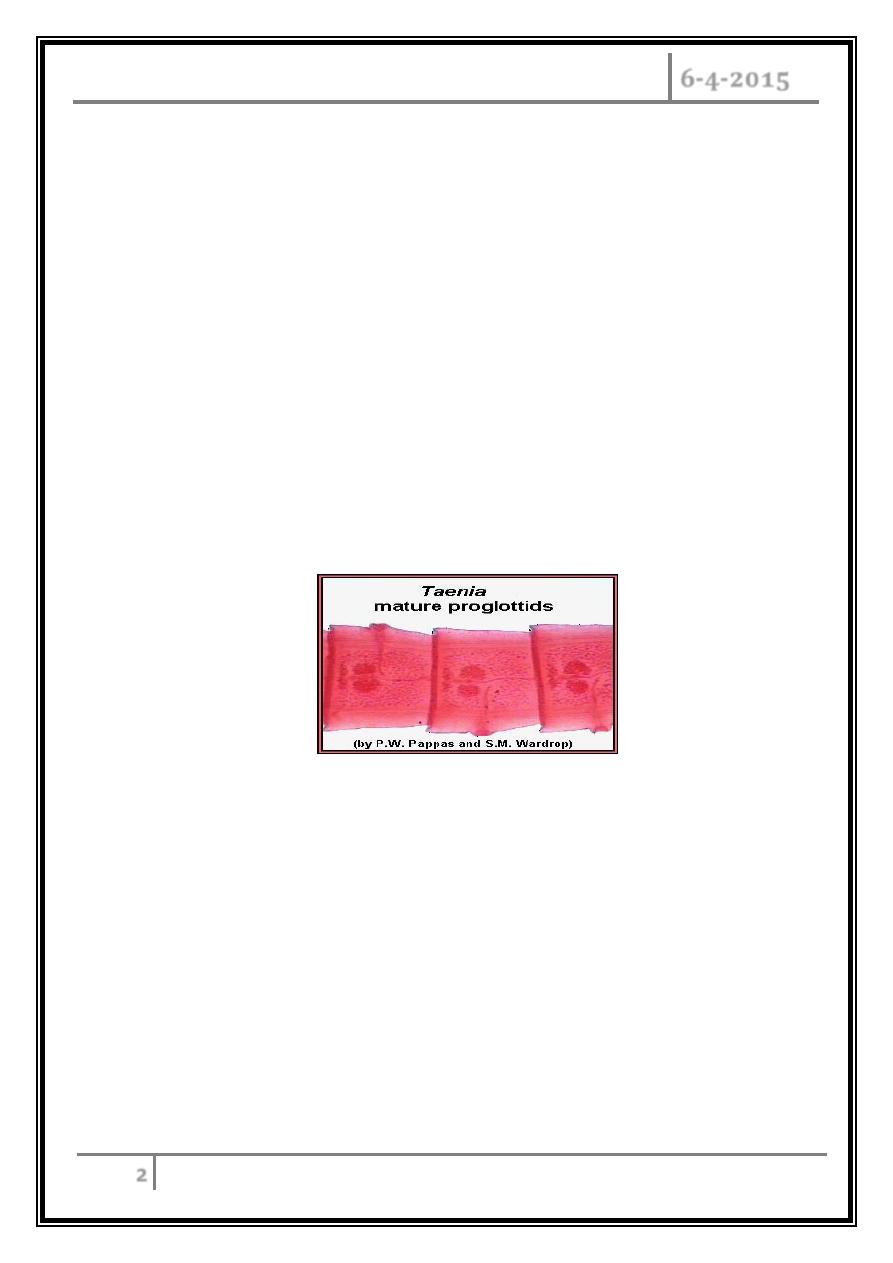
Proglottids (segments) form behind the scolex and constitute the bulk of the
tapeworm.
The length varies among species. In some, the tapeworm may consist of more
than 1000 proglottids and may be several meters long. The mature proglottids are
hermaphroditic and produce eggs, which are subsequently released.
Since eggs of the different Taenia species are morphologically identical,
differences in the morphology of the scolex or proglottids provide the basis for
diagnostic identification to the species level.
Most human tapeworms require at least one intermediate host for complete
larval development.
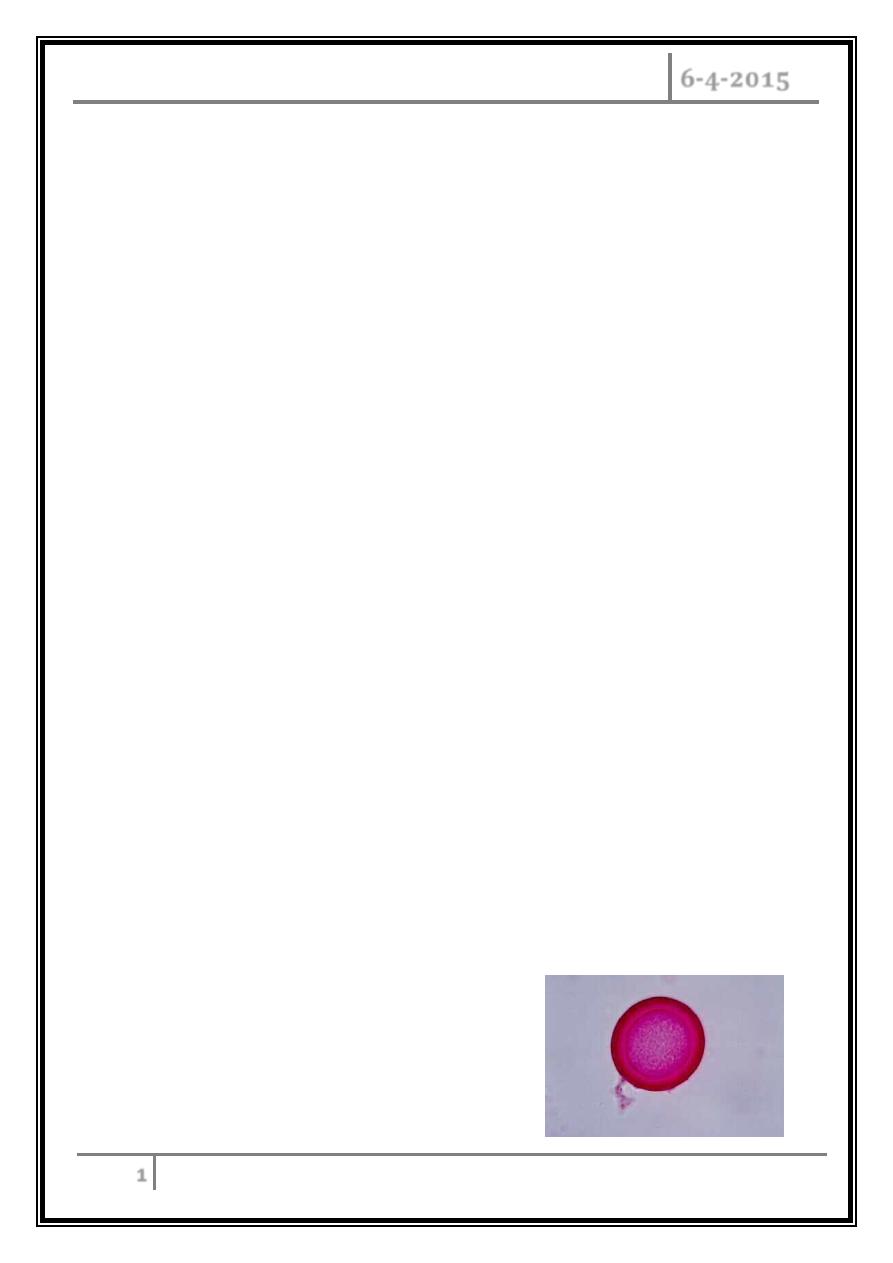
Picture of a T. saginata egg.
Identical to the T.solium egg
to the naked eye.
CESTODES Dr. Abdulla Al-Farttoosi
6-4-2015
2
Taenia saginata
(Beef Tapeworm) - Taeniasis
Etiology and Pathogenesis:
Human is the definitive host for Taenia saginata, the beef tapeworm, which
inhabits the upper jejunum. Eggs are excreted in feces and ingested by cattle or
other herbivores; larvae encyst (cysticerci) in the striated muscles of these animals.
When humans ingest raw or undercooked beef, the cysticerci mature into adult
worms.
Incubation Period
It takes about 5 to 12 weeks for the worm to mature into adulthood in the
human intestine. Usually only a single worm is present at time. However, multiple
worms have been known to inhabit the human body.
Clinical Features
Pts may experience perianal discomfort, mild abdominal pain, nausea, change
in appetite, weakness, and weight loss.
Diagnosis
The diagnosis is made by detection of eggs or proglottids in the stool. Eggs may
be found in the perianal area. Eosinophilia may develop, and IgE levels may be
elevated.
Treatment
Praziquantel is given in a single dose of10 mg/kg.
CESTODES Dr. Abdulla Al-Farttoosi
6-4-2015
3
Taenia solium
(Pork Tapeworm) - Taeniasis and
Cysticercosis
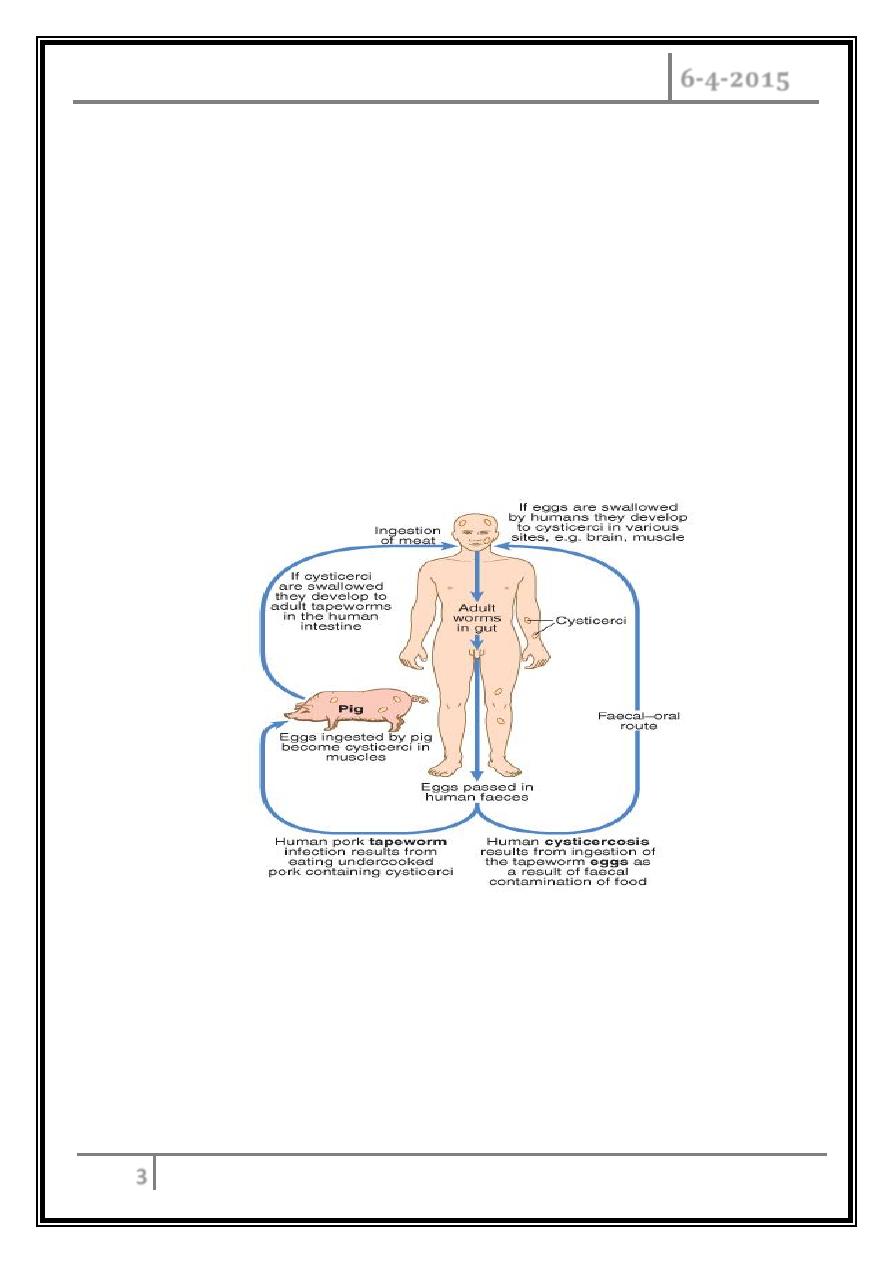
Etiology and Pathogenesis
Humans are the definitive host and pigs the intermediate host for T. solium,
the pork tapeworm. The disease, which is due to ingestion of pork infected with
cysticerci, is similar to taeniasis saginata.
If humans ingest T. solium eggs (e.g., as a result of close contact with a
tapeworm carrier or via autoinfection), they develop cysticercosis. Larvae penetrate
the intestinal wall and are carried to many tissues, where cystercerci develop.
Incubation Period
It takes about 5 to 12 weeks for the worm to mature into adulthood in the
human intestine. Usually only a single worm is present at time. However, multiple
worms have been known to inhabit the human body. T. solium may survive up to 25
years or more.
CESTODES Dr. Abdulla Al-Farttoosi
6-4-2015
4
Clinical Features
Intestinal infections: epigastric discomfort, nausea, a sensation of hunger,
weight loss, and diarrhea can occur, but most infections are asymptomatic.
Cysticercosis: cysticerci can be found anywhere in the body but most often are
detected in the brain, skeletal muscle, SC tissue, or eye. Neurologic
manifestations are most common and include seizures due to inflammation
surrounding cysticerci in the brain, hydrocephalus (from obstruction of CSF flow
by cysticerci and accompanying inflammation or by arachnoiditis), headache,
nausea, vomiting, changes in vision, dizziness, ataxia, and confusion.
Diagnosis
Intestinal infection is diagnosed by detection of eggs or proglottids in stool.
Calcified cysts in muscles can be recognized radiologically. In the brain, however,
less calcification takes place and larvae are only occasionally visible by plain X-
ray; usually CT or MRI will show them.
Epileptic fits starting in adult life suggest the possibility of cysticercosis if the
patient has lived in or travelled to an endemic area. The subcutaneous tissue
should be palpated and any nodule excised for histology. Antibody detection is
available for sero-diagnosis.
Treatment
Intestinal infections respond to a single dose of praziquantel (10 mg/kg).
Neurocysticercosis can be treated with albendazole (15 mg/kg per day for 8–28
days) or praziquantel (50–60 mg/kg daily in 3 divided doses for 15 days or 100
mg/kg in 3 doses given over 1 day).
Patients should be carefully monitored, given the potential for an inflammatory
response to treatment. High-dose glucocorticoids can be administered during
treatment, particularly if symptoms become worse during therapy; since
glucocorticoids induce praziquantel metabolism, cimetidine should be given with
praziquantel to inhibit this effect.
Supportive measures include antiepileptic administration and treatment of
hydrocephalus as indicated.
CESTODES Dr. Abdulla Al-Farttoosi
6-4-2015
5
Echinococcosis
Etiology and Pathogenesis
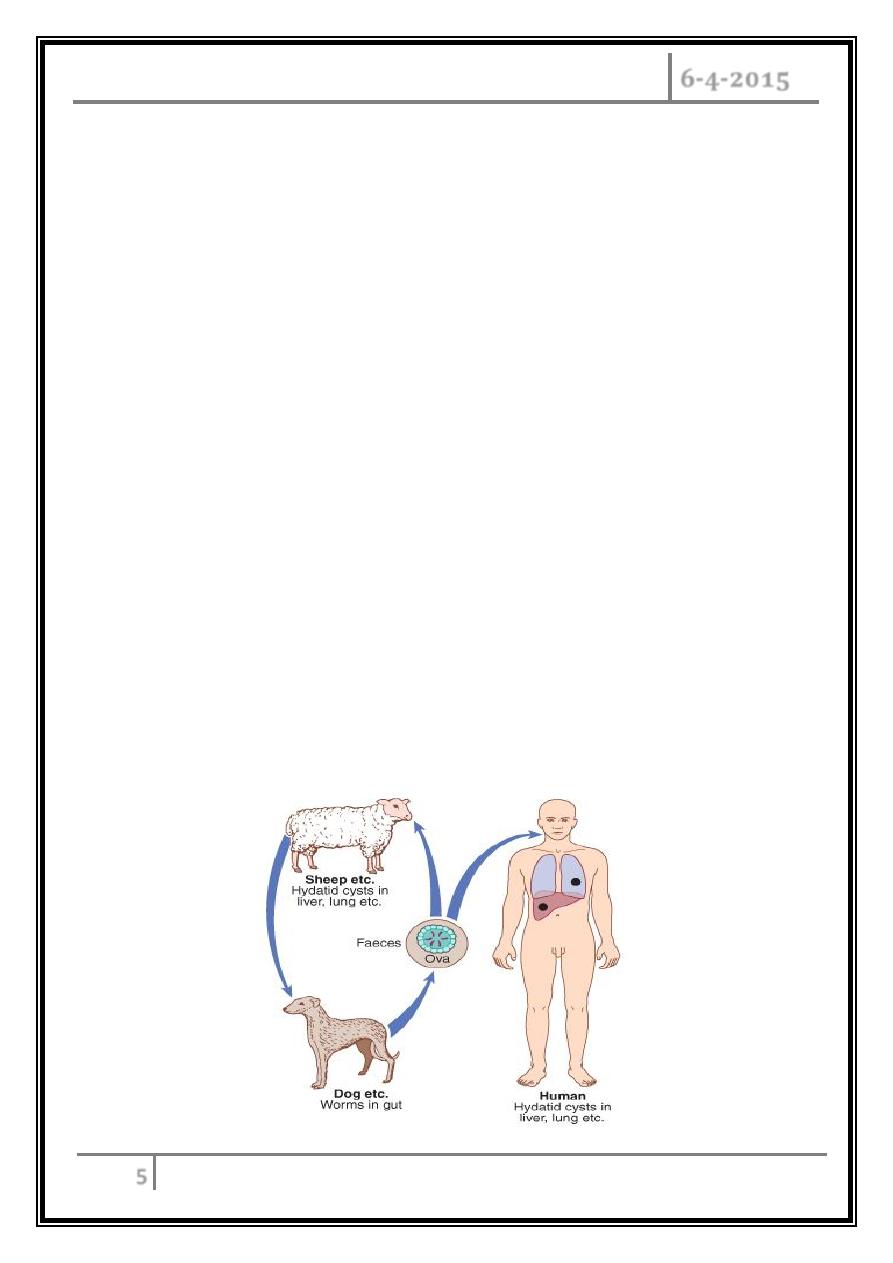
o Echinococcosis is an infection of humans that is caused by Echinococcus larvae.
The adult worm of E. granulosus lives in the jejunum of dogs and releases eggs
that humans may ingest.
o Human echinococcosis (hydatidosis, or hydatid disease) is caused by the larval
stages of cestodes (tapeworms) of the genus Echinococcus. Echinococcus
granulosus causes cystic echinococcosis (CE), the form most frequently
encountered; E. multilocularis causes alveolar echinococcosis (AE).
o Disease is prevalent in areas where livestock is raised in association with dogs.
After ingestion, embryos escape from the eggs, penetrate the intestinal mucosa,
enter the portal circulation, and are carried to many organs but particularly the
liver and lungs.
o Larvae develop into fluid-filled unilocular hydatid cysts within which daughter
cysts develop, as do germinating cystic structures. Cysts expand over years. E.
multilocularis, found in arctic or subarctic regions, is similar, but rodents are the
intermediate hosts. The parasite is multilocular, and vesicles progressively
invade host tissue by peripheral extension of processes from the germinal layer.
CESTODES Dr. Abdulla Al-Farttoosi
6-4-2015
6
Clinical Features
Expanding cysts exert the effects of space-occupying lesions, causing
symptoms in the affected organ. Patients with hepatic disease most
commonly present with abdominal pain or a palpable mass in the RIGHT
UPPER QUADRENT. Compression of a bile duct may cause biliary obstruction
or may mimic cholelithiasis.
Rupture or leakage from a hydatid cyst may cause fever, pruritus, urticaria,
eosinophilia, or anaphylaxis. Pulmonary cysts may rupture into the bronchial
tree or the peritoneal cavity and cause cough, chest pain, or hemoptysis.
Rupture of cysts may result in multifocal dissemination. E. multilocularis
disease may present as a hepatic tumor, with destruction of the liver and
extension into vital structures.
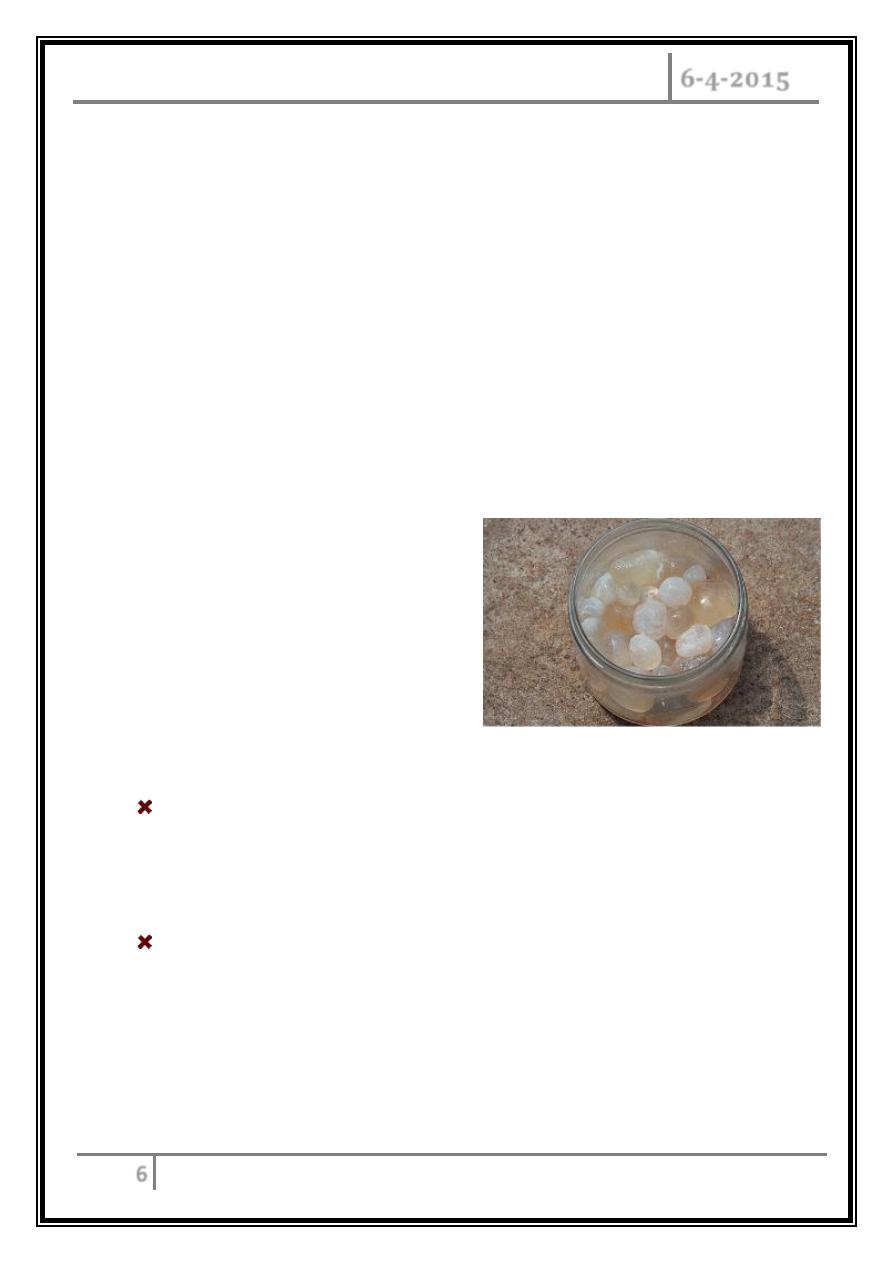
Daughter cysts removed at
surgery
Diagnosis
Radiographic imaging is important in evaluating echinococcal cysts. Daughter
cysts within a larger cyst are pathognomonic. Eggshell or mural calcification
on CT is indicative of E. granulosus infections. Serology may be useful but can
be negative in up to half of pts with lung cysts.
Serology is usually positive in patients with hepatic disease. Aspiration of cysts
usually is not attempted because leakage of cyst fluid can cause dissemination
or anaphylactic reactions.
CESTODES Dr. Abdulla Al-Farttoosi
6-4-2015
7
Treatment
Ultrasound staging is recommended for E. granulosus infection. Therapy is
based on considerations of the size, location, and manifestations of cysts and
the overall health of the pt. For some uncomplicated lesions, percutaneous
aspiration, infusion of scolicidal agents, and re-aspiration are recommended.
Albendazole (15 mg/kg daily in 2 divided doses for 4 days before the
procedure and for at least 4 weeks afterward) is given for prophylaxis of
secondary peritoneal echinococcosis due to inadvertent spillage of fluid
during this treatment. Surgery is the treatment of choice for complicated E.
granulosus cysts.
Albendazole should also be given prophylactically, as just described.
Praziquantel (50 mg/kg daily for 2 weeks) may hasten the death of
protoscolices.
Medical therapy alone with albendazole for 12 weeks to 6 months results in
cure in 30% of cases and in clinical improvement in another 50%. E.
multilocularis infection is treated surgically, and albendazole is given for at
least 2 years after presumptively curative surgery. If surgery is not curative,
albendazole should be continued indefinitely.
Diphyllobothriasis
►
Diphyllobothrium latum, the longest tapeworm (up to 10 meters), attaches to
the ileal and occasionally the jejunal mucosa. Humans are infected by eating raw
fish. Symptoms are rare and usually mild, but infection can cause vitamin B12
deficiency because the tapeworm absorbs large amounts of vitamin B12 and
interferes with ileal B12 absorption.
CESTODES Dr. Abdulla Al-Farttoosi
6-4-2015
8
►
Up to 2% of infected pts, especially the elderly, have megaloblastic anemia
resembling pernicious anemia and can suffer neurologic sequelae due to B12
deficiency. The diagnosis is made by detection of eggs in the stool. Praziquantel
(5–10 mg/kg once) is highly effective.
… the end …