1
Parasitology
Objectives; to study the causative parasite of hydatid
disease including their morphology, life cycle, types of
hydatid cysts ,complications and diagnosis .
Echinococcus Spp.
Genus Echinococcus include three different species in which man acts as
intermediate host and infecting by the larval stage of these species. Adult worm
inhabit the small intestine of dogs and other canidae family.
These species causes a disease known as Echinococcosis or hydatidosis or
hydatid disease.
Species of Echinococcus
Definitive host
Intermediate host
E. granulosus
Dogs and other canidae
Sheep, goats, swine and
other herbivores
E. multilocularis
Foxes, dogs and wolves Small rodents
E. vogeli
Bush dogs and dogs
Small rodents
The most common species is E. granulosus which is present virtually
worldwide mainly in rural, grazing areas where dogs are able to ingest organs
from infected animals.
2
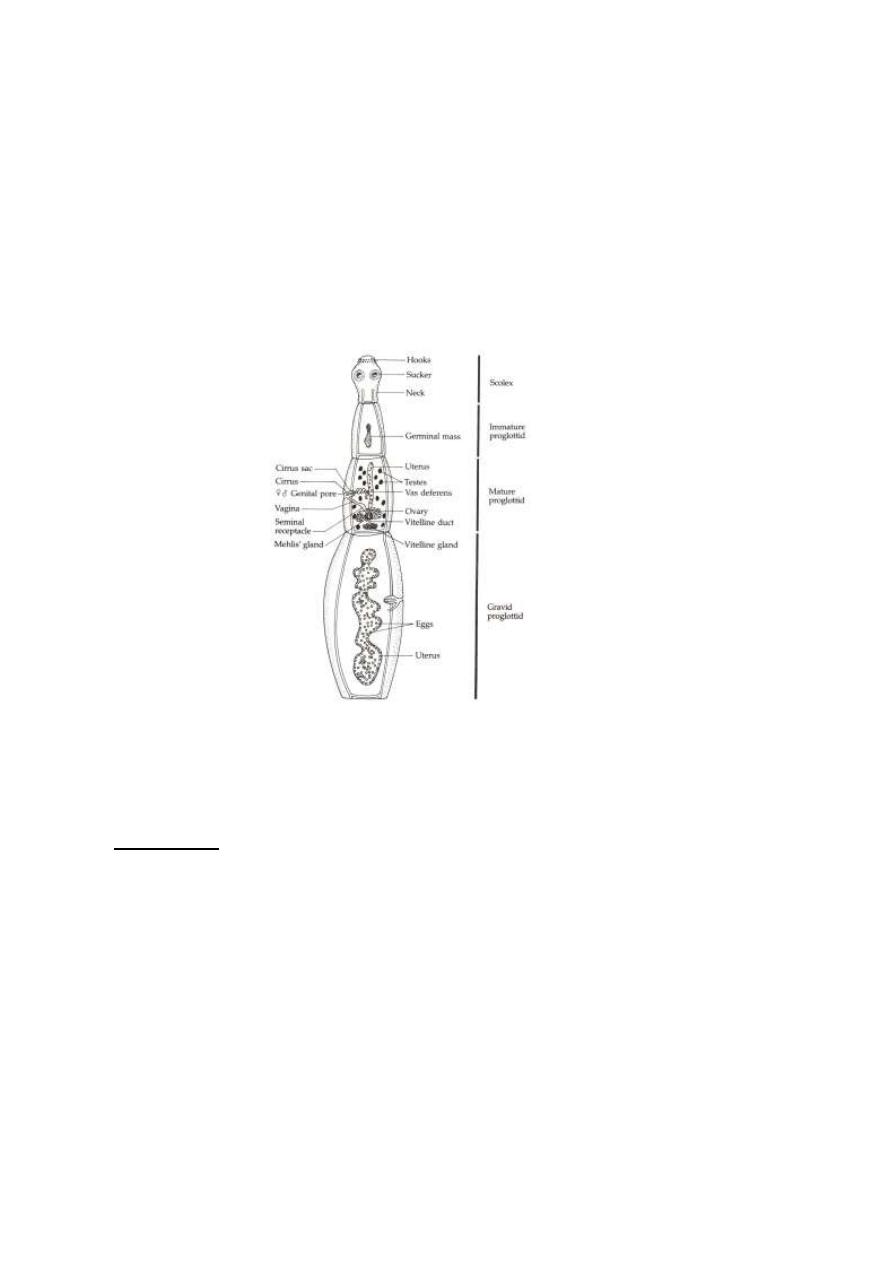
Echinococcus granulosus
Adult Worm: The length of E. granulosus from 3-6mm and have scolex with 4
suckers and rostellum with two rows of hooks, neck and 3 proglottids.
Eggs: are Taenia spp. eggs.
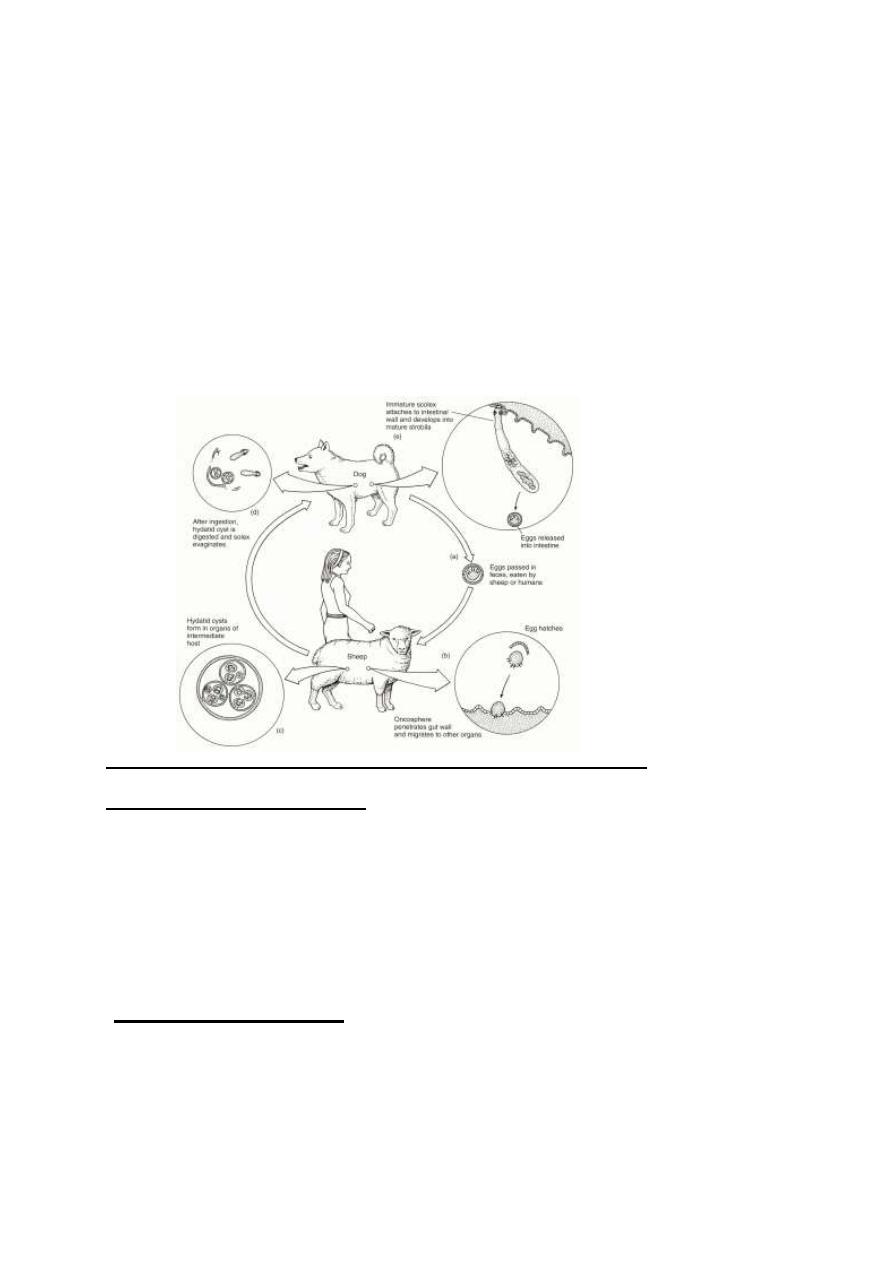
-Life Cycle:
Echinococcus spp. Require two hosts for completion of the life cycle. The
definitive hosts are carnivores harboring mature tapeworm, in the small
intestine. Larvae develop in the liver and other viscera of intermediate hosts.
Human beings become incidental intermediate hosts and do not complete the life
cycle of the parasite. Eggs are shed with the feces of infected definitive host,
when ingested by the suitable intermediate host, the oncospheres hatch in the
small intestine, become activated, penetrate the epithelial layer and migrate via
blood or lymphatic's vessels to the liver. In the liver most of oncospheres may
3
destroy by the action of phagocytic cells and only oncospheres which can escape
phagocytosis, can develop to hydatid cyst. The cyst then slowly enlarges,
creating daughter cyst and protoscolices within the mother cyst.
The definitive host then becomes infected after ingesting the cyst-
containing organs of the infected intermediate host. After ingestion, the
protoscolices attach to the intestine. They then develop into adult worms and
start all over again
Methods of Transmission:
Hydatidosis transmitted to intermediate host via ingestion of eggs with
contaminated uncooked vegetables and fruits, drinking water, by handling soil
and dirt or animal hair that containing eggs.
-Types of Hydatid Cyst:
1- Unilocular hydatid cyst.
2- Multilocular or alveolar hydatid cyst.
3- Osseous hydatid cyst.
4
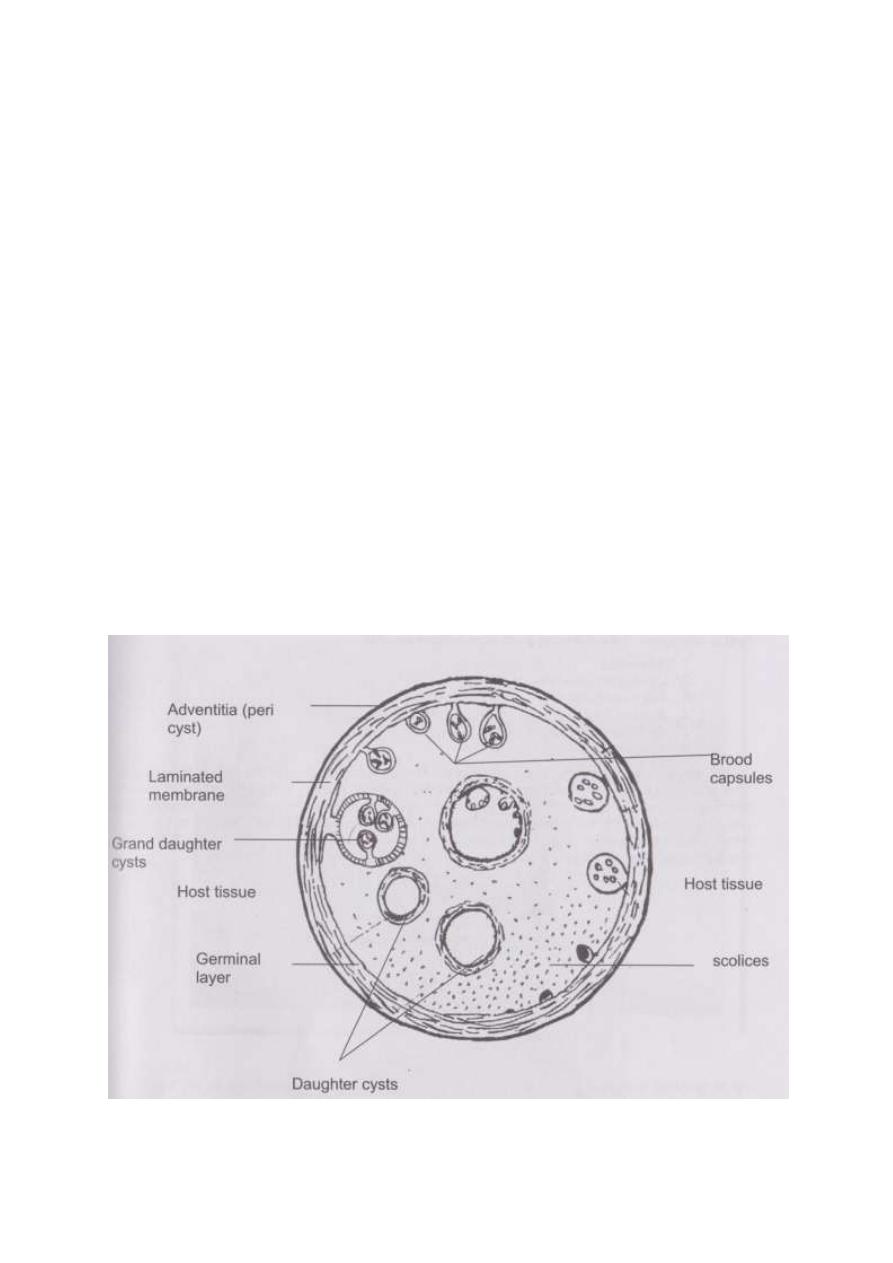
1) Unilocular Hydatid Cyst:
It is the larval stage of E. granulosus composed of single cavity; it is the
most common type of hydatid cyst and composed of the following layers:
1- External, milky laminated layer, about 1mm thickness and it is non-
nucleated. It is act as a support layer to inner germinal layer.
2- Inner germinal layer: is a thin, delicate layer, one cell thick and nucleated.
From inner germinal layer the following structures arise:
A- Brood Capsule: Develop from germinal layer and hold by short
pedicle to the germinal layer. In the brood capsule multiple
protoscolices develops. Hydatid cyst with protoscolices and brood
capsule is known as fertile hydatid cyst. Sometimes hydatid cyst will
not contain protoscolices, so it is known as sterile or acephalocyst.
Fertile hydatid cyst is more dangerous because each protoscolex will
develop to adult worm when ingested by definitive host and if fertile
hydatid cyst rupture it will lead to dissemination of the disease.
B- Hydatid Fluid: The cavity of unilocular hydatid cyst is filled with
hydatid fluid, which is highly antigenic, bacteriologically sterile and
colorless.
C- Hydatid Sand: If the brood capsule detached from germinal layer, the
brood capsule and protoscolices become free in hydatid fluid and they
are called hydatid sand. It contains evaginated and invaginated
protoscolices, the evaginated protoscolices are more dangerous.
D- Endogenous Daughter Cyst: sometime the cyst rupture and the
parasite try to survive itself by formation of endogenous daughter cyst
within the mother cyst. Daughter cyst is morphologically resemble
mother cyst but it is smaller in size and free in hydatid fluid.
5
Endogenous daughter cyst may be derived from:
1- Regressive changes of brood capsule.
2- Fragment of germinal layer.
3- Vesiculation of protoscolices.
E- Exogenous daughter cyst: usually arise due to herniation of germinal and
laminated layers as a result of increased intra-cystic pressure or trauma or
unfavorable conditions, it is usually occurs in bone hydatid cyst.
3- Dense layer of fibrous tissue over the laminated layer. This layer formed
as a result of defense mechanism of the host against foreign body.
6
2) Osseous Hydatid Cyst:
When the embryo reaches bony tissues it will develop to osseous hydatid
cyst. The external laminated layer is not produced or poorly developed.
The larva grows as a protoplasmic stream that erodes the cancellous
tissues and lead to multiple bone fractures. It is occur in the ends of long
bones and pelvic arch sterile never produces brood capsule and
protoscolices with little or no fluid and no fibrous capsule.
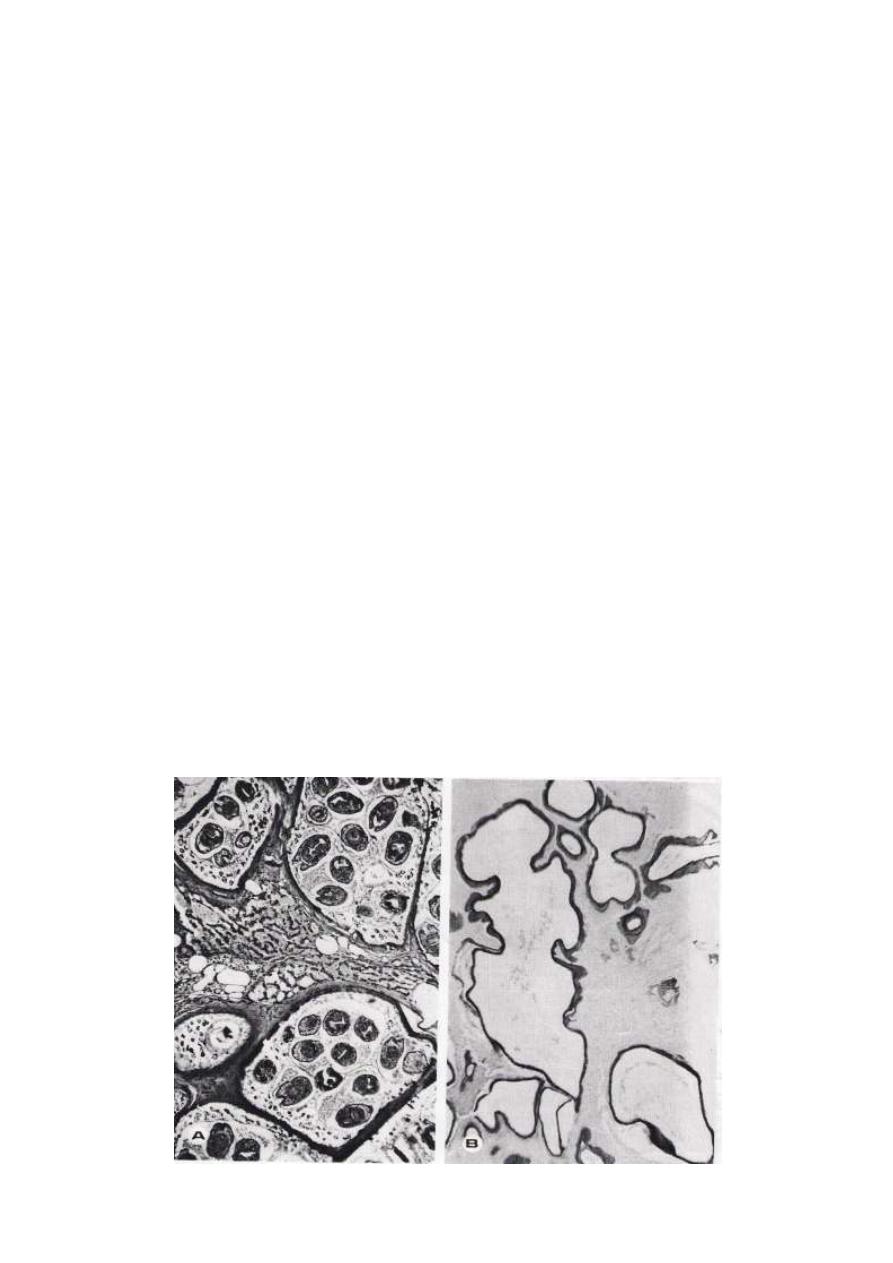
3) Multilocular or Alveolar Hydatid Cyst:
It is the larval stage of E. multilocularis, it is composed of numerous small
spaces or cavities, separated from each other by connective tissue. Each
space filled with jelly-like matrix, mostly it is sterile but occasionally it
may contain protoscolices. The germinal and laminated layers are poorly
developed, it has no fibrous capsule.
It is occurs usually in the liver and rarely in lung. Because of its fast
growth, it is usually fatal. Metastasis of alveolar cyst occurs via blood
stream by plasmodia cells arise from germinal layer.
7
Fertile multilocular hydatid cyst Sterile multiloculor hydatid cyst
Rupture of Hydatid Cyst:
Rupture of hydatid cyst may occur naturally, or in process of obtaining a
biopsy for microscopic examination, due to coughing, muscle strain or surgical
procedures. Such patients may suffer from anaphylactic shock, eosinophilia and
allergic reactions or even death. The escape cyst fluid with protoscolices has the
capacity of spreading to other sites and forming a new cyst (secondary
hydatidosis). Rupture of the cyst are most important than the mass effect of the
cyst, except in the brain where the mass effect has severe consequences.
-Pathogenesis and pathology
:
The pathological effects of hydatid cyst and their clinical features are
mainly due to two factors ;
1-localization with mechanical effects brought about by the cyst acting as
any other space –occupying lesion,with subsequent complications occuring
locally and possibly, leading to systemic manifestations .
2-The generalized allergic reactions due to absorption of the antigenic
material of the parasite .
Unilocular hydatid cyst following primary infection may inhabit any
anatomic site. The two most common organs involved are liver 65% and lungs
25%. Other less common sites affected by cysts include muscles, spleen, bones,
kidneys and CNS.
The majority of patients has single-organ involvement and harbors a solitary
cyst. Secondary infection follows cyst rupture and scolices can grow in the
peritoneum, pleura, bronchial tree and bile ducts or be carried via blood stream
be distant organs. In older cyst, the contents degenerate and then calcification
8
occur in the fibrous capsule, mother cyst and daughter cyst. Calcification of
endocyst indicates that the cyst is nonviable.
-Diagnosis
: It depends on clinical manifestation, imaging techniques and
laboratory diagnosis.
Clinical manifestations: Is difficult because the sign of the disease vary widely
and is based upon the presence of slowly growing tumor.
Clinical manifestations depend on the size and site of hydatid cyst. At the
beginning the disease is asymptomatic. As the cyst continue to grow and
expand, necrosis of the infected tissues, accompanied by pressure on such
tissues, usually results. Death may also result due to direct rupture of hydatid
cyst.
Hydatid thrill in abdominal hydatid cyst indicates the presence of fluid which is
a diagnostic sign.
Imaging Techniques:
X-ray, U.S., C.T. and MRI.
X-ray useful in detect the calcified cyst. Various types of scanning procedures or
US examination of the liver may detect an uncalcified cyst.
Lab. Diagnosis:
1- Finding of protoscolices, brood capsules in cyst after surgical removal.
2- Finding of hydatid fragments in sputum and urine.
3- Finding of protoscolices in punctured cyst. It is not advised method,
because it is probably may lead to rupture of hydatid cyst.
4- Serological tests: are useful not only for the primary diagnosis but also to
the follow up of patients after surgical or pharmacological treatment or
both.
The choice of serological technique depends primary on its sensitivity and
specificity, these tests include IHA, ELISA, DD (double diffusion).

9
Detection of circulating antigen in serum by ELISA has high specificity 90% but
low sensitivity 43%.
The parasite antigens present in hydatid fluid that have major
immunodiagnostic value in detecting Echinococcus granulosu are arc 5 and
antigen B.
The results of serological tests differ due to the size and position of the
cyst. The sensitivity is higher in liver cyst than in those with lung cyst. The
intact cysts have less ability to induce antibody formation than the rupture cyst.
5 - Casoni intradermal test: used in wide spectrum but recently this method is
not recommended because of its less specificity. It may show as high as 18%
false positive results in uninfected persons. An immediate –ve reaction is a good
evidence of freedom from the disease, but +ve reaction may persist for years
after removal or death of the cyst.
6-PCR
using recombinant DNA antigens is valuable in defining
particular species of E . granulosus .
This has been effectively applied in the control of the disease and
development of an animal vaccine .