Dr. Alaa Al-Deen
Lec. 2
Leprosy
Mon 23 / 3 / 2015
2014 – 2015
ﻣﻜﺘﺐ ﺍﺷﻮﺭ ﻟﻼﺳﺘﻨﺴﺎﺥ
LEPROSY Dr. Alaa Al-Deen
23-3-2015
1
Leprosy
What causes it?
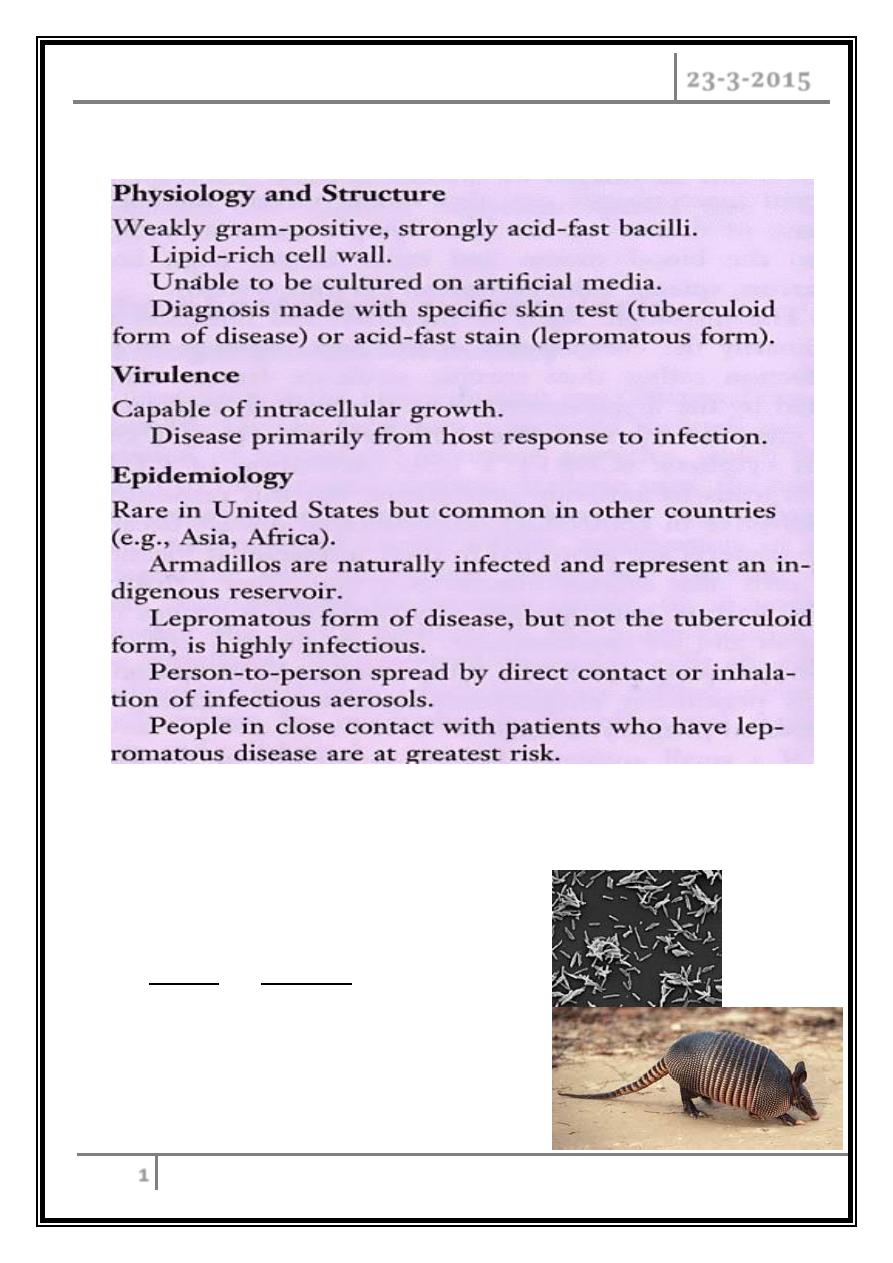
Rod-shaped.
Humans and Armadillos are only
known natural reservoir for
Mycobacterium leprare.
LEPROSY Dr. Alaa Al-Deen
23-3-2015
2
• Mycobacterium leprare multiplies very slowly.
• Symptoms can take as long as 20 years to appear.
• Organisms can’t be distinguished microscopically from other mycobacteria.
What are the types of leprosy?
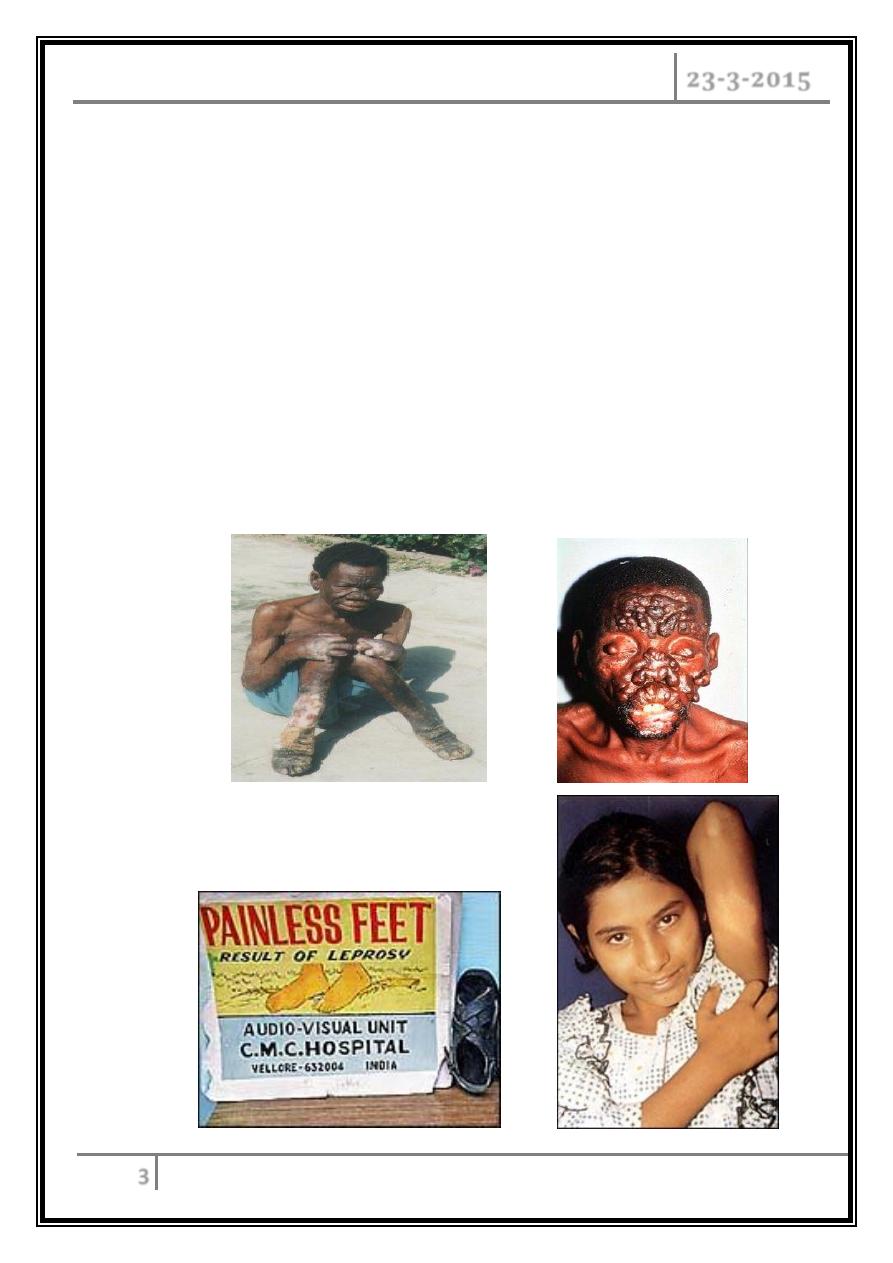
- Lepromatous: damages respiration, eyes, and skin.
- Tuberculoid: affects nerves and skin.
- Borderline: has effects of both types.
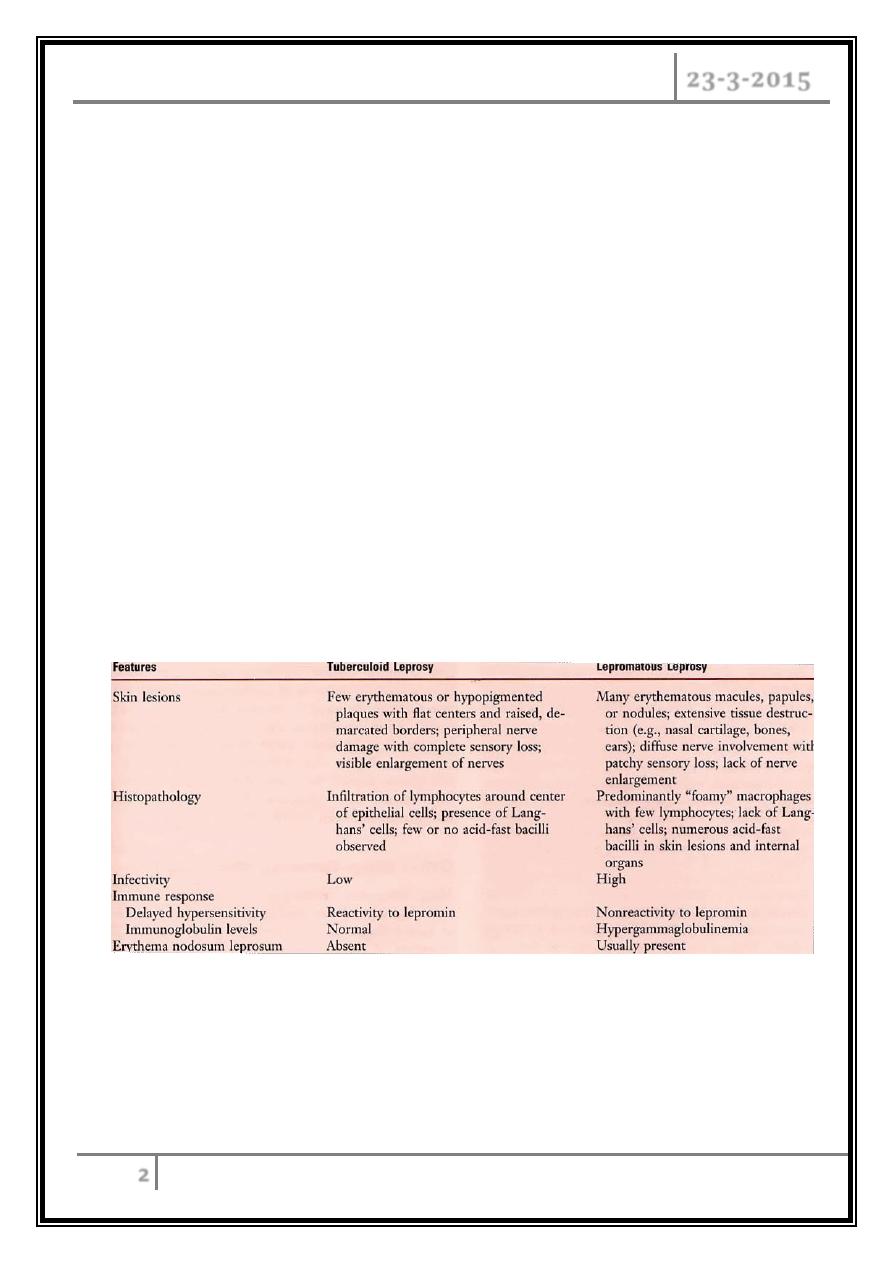
Tuberculoid vs. Lepromatous Leprosy
Clinical Manifestations and Immunogenicity
LEPROSY Dr. Alaa Al-Deen
23-3-2015
3
Borderline tubercloid
Skin lesions are similar to those with tubercloid but are more numerous.
Damage to peripheral nerve more widespread.
Patients are prone to type I reaction.
Borderline lepromatous
Widespresd small macules.
Peripheral nerve involvement is widespread.
Experience type I & II reaction.
LEPROSY Dr. Alaa Al-Deen
23-3-2015
4
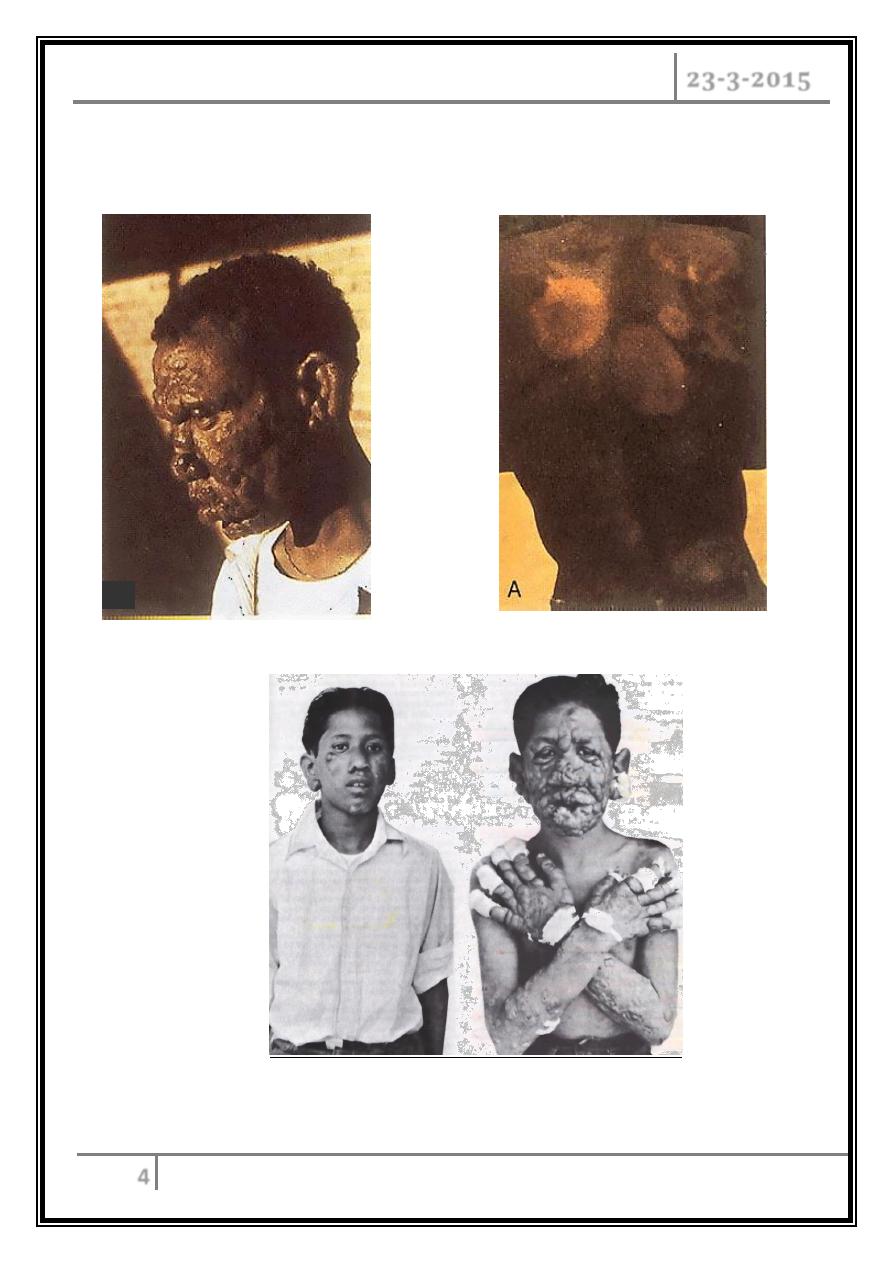
Lepromatous
vs.
Tuberculoid Leprosy
Lepromatous Leprosy (Early/Late Stages)
LEPROSY Dr. Alaa Al-Deen
23-3-2015
5
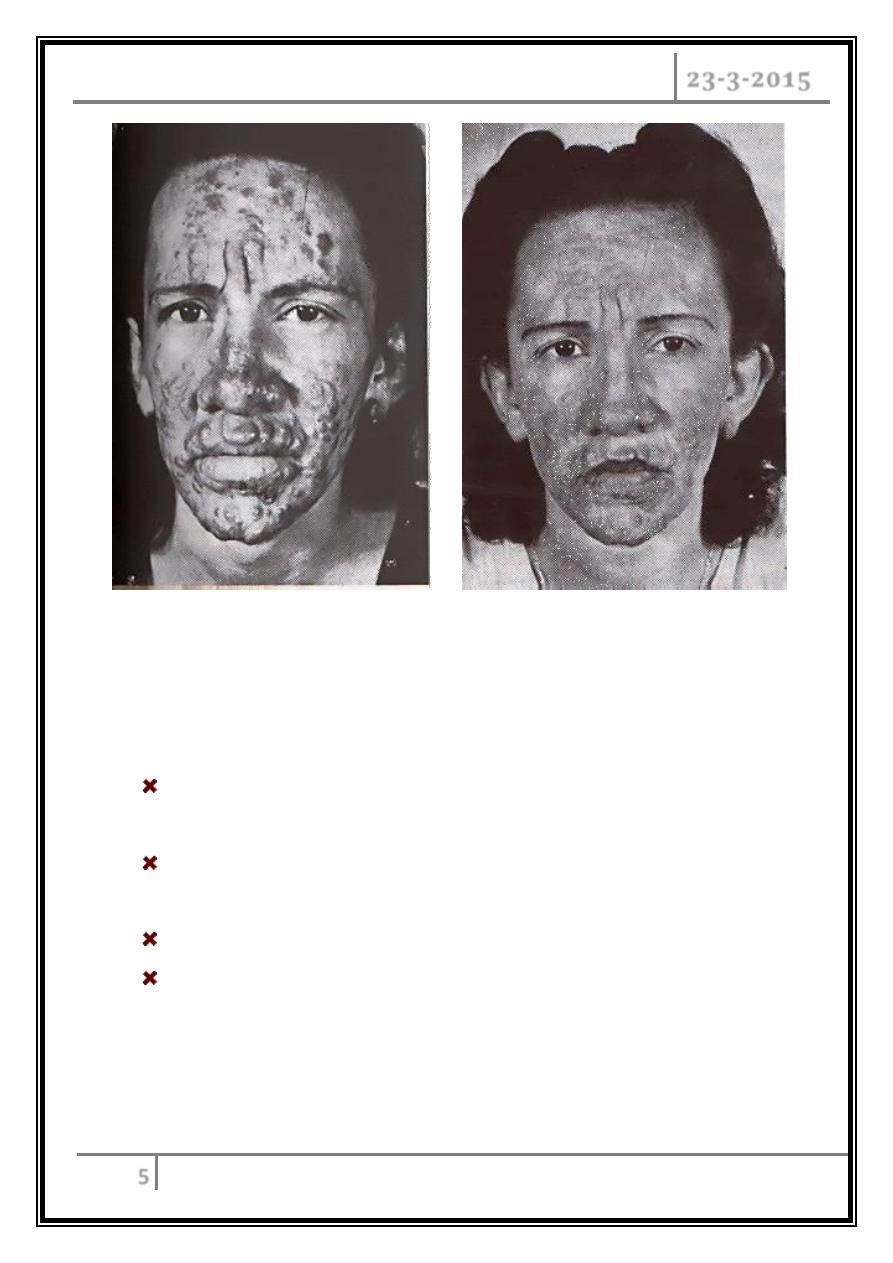
Lepromatous Leprosy Pre- and Post-Treatment
TYPE 1 LEPRA REACTIONS
These reactions occur in almost half of patients with borderline forms of
leprosy (BT, BL, and BB).
Manifestations include classic signs of inflammation within previously involved
macules, papules, and plaques and, on occasion.
Peripheral nerves become tender and painful with sudden loss of function.
Fever—generally low-grade.
LEPROSY Dr. Alaa Al-Deen
23-3-2015
6
TYPE 2 LEPRA REACTIONS
(ERYTHEMA NODOSUM LEPROTICUM, ENL)
ENL occurs exclusively in patients near the lepromatous end of the leprosy
spectrum (BL, and LL).
Immune-complex deposition.
Although ENL may precede leprosy diagnosis and initiation of therapy and in
90% of cases it follows the institution of chemotherapy.
Crops of painful erythematous papules or nodule that resolve spontaneously in
a few days to a week.
It may recur.
Malaise and fever that can be profound.
Acute neuritis.
Iritis and episcleritis are common.
Acute neuritis, lymphadenitis, orchitis, bone pain, dactylitis, arthritis.
DIAGNOSIS:
Biopsy the advancing edge of a skin lesion in TT.
In LL, biopsy even of normal-appearing skin often yields positive results.
Presence of acid fast bacilli in slit skin smear or typical histopathalogy.
LEPROSY Dr. Alaa Al-Deen
23-3-2015
7
Complications:
Extremities: Neuropathy results in insensitivity and affects fine touch, pain,
and heat receptors. Ulcerations, trauma, secondary infections, and (at times) a
profound osteolytic process can take place.
Nose: chronic nasal congestion and epistaxis, destruction of cartilage with
saddle-nose deformity or anosmia.
Eye: trauma, secondary infection, corneal ulcerations, opacities, uveitis,
cataracts, glaucoma, sometimes blindness.
Testes: orchitis, aspermia, impotence, infertility.
TREATMENT:
o Rifampin (daily or monthly) is the only bactericidal M. leprae agent.
o Clofazimine (3 times per week, or monthly). Clofazimine is weakly active
against M. leprae.
Regimens
Paucibacillary disease in adults (<6 skin lesions):
Monthly supervised: rifampin (600 mg monthly) for 6 months.
Daily self adminstered: Dapson (100 mg) daily for 6 months.
LEPROSY Dr. Alaa Al-Deen
23-3-2015
8
Multibacillary disease in adults (>6 skin lesions):
Monthly supervised: rifampin (600 mg monthly) plus clofazimine (300
mg monthly) supervised for 1 year.
Daily adminstration:Clofazimine 50 mg+ dapsone (100 mg/d) for 1 year.
Reactional states:
Mild reactions: glucocorticoids (40–60 mg/d for at least 3 months).
If ENL is present and persists despite two courses of steroids,thalidomide
(100–300 mg nightly) should be given.
… The end …